
Cough can be both a symptom of an underlying disease and a disease in its own right. In most cases, banal respiratory infections trigger the complaints, which can be treated symptomatically. But a coronavirus infection or another serious disease are also possible causes. If “red flags” are present and cough symptoms persist for more than eight weeks, further investigation is required.
Coughing is a common symptom of viral infections, but also of diseases of the lungs, bronchi and upper respiratory tract such as lung cancer or chronic obstructive pulmonary disease (COPD). With a prevalence of 9-33% in the general population, cough is a common reason for a physician visit, and in fact the most common overall in the United States [1,2]. “Cough is classified according to the duration of the symptom,” explains PD Dr. med. Tsogyal Daniela Latshang, Chief Physician Pneumology/Sleep Medicine, Cantonal Hospital Graubünden [1]. Symptom duration up to 3 weeks is referred to as acute cough, 3 to 8 weeks is referred to as subacute cough, and over 8 weeks is referred to as chronic cough. The intensity and frequency of the symptom cough are subject to strong interindividual variations.
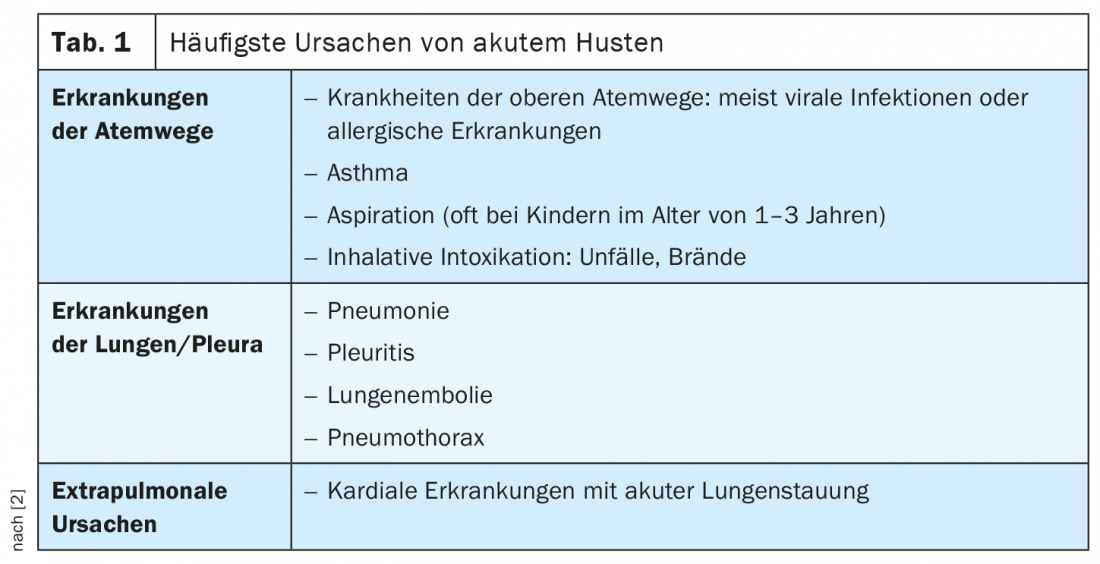
“Common cold” as a frequent cause of acute cough
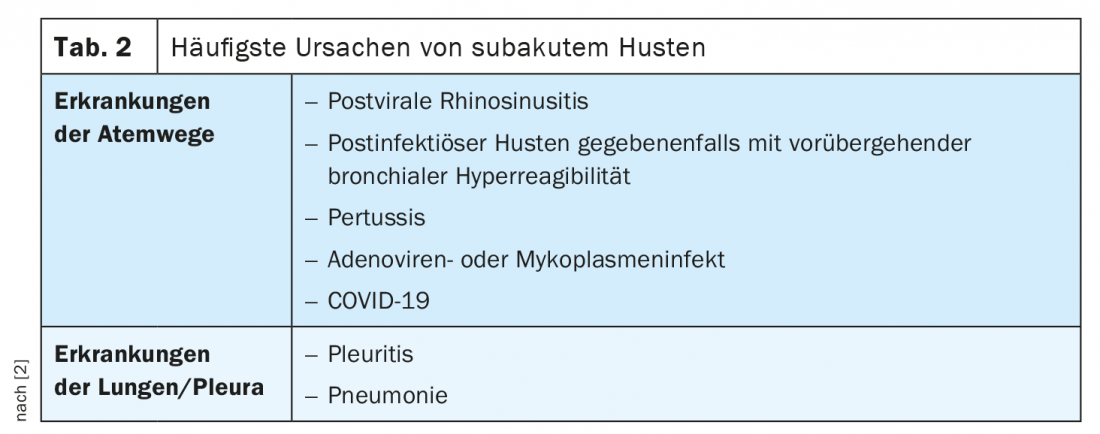
By far the most common cause of acute cough is a viral infection (table 1). Often the causative agent is an influenza virus A or B (influenza) with simultaneous or preceding involvement of the upper respiratory tract: rhinitis, sinusitis, pharyngitis, laryngitis. The spontaneous course of uncomplicated acute bronchitis extends on average over a period of 2-3 weeks. However, after mycoplasma or adenovirus infection, in pertussis, in the development of bronchial hyperresponsiveness, or in delayed healing of acute sinusitis, the cough may persist for up to 8 weeks. In a harmless form of acute and subacute cough, history and physical examination are usually sufficient. For exclusion of SARS-CoV-2 infection, a chest radiograph and a twice-negative polymerase chain reaction (PCR) nasopharyngeal swab are recommended [3].
Symptomatic treatment to alleviate symptoms
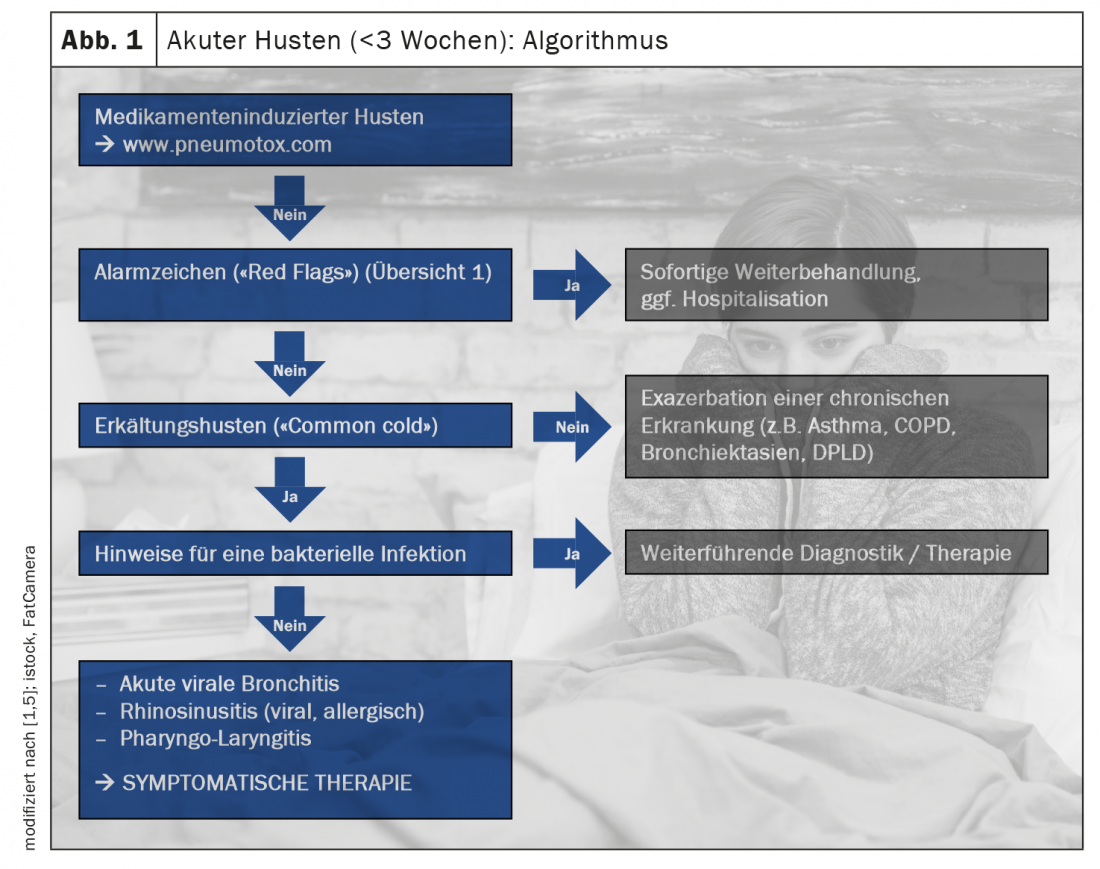
Common cold cough is bacterial in only 3-5% of cases; the vast majority are viral. Antibiotic treatment of acute bronchitis is generally not recommended [2]. Viral cough symptoms are often self-limiting in otherwise healthy individuals, but symptomatic treatment may be useful to reduce distress (Fig. 1). Cold cough is often accompanied by excessive mucus production. N-acetylcysteine is a substance with expectorant effect, which is contained, among others, in the preparation Solmucalm®, in combination with the antihistamine chlorphenamine [6]. As other secretolytic and mucolytic substances characterized by a polyvalent effect (anti-inflammatory, antioxidant, local anesthetic, antiviral) and suitable for short-term treatment, Dr. Latshang mentions the active ingredients dextrometorphan (e.g., Pretuval®, Bexin®, Irotussin®, ephedrine®, Pulmofor®), codeine (e.g. codeine Knoll®, Codicalm®, Resyl plus®, Tossamine®), dihydrocodeine (e.g. Codicontin®, Paracodin®) or guaifenesin (e.g. Resyl®) or the phytotherapeutic Pelargonium sidoides [1,6]. Symptomatic treatment can provide relief from discomfort and a boost to the self-healing powers. There is no evidence-based therapy for the treatment of subacute cough (Table 2); the drugs effective for acute cough can be used [2].
What is important to consider when monitoring cough symptoms?
In what cases is further evaluation of acute and subacute cough indicated? If certain warning signs are present, investigations and, if necessary, hospitalization may be required. These include symptoms such as dyspnea, hemoptysis, high fever, or tachycardia (overview 1) . However, further investigations are also advisable in multimorbid, immunosuppressed, homeless and elderly patients. If cough symptoms persist for a period of 8 weeks, it is advised to immediately perform a chest X-ray in two planes as well as a pulmonary function examination in any case in order not to miss any serious disease [2].

What are possible causes of chronic cough?
In addition to diseases of the respiratory tract or lungs, such as bronchitis, asthma or COPD, extrapulmonary factors are also possible causes of chronic cough. These include gastroesophageal reflux disease (GERD) or certain medications that induce cough irritation (e.g., ACE inhibitors). An overview of other cough-inducing medications is available at www.pneumotox.com. However, cardiac disease and, in rare cases, neuromuscular causes should also be considered [1]. Chronic idiopathic cough can be diagnosed by exclusion diagnosis and treated based on it [4]. In recent years, cough reflex sensitivity has been given more importance. Today, it is assumed that chronic idiopathic and chronic refractory cough can be attributed to hypersensitive cough reflex sensitivity, which is neuropathic in origin and can be treated accordingly, explains Dr. Latshang [1]. For example, the active substances gabapentin and pregabalin are used.
Congress: Medical Congress Davos 2021
Literature:
- PD Tsogyal Daniela Latshang, MD. Cough: What the practitioner needs to know. Medical Congress Davos, 08.-12.03.2021.
- Kardos P: Acute and chronic cough – is there anything new? Pulmonologist (Berl) 2020 Oct 9: 1-9.
- Arévalo Ruales K, et al: Cough in corona times. Z Rheumatol 2021; 80: 270-273.
- Kardos P, et al: S2k guideline of the German Society of Pneumology and Respiratory Medicine on the diagnosis and treatment of adult patients with cough, 2019. AWMF Registry No.: 020-003. www.awmf.org, (last accessed Apr 21, 2021).
- Kardos P, et al: German Respiratory Society guidelines for diagnosis and treatment of adults suffering from acute, subacute and chronic cough. Respir Med 2020; 170: 105939.
- Swissmedicinfo, www.swissmedicinfo.ch, (last accessed 21.04.2021).
HAUSARZT PRAXIS 2021; 16(5): 44-45 (published 5/5/21, ahead of print).









