One advantage of ultra-high-field (7T) MRI is high-resolution imaging due to an increased signal-to-noise ratio. This is of particular interest for functional MRI and spectroscopy. However, in clinical application, 7T MRI is still the exception and evidence of efficacy has been limited to single diseases.
Since the introduction of MRI in the early 1980s, this technology has become extremely important, especially in central nervous system (CNS) diagnostics, neuroscience research, and clinical applications for neurological diseases. Since the resolution of the tissue structures depends strongly on the signal that can be received and this in turn on the field strength, higher and higher field strengths have been developed over the years for human applications. Today, the 3 Tesla (T) system is the upscale standard in routine clinical practice, although the new 1.5 T MR scanners continue to have their place due to advancements in coils and sequences. With higher field strengths, such as 7T, further improvements in signal-to-noise ratio (SNR) and thus image resolution can be achieved. It is also possible to generate new tissue contrasts. On the other hand, higher field strength also increases the problems with artifacts, especially dephasing and ghosting. This article reviews the current state of 7T MRI imaging from the perspective of its potential clinical use, weighing its benefits and limitations.
Benefits and challenges
Meanwhile, some 7T MRIs are available for research but also for clinical applications. The predictions were that the higher SNR would make it possible to image even very small anatomical structures, as well as functional and metabolic examinations and thus further analysis, especially in neurological disease patterns, with previously unattained accuracy. Some neurological conditions expected to gain information were epilepsy, brain tumors, multiple sclerosis, and Alzheimer’s disease. However, the higher field strength due to new contrasts and increased artifacts is also a challenge, so the hardware and software also had to be further developed. Progress was made in this area primarily through the development of new coil technologies [12].
At the beginning, it was not clear whether the higher field strengths (in addition to the imaging limitations) could also lead to increased physiological reactions in the subjects. Meanwhile, some studies have shown that apart from a transient increased sensation of dizziness when entering the magnet, there were no increased sensations or side effects [22]. Thus, in principle, no restriction in the use of 7T MRIs is to be expected from this aspect. However, high examination costs remain as well as somewhat longer examination times compared to the other devices.
Neurological diseases with possible benefit at 7T.
Brain regions near the air-filled osseous structures of the skull base are challenging due to increased dephasing artifacts, especially at 7T. However, this region, including the hippocampus, represents an important structure in the clarification of previously cryptogenic epilepsies, among others. Optimized proton-weighted (PD), T2 and T2* sequences, as well as T1 MPRAGE with isotropic resolution of 0.5 mm were able to overcome these limitations due to increased artifacts and resulted in very high-resolution images in vivo with reasonable measurement time [21]. This enabled accurate and individual anatomical imaging in vivo, with improved detectability of very small pathologies in epilepsy or even Alzheimer’s dementia, which were previously impossible to image up to 3T [4]. In other brain regions, the significantly increased “in-plane” resolution due to the higher SNR may also contribute to improved visualizations of cortical pathologies. In individual cases, this may lead to a change in the therapeutic approach when a previously “cryptogenic” epilepsy becomes one with a detectable focus [25].
Improved imaging of certain typical tissue properties (e.g., iron imaging) at 7T has also been achieved in some degenerative diseases. This now has a place in multimodality imaging analysis in Alzheimer’s disease, Parkinson’s disease, and multiple sclerosis. For example, in Parkinson’s disease, increased iron deposition is found in some brain structures (basal ganglia) and is associated with progressive disease progression, optic and cerebellar atrophy, dystonia, and spasticity. In PD, “susceptibility weighted imaging” (SWI) at 7T has also been used in recent years and changes in the substructure of the substantia nigra have been described. There was an increase in the susceptibility of the pars compacta compared with controls. However, there are differences not only in iron content, but also in substructure representation, such as nigrosome 1 [2]. If in the meantime even with optimized sequences and device hardware some changes at 3T can be displayed [3], the resolution at 7T remains advantageous for special questions. Differentiation of different disease courses and subgroups as well as prodromal diseases (among others sleep disorders) can be done more reliably at 7T than at 3T [5]. Decreased iron deposition can also be detected in other diseases at 7T, e.g., in restless legs syndrome in the thalamus and nucleus dentatus, which apparently gives this disease similarities to periodic trunk movement, which was not previously known in this way [13].
For another degenerative disease, Alzheimer’s disease, improved imaging of substructures such as cortical plaques has been demonstrated. In addition, the improved resolution of the hippocampus mentioned above was also beneficial in diagnosis assignment. Nearly all subunits of the hippocampus as well as the entorhinal cortex show volume reduction on 7T high-resolution images, even compared to “Mild Cognitive Impairment” (MCI) patients [27].
Nowadays, advanced diagnostics in MRI are not limited to purely structural images, but often include metabolic and functional sequences. One sequence that benefits greatly from ultra-high field strength is MR spectroscopy. The clinical applications are, in addition to the differentiation in brain tumors or metabolic diseases traditionally already well established at 3T, in the 7T application to detect also changes in more subtle metabolites, e.g. in amyotrophic lateral sclerosis. Especially for small, rather less stable metabolites, 7T MRI is of clear advantage [19], this also applies to imaging in patient groups with metabolic diseases, where even less prominent metabolites become reliably detectable.
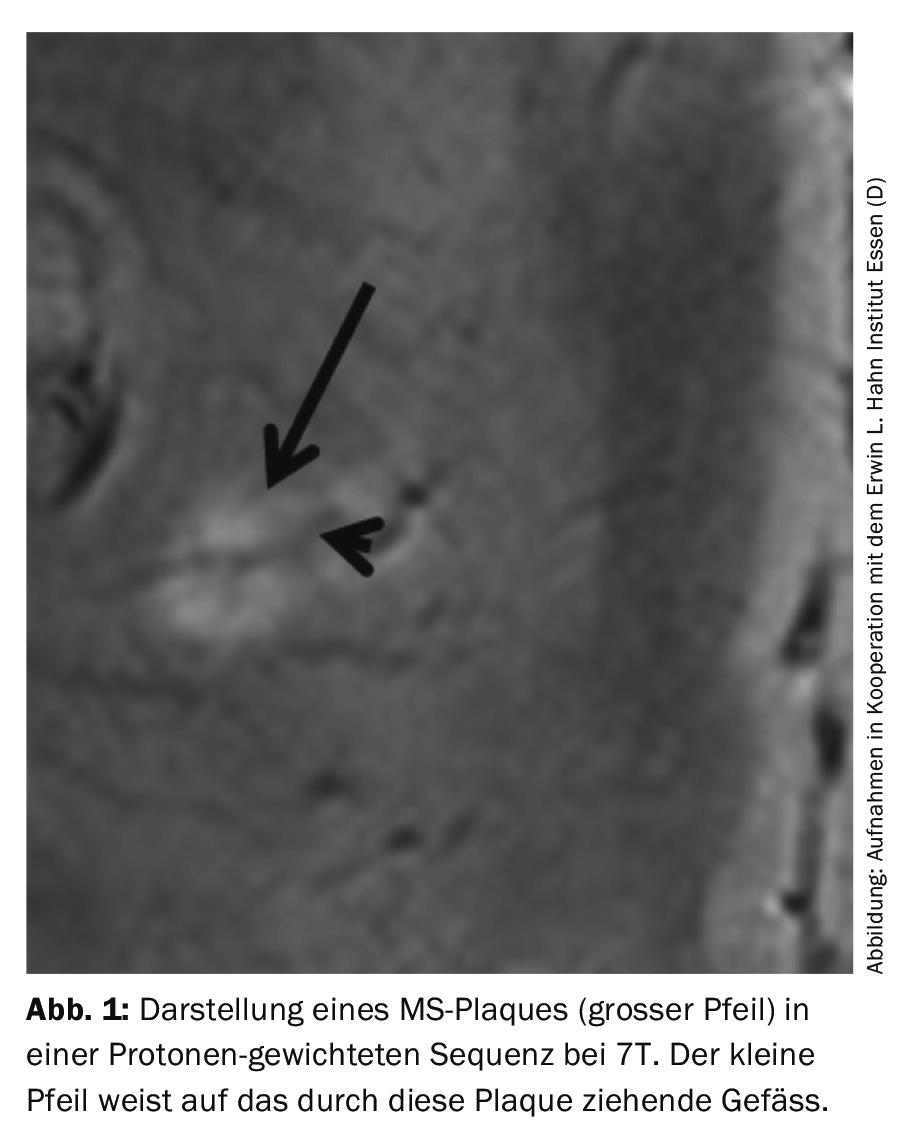
MRI is now the gold standard for diagnosing multiple sclerosis (MS). Nevertheless, patients with the so-called “Clinically Isolated Syndrome” (CIS) with absent correlate at 1.5 and 3T are found again and again. The further increased SNR at 7T also leads to the detection of very small lesions in this disease, e.g., even intra-cortical [8,11]. In addition, the typical structure of MS lesions cerebrally could be visualized for the first time in almost histological resolution in vivo (Fig. 1) and a differentiation between MS and neuromyelitis optica could be achieved [18]. Further development of phase contrast imaging also improved the differentiation of acute and chronic lesions, and quantitative methods (e.g., R2* mapping) or new sequences such as the double inversion recovery (DIR) sequence have been established [9]. In times of debate whether the MRI contrast agent can really be further classified as safe, such an alternative could become of greater importance in follow-up studies. In the group of CIS patients, an optimized 7T protocol that also includes SWI mappings can detect already subtly increased iron deposition in addition to small plaque deposition.
Vascular pathologies and high-resolution imaging.
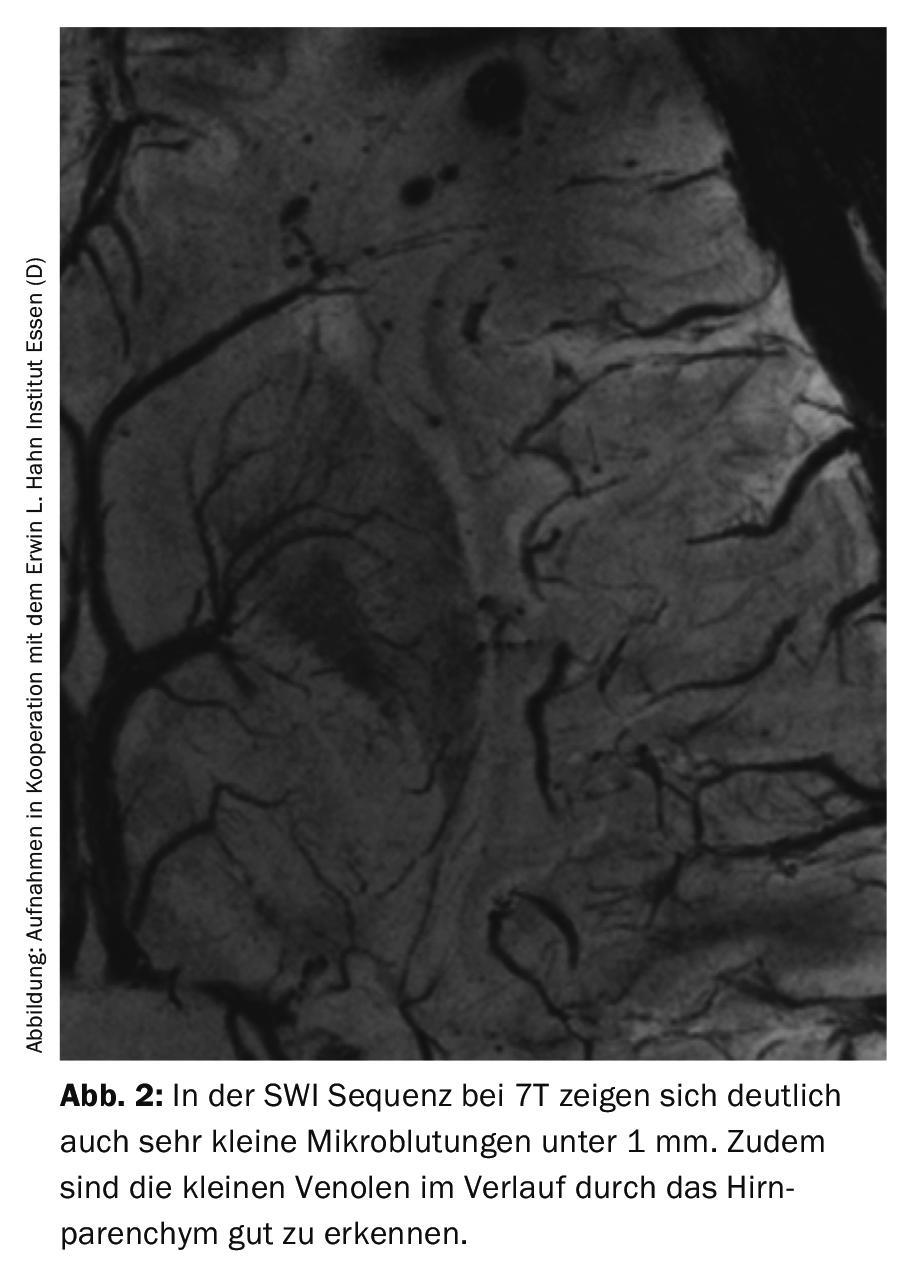
Due to the higher resolution and also higher sensitivity to artifacts, one sequence in particular benefits in the visualization of even very small hemosiderin deposits, namely the SWI at 7T [20] (Fig.2). In addition to the question of microbleeds in vascular disease, high-resolution imaging in the T2 and FLAIR sequences may also be helpful, e.g., to detect microinfarcts, which can occur in intracerebral hemorrhage and appear to be more common than previously thought, as these were often not seen by 3T [24].
In addition, imaging of intracerebral vessels also benefits from the high resolution at 7T with unprecedented accuracy. Thus, the lenticulostriate arteries can also be visualized very well with this. An interesting observation here was that these arteries differ significantly in hypertensive subjects compared with control subjects-also an observation that was not previously possible and may contribute to our understanding of the development of microangiopathic lesions [10]. In the meantime, it has also become possible to image the vessel walls of the intracranial vessels in high resolution [26]. New contrasts were also interesting, such as the ability to generate vascular images intracranially using MPRAGE (magnetization-prepared rapid gradient-echo) without contrast agent instead of time-of-flight MRA (TOF MRA) [15]. A potential clinical application of optimized TOF MRA is the reliable visualization of intracranial aneurysms even below 3 mm. Here (with further spread of 7T MRIs) the benefit would be given to diagnose patients reliably and safely even without invasive angiography [17].
The improved visualization of microbleeds with higher sensitivity in SWI at 7T is not only helpful in the search for amyloid angiopathies. Increased tumor vascularization, micro-metastases in melanoma, and small axonal damage after trauma or microhemorrhages as a result of radiation can also be visualized with higher sensitivity [1,16]. Imaging in cavernomas can be helpful here both in the detectability of very small further cavernomas (e.g., in the case of an incidentally discovered “developmental venous anomaly” [DVA]), but also in the better resolution of the internal structures of a cavernoma.
Clinical functional MRI (fMRI).
3T-fMRI is currently the standard in experimental studies but increasingly also in clinical applications. This method, due to the already higher SNR compared to 1.5 T, is a very good method to improve the otherwise very low signal in fMRI and thus obtain more valid results with acceptable susceptibility artifacts. However, the clinical application remains limited by the still low signal and the requirement to obtain results reliably at the single-subject level (the individual patient). This problem can be at least partially overcome by even higher field strengths (albeit with the disadvantage of increased artifact susceptibility). After initial studies demonstrated the benefit of 7T-fMRI also when applied to the whole brain [6], further optimizations were achieved, even replacing the otherwise common block-design measurement with a “single-event” measurement. Further studies followed, further confirming and expanding the utility of 7T MRI, particularly in clinical applications.
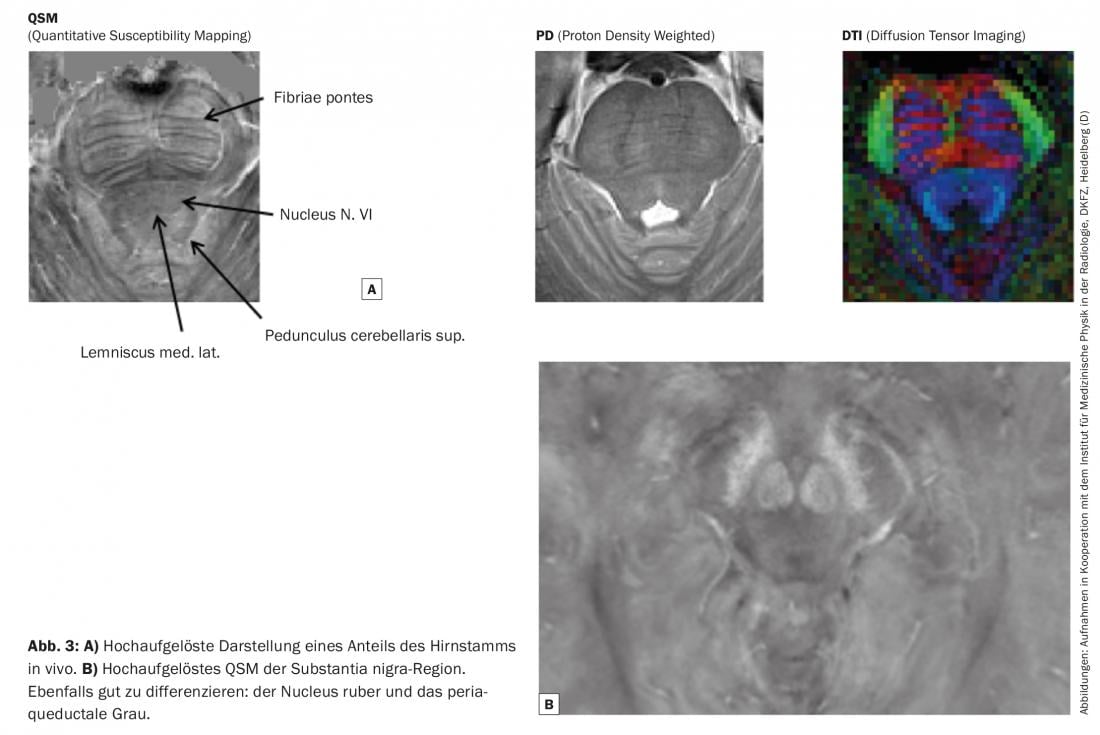
In particular, techniques have been developed that have been able to reduce the artifacts in ultra-high-field imaging, which are highly emphasized in echoplanar imaging in particular [14]. Ultra-high field also allows for much higher resolution mapping of motor regions, which may have advantages in pre-surgical assessment. In addition, deep brain structures that were more difficult to image in activation at lower field strengths could be reliably activated at 7T: for example, the dentate nucleus in a verb generation task [23]. Optimizing the representation of brainstem function and substructure also belongs to this field of application. Here, many central functional units that play an important role in pain disorders, for example, are densely packed. With the higher SNR, it is now possible to visualize these substructures as well [7] (Fig. 3) . However, the actual clinical benefit still has to be demonstrated in the near future.
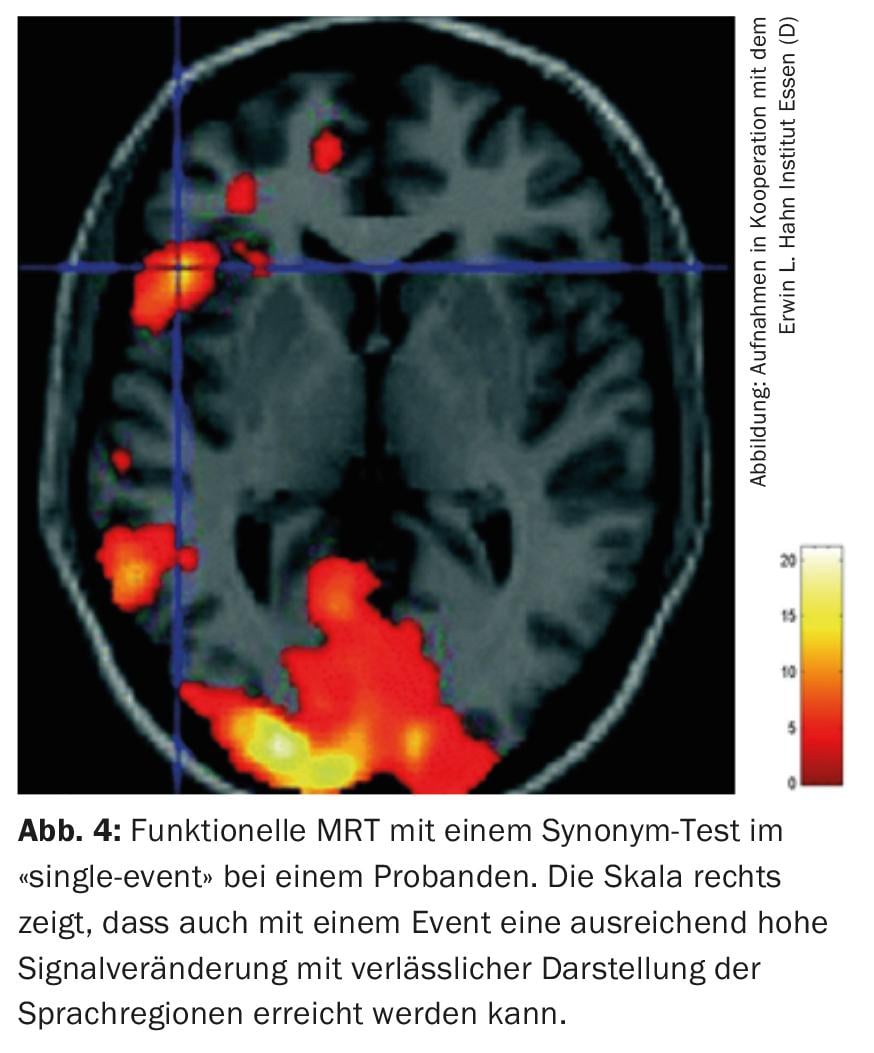
Therefore, in addition to the clear benefits of ultra-high field MRI, especially in functional applications in the cognitive sciences, clinical applications also benefit from the higher field strength. Due to the above-mentioned possibility of also performing “single-event” measurements, fMRI measurements are possible pre-surgically even in patients who are already partially limited in the function to be examined (motor function or speech) (Fig. 4). A single measurement is usually still feasible, but multiple “on-off” measurements are often excessive.
Conclusion
Overall, 7T MRI is still the exception in clinical use. Even though many limitations due to artifacts and altered image impressions have been improved by new developments, the clinical benefit has only been reliably proven in some diseases so far and even then mostly limited to some subgroups (certainly also due to the still high costs and thus still low diffusion of 7T MRIs). However, in these selected groups, the new information from the 7T recordings may well lead to changes in treatment regimens. More common, however, is the benefit in some central nervous system diseases from new in vivo insights into the underlying pathomechanisms.
Take-Home Messages
- Magnetic resonance imaging (MRI) is one of the most important methods in the diagnosis and treatment of many diseases. The high clinical standard today is a field strength of 3 Tesla (T).
- Ultra-high-field MRI (mostly 7T) already offers clinical perspectives, as outlined in this article, but currently has some problems and limitations.
- The significantly increased signal-to-noise ratio (SNR) reveals advantages in high-resolution, almost histological imaging of some brain structures and pathologies.
- Functional MRI (fMRI) and metabolic studies (MR spectroscopy) particularly benefit.
Literature:
- Bian W, et al: Susceptibility-weighted MR imaging of radiation therapy-induced cerebral microbleeds in patients with glioma: a comparison between 3T and 7T. Neuroradiology 2014; 56(2): 91-96.
- Blazejewska AI, et al: Visualization of nigrosome 1 and its loss in PD: pathoanatomical correlation and in vivo 7T MRI. Neurology 2013; 81(6): 534-540.
- De Marzi R, et al: Loss of dorsolateral nigral hyperintensity on 3.0 tesla susceptibility-weighted imaging in idiopathic rapid eye movement sleep behavior disorder. Ann Neurol 2016; 79(6): 1026-1030.
- Derix J, et al: Visualization of the amygdalo-hippocampal border and its structural variability by 7T and 3T magnetic resonance imaging. Hum Brain Mapp 2014; 35(9): 4316-4129.
- Frosini D, et al: Seven tesla MRI of the substantia nigra in patients with rapid eye movement sleep behavior disorder. Parkinsonism Relat Disord 2017; 43: 105-109.
- Gizewski ER, et al: fMRI at 7T: whole-brain coverage and signal advantages even infratentorially? Neuroimage 2007; 37(3): 761-768.
- Gizewski ER, et al: High-resolution anatomy of the human brain stem using 7-T MRI: improved detection of inner structures and nerves? Neuroradiology 2014; 56(3): 177-186.
- Harrison DM, et al: Thalamic lesions in multiple sclerosis by 7T MRI: Clinical implications and relationship to cortical pathology. Mult Scler 2015; 21(9):1139-1150.
- Inglese M, et al: Clinical applications of ultra-high field magnetic resonance imaging in multiple sclerosis. Expert Rev Neurother 2018; 18(3): 221-230.
- Kang CK, et al: Hypertension correlates with lenticulostriate arteries visualized by 7T magnetic resonance angiography. Hypertension 2009; 54(5): 1050-1056.
- Kollia K, et al: First clinical study on ultra-high-field MR imaging in patients with multiple sclerosis: comparison of 1.5T and 7T. AJNR Am J Neuroradiol 2009; 30(4): 699-702.
- Kraff O, Quick HH: 7T: Physics, safety, and potential clinical applications. J Magn Reson Imaging 2017; 46(6): 1573-1589.
- Li X, et al: Brain iron deficiency in idiopathic restless legs syndrome measured by quantitative magnetic susceptibility at 7Tesla. Sleep Med 2016; 22: 75-82.
- Lima Cardoso P, et al: The clinical relevance of distortion correction in presurgical fMRI at 7T. Neuroimage 2018; 168: 490-498.
- Maderwald S, et al: To TOF or not to TOF: strategies for non-contrast-enhanced intracranial MRA at 7T. MAGMA 2008; 21(1-2): 159-167.
- Moenninghoff C, et al: Diffuse axonal injury at ultra-high field MRI. PLoS One 2015; 10(3): e0122329.
- Monninghoff C, et al: Evaluation of intracranial aneurysms with 7T versus 1.5 T time-of-flight MR angiography – initial experience. Rofo 2009; 181(1): 16-23.
- Sinnecker T, et al: MRI phase changes in multiple sclerosis vs neuromyelitis optica lesions at 7T. Neurol Neuroimmunol Neuroinflamm 2016; 3(4): e259.
- Terpstra M, et al: Test-retest reproducibility of neurochemical profiles with short-echo, single-voxel MR spectroscopy at 3T and 7T. Magn Reson Med 2016; 76(4): 1083-1091.
- Theysohn JM, et al: 7Tesla MRI of microbleeds and white matter lesions as seen in vascular dementia. J Magn Reson Imaging 2011; 33(4): 782-791.
- Theysohn JM, et al: The human hippocampus at 7T–in vivo MRI. Hippocampus 2009; 19(1): 1-7.
- Theysohn JM, et al: Subjective acceptance of 7Tesla MRI for human imaging. MAGMA 2008; 21(1-2): 63-72.
- Thurling M, et al: Activation of the dentate nucleus in a verb generation task: A 7T MRI study. Neuroimage 2011; 57(3): 1184-1191.
- van Veluw SJ, et al: Cortical microinfarcts on 7T MRI in patients with spontaneous intracerebral hemorrhage. J Cereb Blood Flow Metab 2014; 34(7): 1104-1106.
- Veersema TJ, et al: Seven tesla MRI improves detection of focal cortical dysplasia in patients with refractory focal epilepsy. Epilepsia Open 2017; 2(2): 162-171.
- Viessmann O, et al: T2-Weighted intracranial vessel wall imaging at 7Tesla using a DANTE-prepared variable flip angle turbo spin echo readout (DANTE-SPACE). Magn Reson Med 2017; 77(2): 655-663.
- Wisse LE, et al: Utrecht Vascular Cognitive Impairment Study. Hippocampal subfield volumes at 7T in early Alzheimer’s disease and normal aging. Neurobiol Aging 2014; 35(9): 2039-2045.
InFo NEUROLOGY & PSYCHIATRY 2018; 16(6): 28-33.









