
The musculoskeletal system is the most common source of chronic pain; degenerative wear and tear is the primary cause. If physiotherapy, massage and the whole range of conservative measures show no lasting effect, it must be assumed that the cause of pain is generated by wear and tear of the intervertebral joints in about 60% of cases. The therapeutic approaches are manifold: surgical stiffening of the joints, injection of cortisone into the intervertebral joints, obliteration (radiofrequency lesion) of the nerve branches, or pain treatment with medication. The following is a brief explanation of the radiofrequency (RF) lesioning method.
Breakthrough in 1996
Radiofrequency (RF) lesioning has been used to treat chronic back pain since the mid-1970s. Here, under X-ray control with real-time imaging, a special needle is directed by puncture through the skin (minimally invasive intervention) to the nerve sought, where it is treated with heat (approx. 80 °C) is specifically obliterated. Fluoroscopy, as in cardiac catheterization, is the only imaging technique with real-time imaging; computed tomography is unsuitable for performing the treatment. It was not until 1996 that it was first demonstrated that for successful treatment it is essential that the needle tip be placed parallel to the nerve to create the longest possible contact area. Otherwise, sufficient sclerotherapy cannot be achieved and the procedure fails. Thus, it is clear that only a meticulously precise technique applied by an experienced specialist can be successful. A facet joint is considered to be completely denervated and pain-free when the draining nerve branches (medial branches) have been completely obliterated.
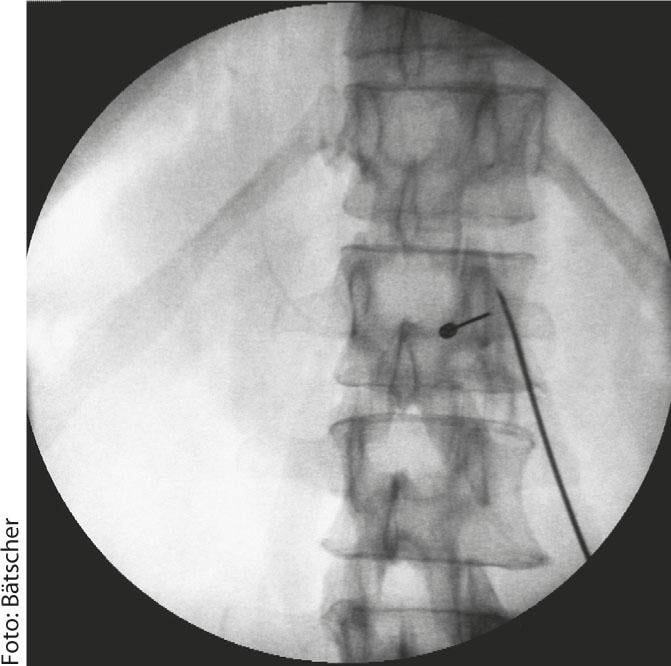
RF at the transition joint on the right between the thoracic and lumbar spine. The long RF needle is parallel to the nerve course, the short block needle is perpendicular to the nerve course as in the diagnostic test.
Prerequisite:confirmed diagnosis
An indispensable prerequisite for significant benefit to the patient is the underlying confirmed diagnosis. In expert circles, this is only considered to be certain if two trial blockades of the nerve branches in question, which are independent of each other in terms of time, have led to as complete freedom from pain as possible by means of targeted injections. All other diagnostic measures, particularly imaging or even clinical examination, may provide clues to the presence of facet joint pain, but correlate poorly with real findings. Nor do they allow any conclusions to be drawn in determining the levels involved.
The following requirements must be met for lasting success in treatment using radiofrequency therapy:
- the diagnosis must be correct;
- the affected vertebral segments must be correctly defined;
- the radiofrequency lesion must be performed in a technically perfect manner; and
- following the completed intervention, the regional musculature should be loosened and strengthened with targeted and professional physiotherapy, because it increasingly hardens as a result of the chronic pain condition and begins to hurt itself.
After completion of the intervention therapy, the task of physiotherapy is to optimize the movement sequence of the involved joint partners with targeted grip techniques and to correct the imbalance between stabilizing and mobilizing muscles by means of targeted exercise selection in order to enable the trunk muscles to be built up.
However, if all these conditions are met, radiofrequency therapy is a good form of therapy for many patients.
Andreas Bätscher, MD









