
Improvements in disease management increase the quality of life and life expectancy of patients with cystic fibrosis. Newborn screening, introduced in 2011, enables early diagnosis. However, the disease should also be considered as a possible differential diagnosis in adulthood.
Cystic fibrosis (CF, sometimes also cystic fibrosis) is the most common congenital, ultimately life-limiting metabolic disease in Switzerland. As a systemic disease, CF primarily affects the function of the exocrine glands of the respiratory and digestive tracts. In particular, the pulmonary course with continuous irreversible destruction of the organ causes the shortened life expectancy. Due to improved medical measures, the affected persons now reach adulthood almost without exception, but thus still represent a relatively new collective in family practice. As a promising innovation, causal therapy has been available for a very small proportion of patients since early 2014.
Disease pattern
As early as 1936, the Zurich pediatrician Guido Fanconi described CF, which at that time was still called by other names, as a fatal disease of small children, which is why access to it remained closed to colleagues in family medicine for a long time.
CF is the most common congenital chronic and ultimately life-limiting hereditary disease with a prevalence of approximately 1:2500. Approximately every 25th person in Central Europe is a healthy mutation carrier. There are about 70,000 people with the disease worldwide, and an estimated 900 in Switzerland. About half of the patients are over 18 years old. The mode of inheritance is autosomal recessive, thus statistically one child out of four children resulting from a relationship of two healthy mutation carriers is affected by CF, two children are like the parents also healthy mutation carriers and one child is neither mutation carrier nor ill. In 1989, the underlying gene was identified on chromosome 7. The cause is a mutation in the CFTR gene (“cystic fibrosis transmembrane conductance regulator”), which codes for the chloride channel in the cell membrane [1,2].
Clinic
In systemic disease, various organs are affected, but usually chronic lung disease leads to increased morbidity and reduced life expectancy. Due to improved medical possibilities, life expectancy has risen continuously in recent years. The average life expectancy in Europe is currently over 40 years and will continue to increase, especially in the generation detected in newborn screening in Switzerland since 2011. Nevertheless, the course of the disease is very inconsistent, and individual patients still die of lung failure in young adulthood. Common to all sufferers are bacterial chronic respiratory infections that lead to irreversible destruction of the lungs. Patients suffer from cough, sputum and an increasing limitation of their physical capacity. Furthermore, chronic diarrhea with maldigestion is found due to exocrine pancreatic insufficiency, which affects approximately 85% of patients. As a result of malnutrition, but also increased work of breathing results in failure to thrive. Around 10% present with meconium ileus after birth, but elders may also suffer from recurrent intestinal obstruction syndromes. Despite optimal symptomatic therapy, liver cirrhosis or endocrine pancreatic insufficiency with development of diabetes mellitus may also occur in the further course of the disease. Male CF patients in particular are frequently affected by infertility [1,2].
Pathophysiology
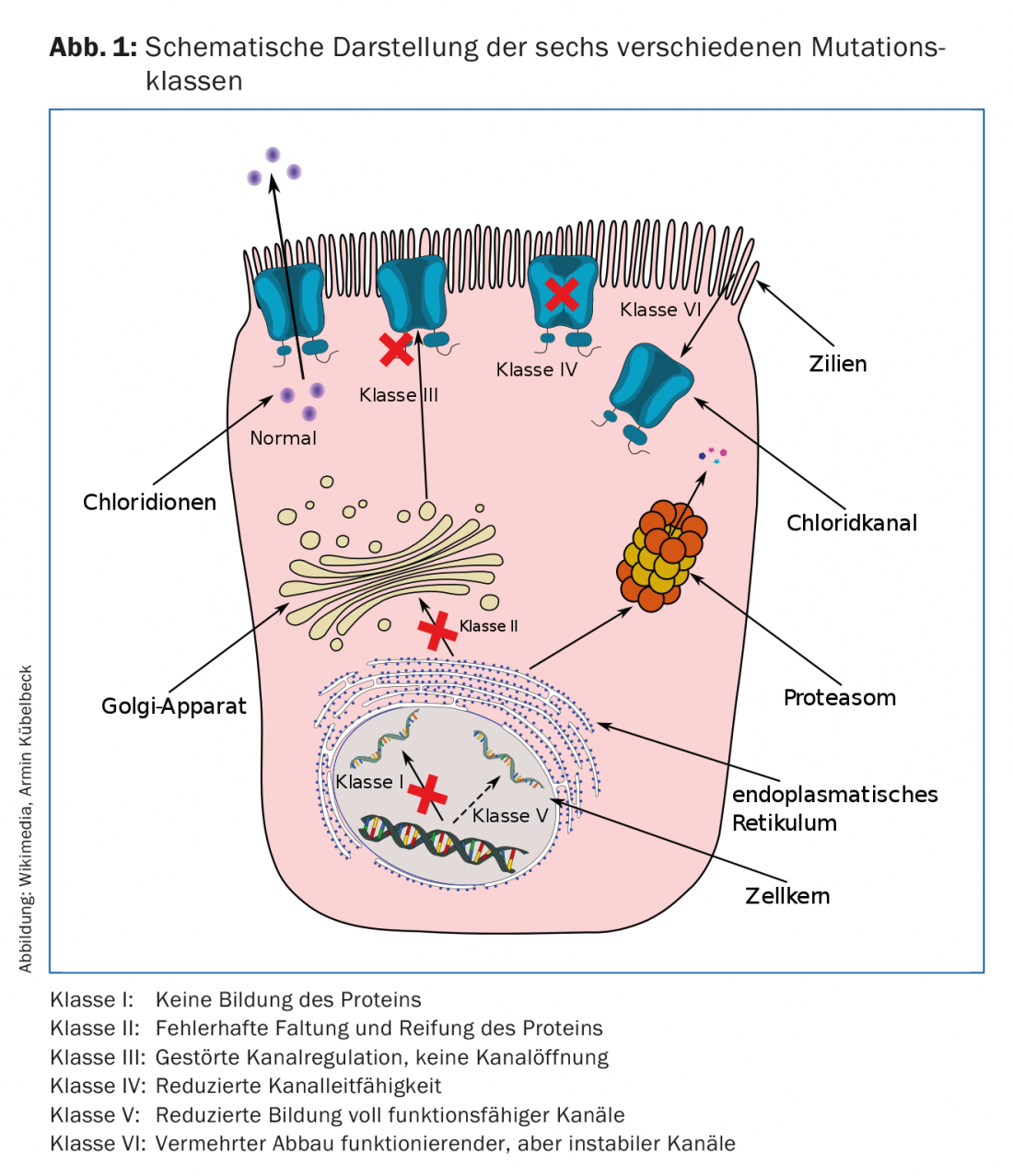
The CFTR gene on chromosome 7 codes for the chloride channel in the cell membrane. Gene mutations, of which more than 2000 are now known but fewer than 200 are clearly disease-causing, cause dysfunction or complete absence of the chloride channel in epithelial cells. Mutations in the CFTR gene are divided into six classes (Fig. 1), which differ in their pathomechanism. For example, some mutations cause an almost complete failure of the synthesis of the CFTR protein. The mutation 3905insT occurring in Swiss or persons of Swiss descent (e.g. Amish in North America) is assigned to this class I and constitutes the second most frequent mutation in Switzerland. In other mutations, the incorporation of the protein into the cell membrane is prevented or the ion channel of the protein is blocked or has only limited conductivity. The most common mutation in Europe, but also in Switzerland (86% heterozygous, 47% homozygous) is assigned to class II and involves a deletion at site 508 (F508del). Produced protein is misfolded here and degraded before any function is taken up. Failure of the chloride channel results in disruption of transepithelial transport in all organs where epithelial cells express CFTR. Using the airway epithelium as an example, an inflammatory cascade results. The increased viscosity of the mucus causes impaired mucociliary clearance, which in turn is associated with early and, in the further course, chronic bacterial colonization. The endogenous immune response causes excessive recruitment of neutrophil granulocytes, resulting in inadequate release of neutrophil elastase and ultimately tissue destruction. In addition to the two classical mutations (F508del, 3905insT), which are responsible for a severe course of the disease, mutations are now also known which are associated with a rather mild clinical course – whereas in the case of other mutations it is unclear whether they cause CF at all. The database www.cftr2.org attempts to provide a continuously updated overview of known CF-causing mutations and their likely phenotypes [1,3,4].
Diagnostics
Prior to 2011, about 10% of ill children were noticed with meconium ileus, but the vast majority were not identified until CF-suspicious symptoms appeared during the course. The gold standard for diagnosis is considered to be the sweat test, i.e. the quantitative determination of the chloride concentration in sweat after pilocarpine iontophoresis. In addition, the measurement of sweat conductivity is also frequently used as a screening test, as this test works quickly and reliably with a significantly smaller amount of sweat. Macroduct® and Nanoduct® are commercially available test systems. For quality assurance, the performance of welding tests should be reserved for appropriate centers.
In 2011, CF was included in the newborn screening program in Switzerland. Immunoreactive trypsinogen (IRT) is measured in heel blood. If the threshold is exceeded, newborns are referred to a pediatric CF center. There, the diagnosis is confirmed or ruled out with sweat tests and, if necessary, further examinations (determination of pancreatic elastase, genetic analysis).
As of 2016, 143 children have been diagnosed with CF through newborn screening. In an estimated total of 900 CF patients, about 15% of all patients could be detected by newborn screening. This value will continue to rise steadily.
However, it is important to note, especially for the primary care physician, that because of the different phenotypes, there may be cases diagnosed in childhood as well as those with a mild course or with measurable residual CFTR function. Accordingly, individuals may not present until adulthood with atypical symptoms such as pancreatitis, sinusitis, nasal polyps, diffuse bronchiectasis, and/or unfulfilled childbearing. Therefore, the general practitioner should also consider CF as a possible differential diagnosis in case of corresponding symptoms [1,5–7].
Therapy and care
According to international guidelines, patients should be connected to specialized centers. Patients are seen at 3-month intervals. Depending on the individual course of the disease, the therapy must be reviewed and adjusted. In addition to the medical history and clinical examination, lung function measurements (depending on the infrastructure, bodyplethysmography, spirometry, N2 multiple-breath washout) and microbiological tests (sputum or throat swab) are part of the routine examinations, which are supplemented at larger intervals by imaging of the lungs and abdomen, blood tests, glucose loadings and bone density measurements. The aim is to detect changes at an early stage so that they can be counteracted and further deterioration prevented.
Basic treatment is complex and includes intensive airway clearance by inhalation and special respiratory physiotherapy (hypertonic saline, rhDNAse if necessary, special “airway clearance technique”), pancreatic enzyme replacement (lipase) and nutritional therapy (substitution of fat-soluble vitamins, high-calorie diet), and aggressive antimicrobial treatment (inhalation and/or systemic application).
Depending on the patient’s age and the accompanying circumstances, continuous and targeted counseling is also required in order to be able to optimally accept the challenges of the disease and its effects on the way of life. In addition to the obvious disease and therapy-related content, the patients (and depending on their age also their legal guardians) also need support in dealing with social, psychological, financial, insurance-related (disability and/or health insurance) issues, in organizing daycare, kindergarten and school attendance, training and career, travel, the parents’ desire to have children again or the adult patient’s own family planning, etc.
The fact that the people concerned are fortunately getting older and older must be additionally taken into account. Suddenly patients, but also treating teams, are exposed to internal problems that arise independently of CF, but influence its course. To meet these demands, a multidisciplinary therapeutic approach is needed, which can only be provided by a CF center [8,9].
Outlook
In 2014, Swissmedic approved the drug ivacaftor (Kalydeco®) for patients with the class III mutation G551D. For the first time, in the few patients with this mutation (approximately 4-5% of all patients worldwide), a causal therapy could be used with a significant increase in chloride channel function, measurable in a marked improvement in sweat test and lung function. Other CFTR modulators are currently being tested. The hope remains that mutation-specific causal therapy will be available to a larger patient population in the future [10].
Take-Home Messages
- Due to improvements in symptomatic therapy and disease management, quality of life and life expectancy are steadily increasing.
- Already today, half of all Swiss CF patients are in adulthood.
- Newborn screening for CF, introduced in 2011, enables early diagnosis. This means that basic therapy can be started even before the first disease-related changes occur.
- Oligosymptomatic and atypical courses are possible. Therefore, CF should also be considered as a possible differential diagnosis in adulthood.
- Clarification and further care should always be done in collaboration with a CF center.
Literature:
- Elborn JS: Cystic fibrosis. Lancet 2016 Nov 19; 388(10059): 2519-2531.
- Zolin A, et al: ECFSPR Annual Report 2014. 2016.
- Hergersberg M, et al: A new mutation, 3905insT, accounts for 4.8% of 1173 CF chromosomes in Switzerland and causes a severe phenotype. Hum Genet 1997 Aug; 100(2): 220-223.
- CFTR2. www.cftr2.org
- Torresani T, et al: Newborn screening for cystic fibrosis in Switzerland–consequences after analysis of a 4 months pilot study. J Cyst Fibros 2013; 12(6): 667-674.
- Newborn Screening Switzerland. www.neoscreening.ch
- Barben J, et al: Newborn screening for cystic fibrosis – a success story. Schweiz Med Forum 2013; 13(49): 1010-1012.
- Smyth AR, et al: European Cystic Fibrosis Society Standards of Care: Best Practice guidelines. J Cyst Fibros 2014 May; 13(Suppl 1): S23-42.
- Elborn JS, et al: Report of the European Respiratory Society/European Cystic Fibrosis Society task force on the care of adults with cystic fibrosis. Eur Respir J 2016 Feb; 47(2): 420-428.
- Ramsey BW, et al: A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. N Engl J Med 2011 Nov 3; 365(18): 1663-1672.
HAUSARZT PRAXIS 2017; 12(11): 31-33









