Variations in cerebral arteries are usually attributed to persistence or excessive involution of anastomotic vessels that are physiologic to the embryo. In most cases, these persistent embryonic anastomoses remain asymptomatic and are detected only by angiography or at autopsy. Occasionally, they may carry an aneurysm or compress a cranial nerve. The rare case of persistent primitive hypoglossal artery is documented below.
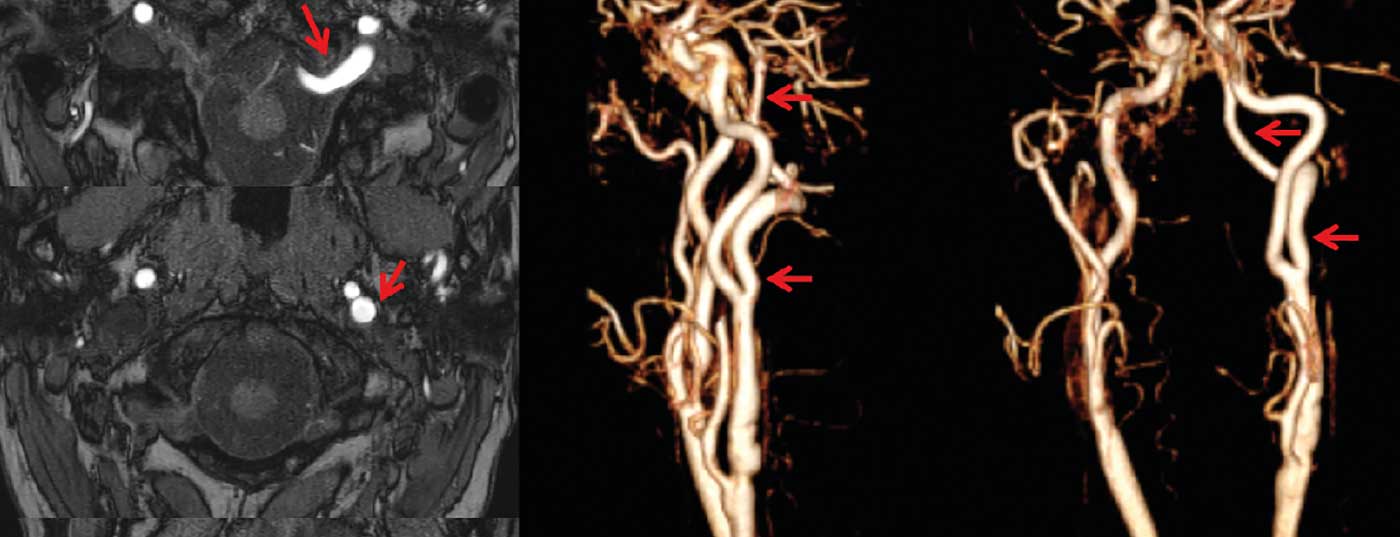
Case description: A 65-year-old female patient underwent KM-guided MR angiography of the brain-feeding arteries as part of the workup for right-sided branch stenosis of the internal carotid artery (ACI). This revealed severe hypoplasia of both vertebral arteries cervically. At the level of HWK1/2, a caliber artery arising from the dorsal circumference of the left distal ACI was detectable. This first ran vental of HWK1 to cranial and then through an enlarged canalis hypoglossi left to intracranial to finally take the course of the basilar artery.
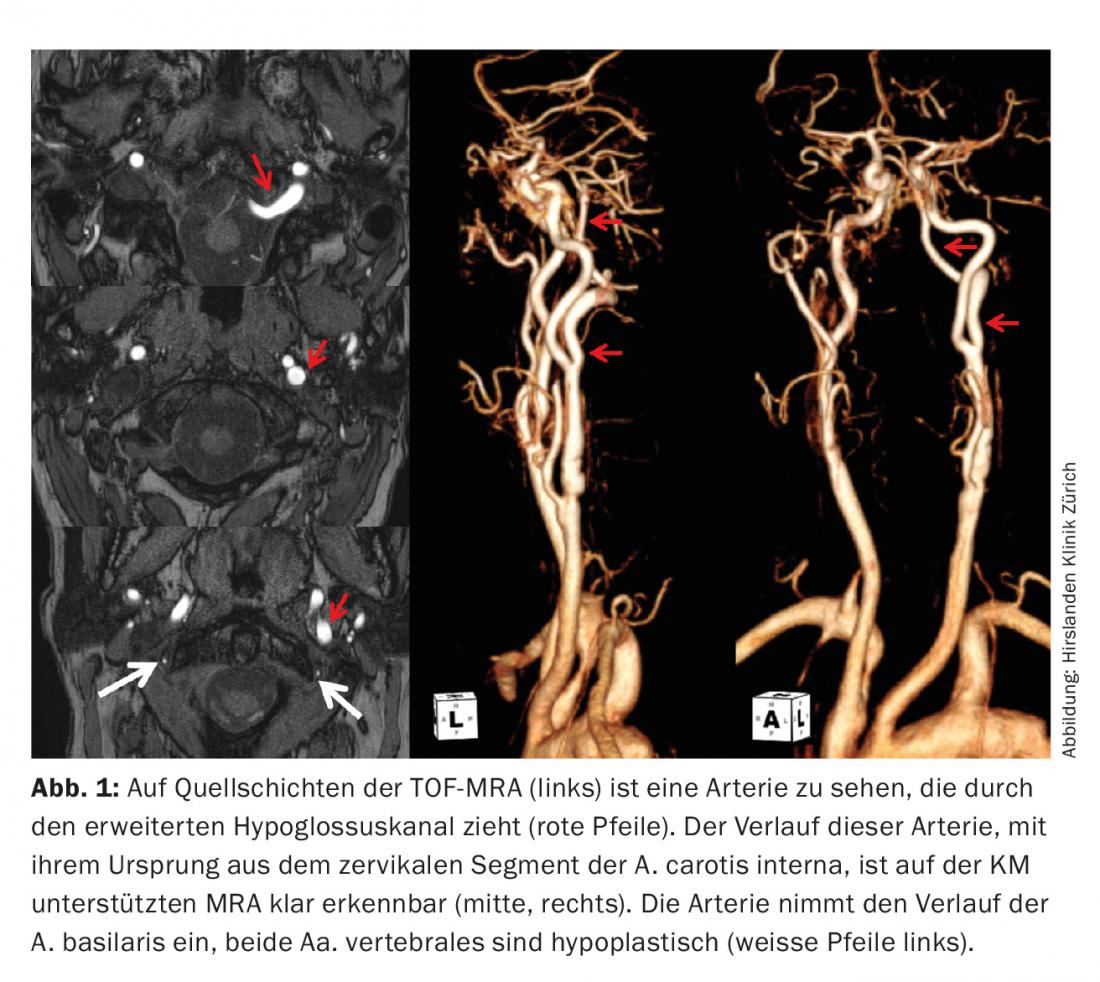
Discussion: The cause of carotidobasilar anastomoses is a lack of obliteration of the embryonic vascular connections between the carotids and the paired neural arteries that later develop into the vertebrobasilar arteries. The trigeminal primitive artery is the most common carotidobasilar anastomosis with a frequency of 0.1-1%. The other anastomoses, the acustica primitiva, the proatlantic artery, and the hypoglossica primitiva presented here are much rarer. With the exception of the A. proatlantica, the designation of the anastomoses follows the nerves they follow. Knowledge of these anatomic variations is of enormous importance for a correct neurovascular workup.
InFo NEUROLOGY & PSYCHIATRY 2016; 14(5): 39.









