
Ovarian cysts are cavities filled with fluid or tissue in the ovaries. They occur in women of all ages, but are particularly common during hormonal fluctuations. If large ovarian cysts burst or rupture, this is often associated with severe pain. Bleeding in the abdomen can also occur, making surgery necessary.
Ovarian cysts are often found as an incidental finding during abdominal imaging examinations.
They occur in pre- and postmenopausal women.
Individual ovarian cysts are usually clinically silent and the risk of malignant degeneration is very low [1].
However, the risk of malignancy in complex cysts and solid tissue proliferations is 23 to 25 times higher.
If ovarian cysts occur frequently in a woman, do not regress or become very large, a gynecological consultation is required [2].
In most cases, ovarian cysts are functional cysts and have hormonal causes that are associated with a disruption of follicular or corpus luteum development.
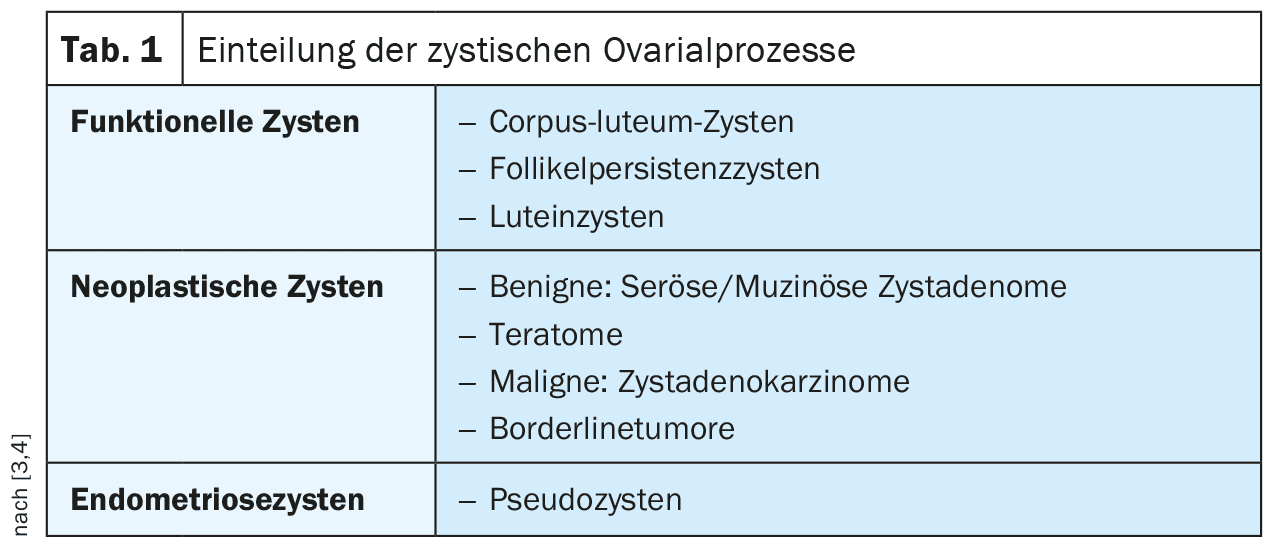
Ovarian cysts are classified according to their dignity [3].
Table 1 provides an overview. Simple cysts are usually asymptomatic.
Complications with lower abdominal pain are common in cases of hemorrhage, cyst rupture, torsion (stem rotation) and breakthrough bleeding.
Acute pain symptoms are then also possible.
Important differential diagnoses, which may also require acute treatment, are listed in Overview 1 .
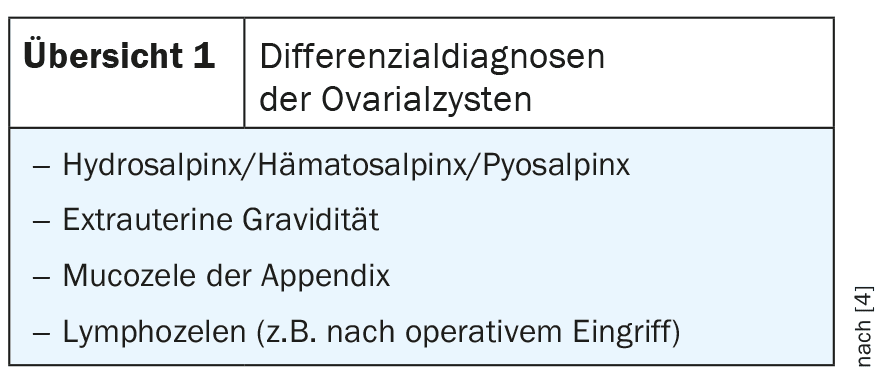
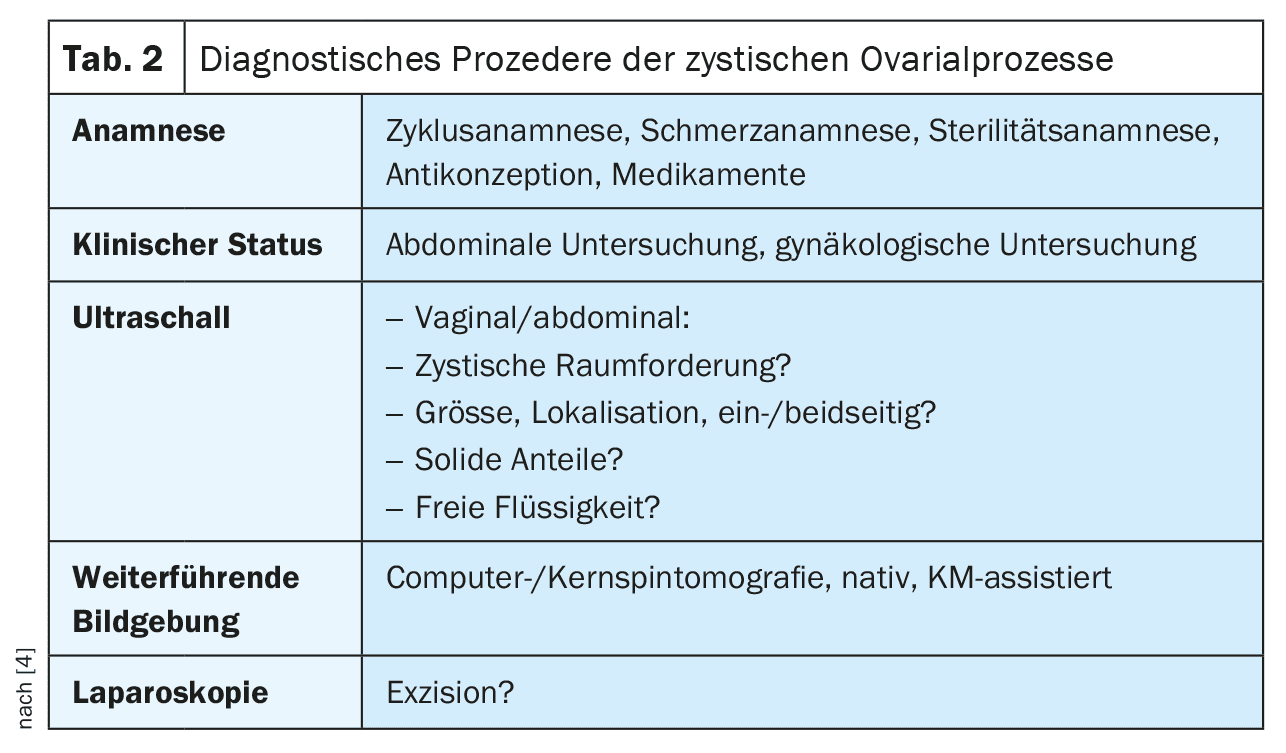
Table 2 summarizes the diagnostic procedure.
Sonographically , the simple cysts are homogeneously echoloculated with dorsal acoustic enhancement. The cyst wall may be delineated delicately. Increased internal echoes, wall thickening or dorsal sound effacement indicate a cyst complication and require further clarification.
It can be difficult to differentiate benign from malignant cystic changes on computed tomography [4]. Functional cysts can appear fluid equivalent, after hemorrhages also with density values above 20 HU. In Stein-Leventhal syndrome, several smaller cysts, usually less than 1.5 cm in diameter, lead to bilateral enlargement of the ovaries.
Magnetic resonance imaging shows ovarian cysts as thin-walled, fluid-equivalent structures with smooth boundaries. The signal intensity is isointense to the urine in all native sequences. They are normally smaller than 4 cm. They can occur solitary, but also bilateral and multiple. If they are larger than 4 cm and show septations, a malignant variant must be ruled out [5]. Hemorrhages lead to signal inhomogeneities of the cyst, stratification in the supine position on examination then occurs, occasionally also a hemosiderin ring with signal reduction. Embryonic remnants of the Wolffian duct lead to cysts in the suspensory ligament of the ovaries (paraöphoron, epoöphoron, Morgagni hydatid).
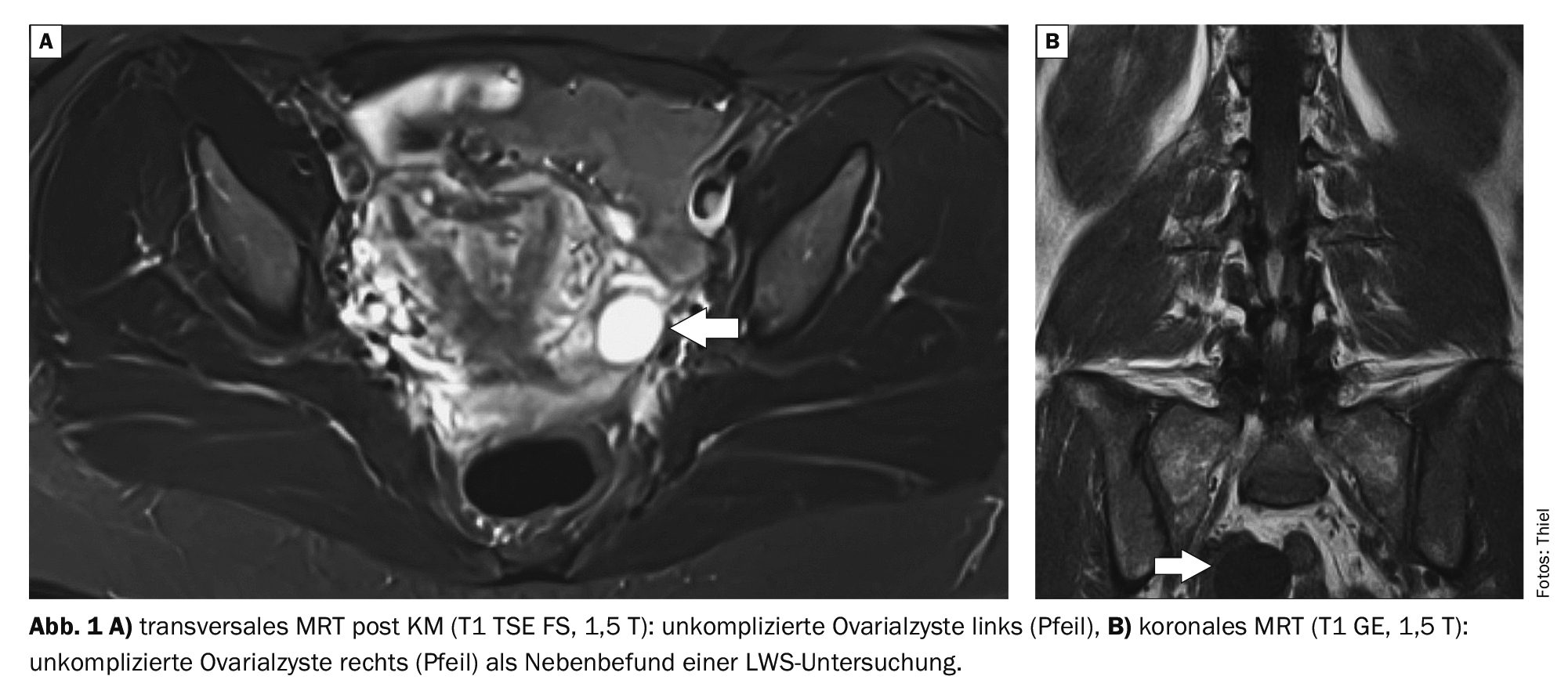
Case studies
In case examples 1 (Fig. 1A) and 2 (Fig. 1B), uncomplicated ovarian cysts can be delineated as incidental findings on magnetic resonance imaging (arrows). They are visualized as homogeneously liquor-intensive.
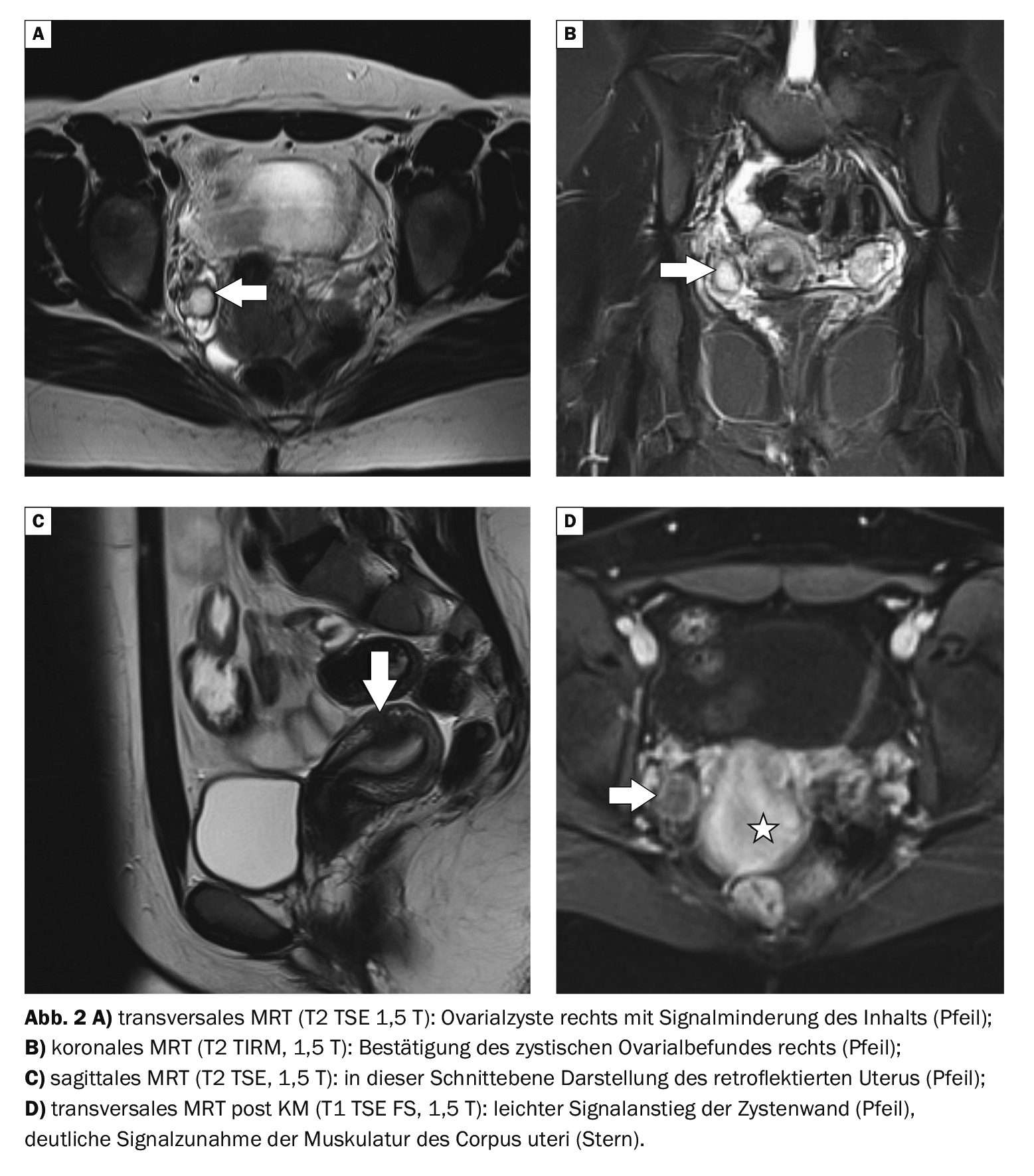
Case 2 (Fig. 2A to 2D) shows an ovarian cyst on the right side on MRI, which indicates hemorrhage with low-signal liquid content. Post contrast medium, there is also a moderate circular signal increase in the cyst wall, indicating an accompanying inflammatory reaction. The patient had increasing lower abdominal pain, right dominant. In addition, a retroflexed uterus was found, which can cause alteration of the sacral plexus.
Case 3 shows a young female patient with undulating pain symptoms in the pelvis on the left with an ovarian cyst with mirror formation as an indication of bleeding that has taken place and is no longer completely fresh (Fig. 3A and B) . The increase in signal in the contrast sequence indicates an incipient fibrous organization of the sedimentation.

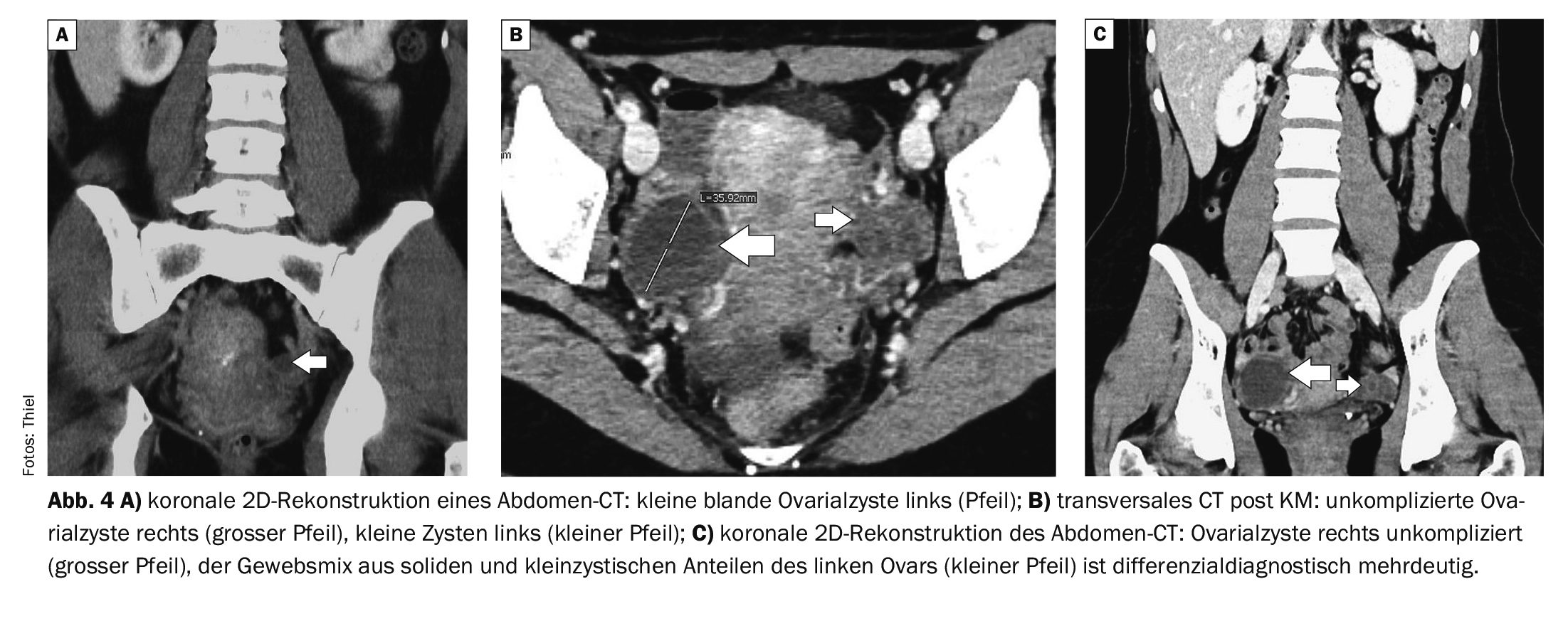
Case study 4 shows an uncomplicated ovarian cyst on the left (Fig. 4A) and ovarian cysts of different sizes on both sides (Fig. 4B and C) in two women between the ages of 40 and 50 in computed tomography scans; there were no relevant symptoms in either case.
Take-Home-Messages
- Ovarian cysts are relatively common and are often discovered as an incidental finding during abdominal imaging examinations.
- If they are uncomplicated and less than 4 cm in size, there are no consequences in the absence of symptoms.
- Cyst complexes, solid parts and conspicuous contrast medium reactions have a significantly increased risk of degeneration or do not rule out the existing malignancy.
- Surgical removal of this ovarian change is then necessary.
Literature:
- Burgener FA, et al: Differential diagnostics in MRI. Georg Thieme Verlag Stuttgart, New York 2002; 624-625.
- Starostzik C: Carcinoma risk: Simple ovarian cysts on ultrasound are normal findings. Gynecology + Obstetrics 2019; 24, 12.
- Ovarian cysts (ovarian cysts), www.med-specialists.com/behandlungen/
ovariancysts, (last accessed 26.06.2024). - Sarlos D: Benign ovarian cysts, www.ksa.ch,(last accessed 26.06.2024).
- Burgener FA, et al: Differential diagnoses in computed tomography. 2nd, completely revised and expanded edition. Georg Thieme Verlag Stuttgart, New York: 2013; 890.
FAMILY PHYSICIAN PRACTICE 2024; 19(7): 39-41









