The use of multigene testing is currently limited to the adjuvant setting in HER2-negative luminal breast carcinoma and allows reproducible predictions of recurrence risk. The tests will lead to fewer chemotherapies in the foreseeable future. However, unnecessary adjuvant chemotherapy can already be avoided with consistent application of the current St. Gallen criteria or ESMO guidelines. Prospective studies involving the OncotypeDX and MammaPrint will be available in the next few years, but do not test these methods against current tools as desired. Molecular test methods should be used for the approval resp. reimbursement be subject to the same criteria and requirements as medicines. Cost coverage by health insurers obliges critical use without extrapolations to untested situations: In low-risk women or clear contraindications to chemotherapy, it should be omitted.
A meta-analysis based on data from 6200 breast cancer patients failed to show a survival benefit from adjuvant high-dose chemotherapy with autologous stem cell transplantation [1]. At Inselspital, eleven patients were treated in this way from 1997 to 1999 as part of the IBCSG-15-95 study. The editorial on the meta-analysis points to current knowledge on biology that would lead to effective and less risky treatments. The final sentence “We remember with gratitude those women who willingly enrolled onto the clinical trials that provided us these gains” shows that the efficacy of chemotherapy was overestimated and that a change of heart has since taken place. In the meta-analysis, the publication year is surprising: 2011. This is because data from approximately 100,000 women with breast cancer show that adjuvant chemotherapy reduces recurrences by 8%, breast cancer mortality by 6.5%, and all-cause mortality by 5% over ten years [2]. In the head-to-head comparison allowed here, tamoxifen is more effective, reducing recurrence risk by 13.2% over 15 years, breast cancer mortality by 9.2%, and all-cause mortality by 9.5%. However, the greater effect is reserved for patients with hormone-sensitive tumors [3].
Intrinsic breast cancer types and surrogate markers.
Gene expression profiling identified four groups of breast carcinoma with different clinical course and response to therapy (“intrinsic subtypes”) over ten years ago:
- Hormone receptor (HR)-positive tumors with low aggressiveness (Luminal A).
- HR-positive tumors with higher aggressiveness (Luminal B).
- HER2-positive tumors (HER2+)
- HR- and HER2-negative carcinomas with or without basal cell characteristics (basal- and normal-like, triple-negative) [4].
Later analyses showed that the four groups simplify reality. The most heterogeneous group is the Luminal A type with relative chemotherapy resistance [5,6]. It must be immediately specified that these methods used several thousand genes and should not be confused with the multigene tests discussed here. Since the former are not routinely available, surrogate definitions were sought (Table 1).
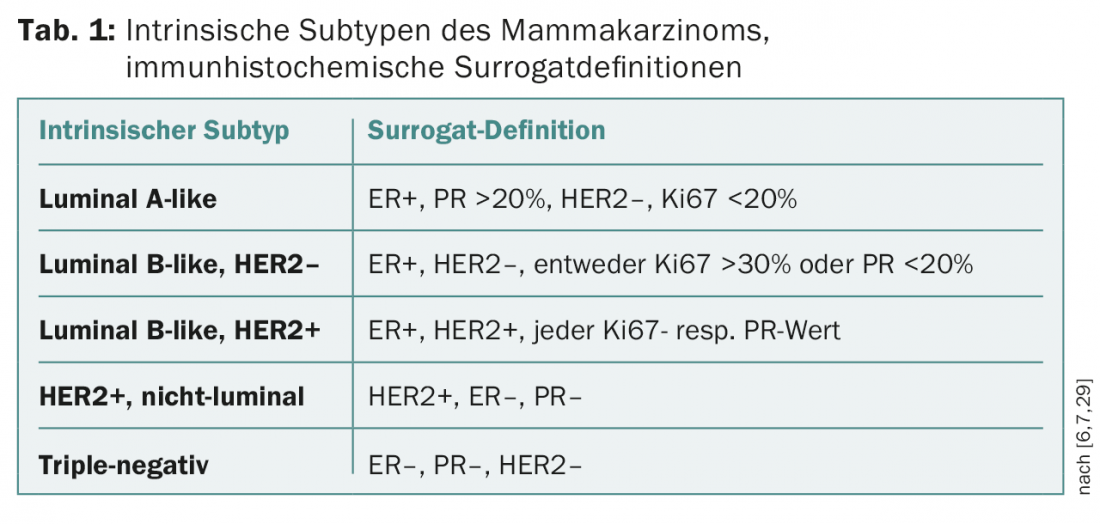
Intrinsic breast carcinoma subtypes, based on the determination of estrogen (ER) and progesterone receptors (PR), proliferation (Ki67), and HER2 (immunohistochemistry or FISH), found their way into the St. Gallen Consensus starting in 2011 [7]. Because of the predictive value of response to available therapies (hormone therapy, chemotherapy, and HER2-targeted therapies), these subtypes have since formed the basis for adjuvant therapy recommendations; previously, these recommendations had been based primarily on prognostic assessment with nonbiologic factors (tumor size, number of affected lymph nodes).
The crux of surrogate definition: luminal A and luminal B carcinomas.
A breast cancer patient wants to know whether or not she will benefit from a particular therapy. In contrast to triple-negative and most HER2+ cancers, the question regarding chemotherapy in luminal breast cancer is how to identify affected individuals who will benefit from this therapy – in addition to hormone therapy. Proliferation is a predictive factor and is used to distinguish between luminal A-like and luminal B-like carcinomas (Table 1) . However, proliferation is a continuous variable, which implies a cut-off value in clinical application. After this value for defining Luminal B-like type was 14% in the 2011 St Gallen Consensus (i.e. Ki67 >14% = Luminal B-like), it was raised to 20% in 2013 and to 20-30% in 2015 with 36% of the votes [6]. In the 2015 vote, 20% of those present abstained, and the same proportion of the expert panel denied Ki67 the justification for this distinction [6].
Despite international efforts, the determination of Ki67 has not yet been standardized. Reproducibility could not be improved even after discussions among 15 Swiss pathologists [8]. However, very good agreement was achieved in the low (<10%) and high range (>30%). Ki67 stains cells in the G1, S, G2, and M phases of the cell cycle, which in addition to technical aspects (definition of positivity, selection of tumor fractions) may explain the discrepant results. Despite intensive promotion of commercial multigene assays and the lure of modern techniques, further studies in this field are desirable.
Multigen tests are not comparable
Various tests jumped into this gap with great market potential. They have been mentioned in the St. Gallen Consensus since 2011, and they have already been included in various guidelines. For an overview, please refer to the article by Patrizia Sager, MD (InFo ONKOLOGIE & HÄMATOLOGIE 2/2015). In multivariate models, the tests quantify HR positivity and proliferation.
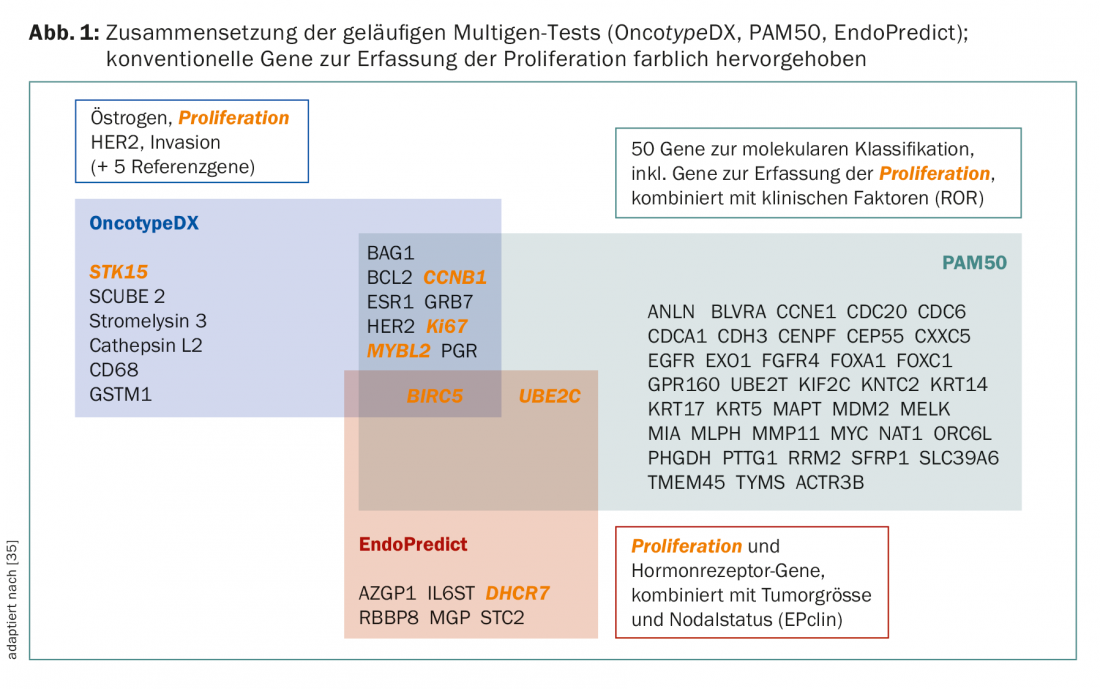
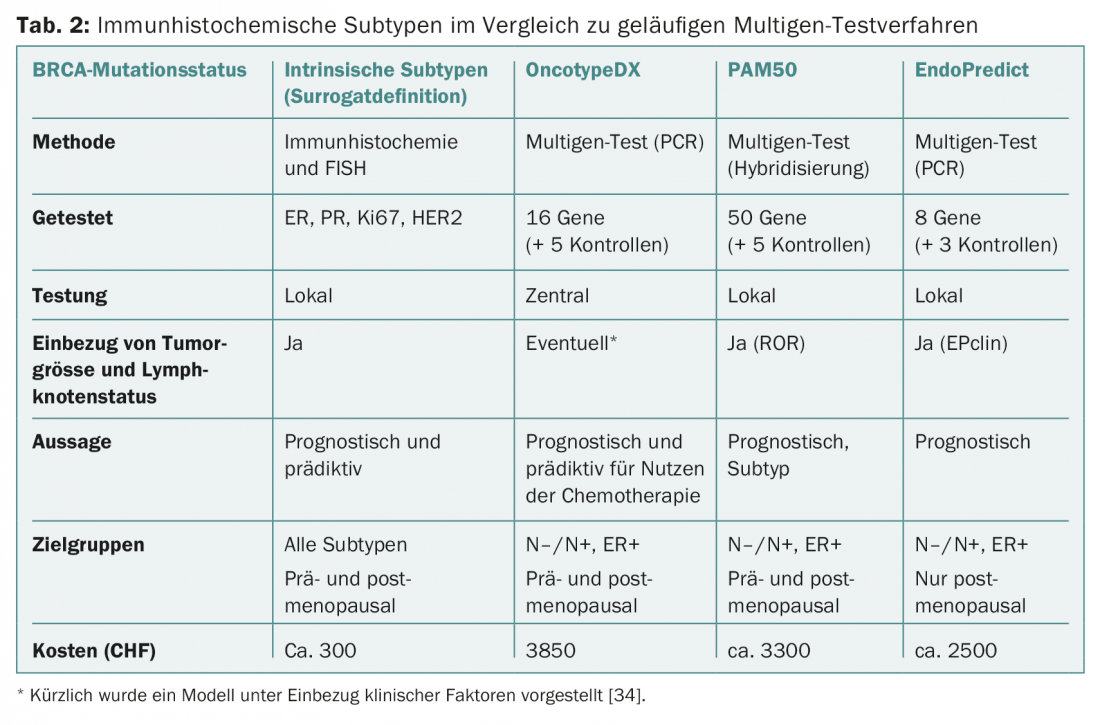
Even if the tests pursue the same goal in principle, they are still not conceptually comparable. There are differences in the gene sets and primary cases for development and validation (Fig. 1 and Table 2) . For example, the PAM50 includes genes for ER+/- cancers and reflects intrinsic types [9], while the OncotypeDX was compiled for predicting chemotherapy benefit in ER+ cancers [10]. MammaPrint measures the risk of recurrence in untreated patients [11,12]. Clinical factors influence the final outcome of PAM50 (as PAM50 ROR) and EndoPredict (as EPclin), diluting the value of “biology”.
Accordingly, the different results in direct (academic!) test comparisons are not unexpected [13–15]. The risk detected by a test is also a continuous variable, which has proven to be a stumbling block in immunohistochemistry.
Multigene tests: prognostic and/or predictive
Prognostic markers, independent of treatment, predict disease progression. Predictive markers indicate whether a treatment will be successful or not. Some factors are prognostic and predictive; in the case of HER2, the availability of specific drugs later disappeared the prognostic value [16]. That procedures in ER+/HER2- breast carcinoma use ancillary information such as tumor size and degree of differentiation to elicit the probability of recurrence is generally accepted. First-generation tests (OncotypeDX, Mammaprint, Genomic Grade Index) can predict relapse in the first five years. The newer methods (PAM50, EndoPredict, Breast Cancer Index) perform better for predicting recurrence at five years, which is relevant because of longer hormone therapies [17–19]. Other potential applications of the tests, besides intrinsic type, are prediction of response rate in neoadjuvant therapy [20–22] and, with limited alternatives, risk assessment in precancerous conditions [23].
The OncotypeDX results – in mostly uncontrolled studies – in fewer chemotherapies and causes currently frightened physicians to feel more confident in their decisions [24,25]. The “psychology” of the possibility of using the OncotypeDX in the choice of adjuvant therapies was part of the SAKK 26/10 study; it will predictably show the large influence of the OncotypeDX on decisions [25]. Recently, the PAM50 test was shown to identify nodal-positive patients in whom chemotherapy does not confer benefit [26].
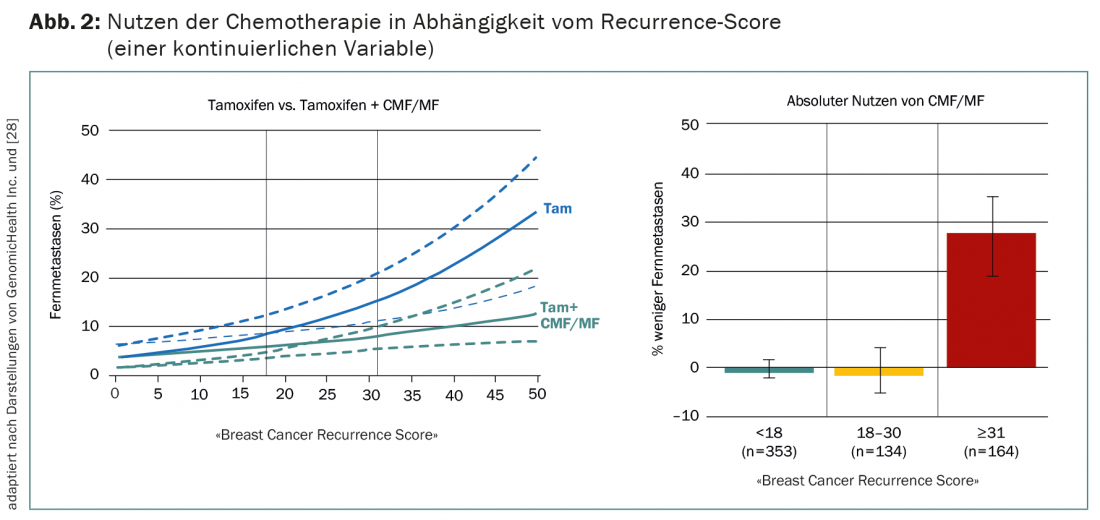
Currently, the most compelling evidence of multigene testing in breast cancer comes from an analysis in node-negative ER+ patients. These were randomized to receive tamoxifen with or without the now rarely used chemotherapy CMF/MF in the NSABP B20 trial [27]. Subsequent OncotypeDX in 651 of the 2299 patients shows that chemotherapy benefits only those with a high probability of recurrence (recurrence score >30) (Fig. 2) [28]. Sensu stricto, this is therefore not a prospective validation, as is often claimed.
Added value of multigene testing?
“Do I need chemotherapy?” With this rhetorical question the commercial tests advertise e.g. with the following case study on the website: 1.8 cm invasive ductal carcinoma in a postmenopausal woman, N0, G2, ER 90%, PR 40%, Ki67 15%. The probability of recurrence, expressed as a recurrence score, is low at 13, and the additional benefit of chemotherapy is minimal [28]. Using the current St. Gallen criteria [6] or ESMO guidelines [29], this woman does not require adjuvant chemotherapy in addition to an aromatase inhibitor.
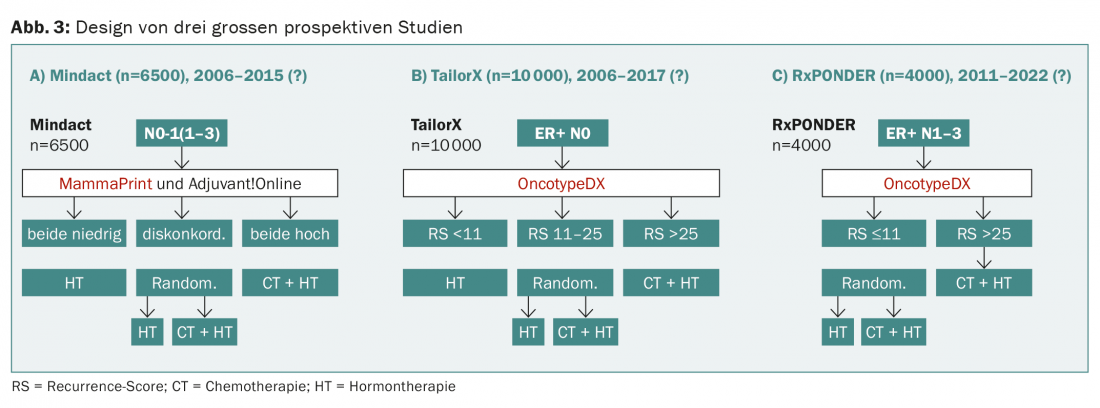
Currently, three large prospective trials (Mindact, TailorX, RxPONDER) are randomized to test hormone therapy vs. combination with chemotherapy depending on the OncotypeDX or MammaPrint result (Fig. 3) .
The prospective WSG-planB trial is comparing two chemotherapies for a recurrence score >11, among others. The design of WSG-ADAPT is interesting: postoperatively, an approach similar to TailorX is followed, but the response to three weeks of hormone therapy is also considered. However, none of these studies “test” any of the tests, as would be required by the ideal study design and is common practice for drugs (Fig. 4).
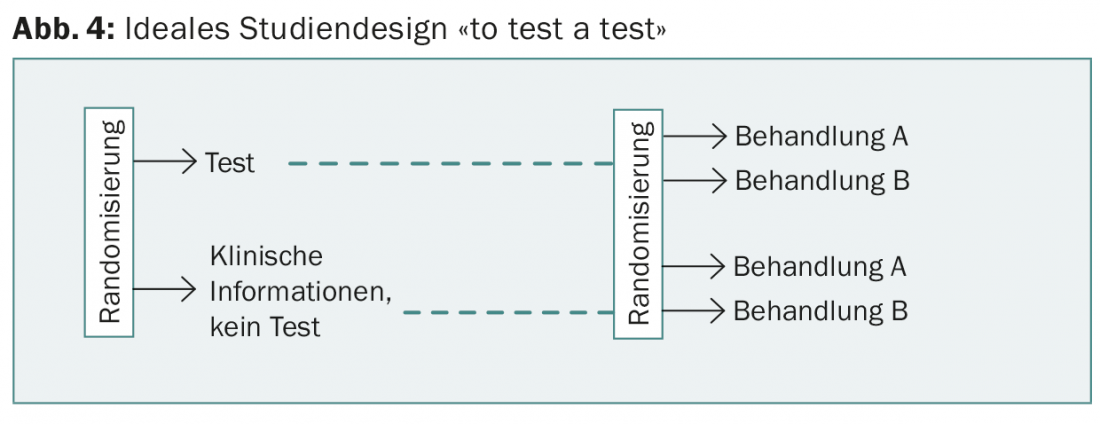
However, this would be necessary to demonstrate the added value of the new tests compared to previous information (including best possible Ki67 determination) and to justify the additional costs. The latter have been covered by health insurance since the beginning of 2015 and vary (tab. 2). No test so far allows a prediction on the choice of specific chemotherapy.
The competing providers understandably put themselves in the best light and play hardball. Although unconfirmed, the OncotypeDX manufacturer’s website, for example, claims that the test can help even if HER2 status is unclear [30,31]. This explains why the cost of Herceptin® has been included in calculations that, in conclusio, attest to the cost-effectiveness of this test [32]. As experience with other competing products in oncology shows, without pioneering comparisons in Switzerland, the various products will become established in everyday use, leading to a federal puzzle here as well.
As long as reproducibility is not compromised, local testing is advantageous because consultation between clinicians and pathology is possible. This is illustrated by the case of a patient with multifocal breast carcinoma who was enrolled in the SAKK 26/10 study at Inselspital. Proliferation of three- to 1 -cm carcinomas determined by Ki67 was 19%, 27%, and 53%, respectively. The OncotypeDX recurrence score determined in faraway California was reported to be 13%, which could not be questioned regarding representativeness. Furthermore, in the spirit of evidence-based medicine, extrapolations to untested populations, e.g., the use of the EndoPredict in premenopausal women, are not permissible.
Addendum: The first results of the TailorX study [33], published after submission of this manuscript, remain conceptually without influence on the statements made.
Literature:
- Berry DA, et al: High-dose chemotherapy with autologous stem-cell support as adjuvant therapy in breast cancer: overview of 15 randomized trials. J Clin Oncol 2011; 29: 3214-3223.
- Peto R, et al: Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012; 379: 432-444.
- Davies C, et al: Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet 2011; 378: 771-784.
- Sotiriou C, et al: Breast cancer classification and prognosis based on gene expression profiles from a population-based study. Proc Natl Acad Sci USA 2003; 100: 10393-10398.
- Ciriello G, et al: The molecular diversity of Luminal A breast tumors. Breast Cancer Res Treat 2013; 141: 409-420.
- Coates AS, et al: Tailoring therapies-improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol 2015; 26: 1533-1546.
- Goldhirsch A, et al: Strategies for subtypes – dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol 2011; 22: 1736-1747.
- Varga Z, et al: How reliable is Ki-67 immunohistochemistry in grade 2 breast carcinomas? A QA study of the Swiss Working Group of Breast and Gynecopathologists. PLoS One 2012; 7: e37379.
- Parker JS, et al: Supervised risk predictor of breast cancer based on intrinsic subtypes. J Clin Oncol 2009; 27: 1160-1167.
- Paik S, et al: A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med 2004; 351: 2817-2826.
- van de Vijver MJ, et al: A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 2002; 347: 1999-2009.
- van ‘t Veer LJ, et al: Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002; 415: 530-536.
- Dowsett M, et al: Comparison of PAM50 risk of recurrence score with oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine therapy. J Clin Oncol 2013; 31: 2783-2790.
- Fan C, et al: Concordance among gene-expression-based predictors for breast cancer. N Engl J Med 2006; 355: 560-569.
- Varga Z, et al: Comparison of EndoPredict and Oncotype DX test results in hormone receptor positive invasive breast cancer. PLoS One 2013; 8: e58483.
- Buyse M, et al: Integrating biomarkers in clinical trials. Expert Rev Mol Diagn 2011; 11: 171-182.
- Goss PE, et al: A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med 2003; 349: 1793-1802.
- Davies C, et al: Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013; 381: 805-816.
- Bianchini G, et al: Proliferation and estrogen signaling can distinguish patients at risk for early versus late relapse among estrogen receptor positive breast cancers. Breast Cancer Res 2013; 15: R86.
- Pivot X, et al: In the era of genomics, should tumor size be reconsidered as a criterion for neoadjuvant chemotherapy? Oncologist 2015; 20: 344-350.
- Gluck S, et al: Molecular subtyping of early-stage breast cancer identifies a group of patients who do not benefit from neoadjuvant chemotherapy. Breast Cancer Res Treat 2013; 139: 759-767.
- Esserman LJ, et al: Chemotherapy response and recurrence-free survival in neoadjuvant breast cancer depends on biomarker profiles: results from the I-SPY 1 TRIAL (CALGB 150007/150012; ACRIN 6657). Breast Cancer Res Treat 2012; 132: 1049-1062.
- Rakovitch E, et al: A population-based validation study of the DCIS Score predicting recurrence risk in individuals treated by breast-conserving surgery alone. Breast Cancer Res Treat 2015; 152: 389-398.
- Eiermann W, et al: The 21-gene recurrence score assay impacts adjuvant therapy recommendations for ER-positive, node-negative and node-positive early breast cancer resulting in a risk-adapted change in chemotherapy use. Ann Oncol 2013; 24: 618-624.
- Augustovski F, et al: Decision-making impact on adjuvant chemotherapy allocation in early node-negative breast cancer with a 21-gene assay: systematic review and meta-analysis. Breast Cancer Res Treat 2015; 152: 611-625.
- Gnant M, et al: Identifying clinically relevant prognostic subgroups of postmenopausal women with node-positive hormone receptor-positive early-stage breast cancer treated with endocrine therapy: a combined analysis of ABCSG-8 and ATAC using the PAM50 risk of recurrence score and intrinsic subtype. Ann Oncol 2015; 26: 1685-1691.
- Fisher B, et al: Tamoxifen and chemotherapy for lymph node-negative, estrogen receptor-positive breast cancer. J Natl Cancer Inst 1997; 89: 1673-1682.
- Paik S, et al: Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol 2006; 24: 3726-3734.
- Senkus E, et al: Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-updagger. Ann Oncol 2015; 26 Suppl 5: v8-v30.
- Dabbs DJ, et al: High false-negative rate of HER2 quantitative reverse transcription polymerase chain reaction of the Oncotype DX test: an independent quality assurance study. J Clin Oncol 2011; 29: 4279-4285.
- Bhargava R, Dabbs DJ: Oncotype DX test on unequivocally HER2-positive cases: potential for harm. J Clin Oncol 2012; 30: 570-571.
- Holt S, et al: A decision impact, decision conflict and economic assessment of routine Oncotype DX testing of 146 women with node-negative or pNImi, ER-positive breast cancer in the U.K.. Br J Cancer 2013; 108: 2250-2258.
- Sparano JA, et al: Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med 2015 Nov 19; 373(21): 2005-2014.
- Klein ME, et al: Prediction of the Oncotype DX recurrence score: use of pathology-generated equations derived by linear regression analysis. Mod Pathol 2013; 26: 658-664.
- Denkert C, et al: [Molecular pathology for breast cancer: Importance of the gene expression profile]. Pathologist 2015; 36: 145-153.
InFo ONCOLOGY & HEMATOLOGY 2016; 4(1): 10-14.









