
Not all vaccinations that are recommended are really necessary and useful for every patient. A detailed review of vaccinations for travel has recently been published [1]; this article characterizes the travel vaccinations for adults and explains their use in the day-to-day practice of the general practitioner.
Right at the beginning, some pejorative remarks on the importance of travel vaccinations, whose significance is often overestimated in medical travel advice: Only a few vaccinations are really “necessary” for a trip. The preventive value of vaccination in preventing travel-associated diseases is small in absolute terms [2]. The recommendations, like this article, are based on expert opinion rather than evidence-based findings. Experts consider accidents (e.g., in road traffic) and sexually transmitted infections (STIs) to be potentially higher health risks than vaccine-preventable infections [3].
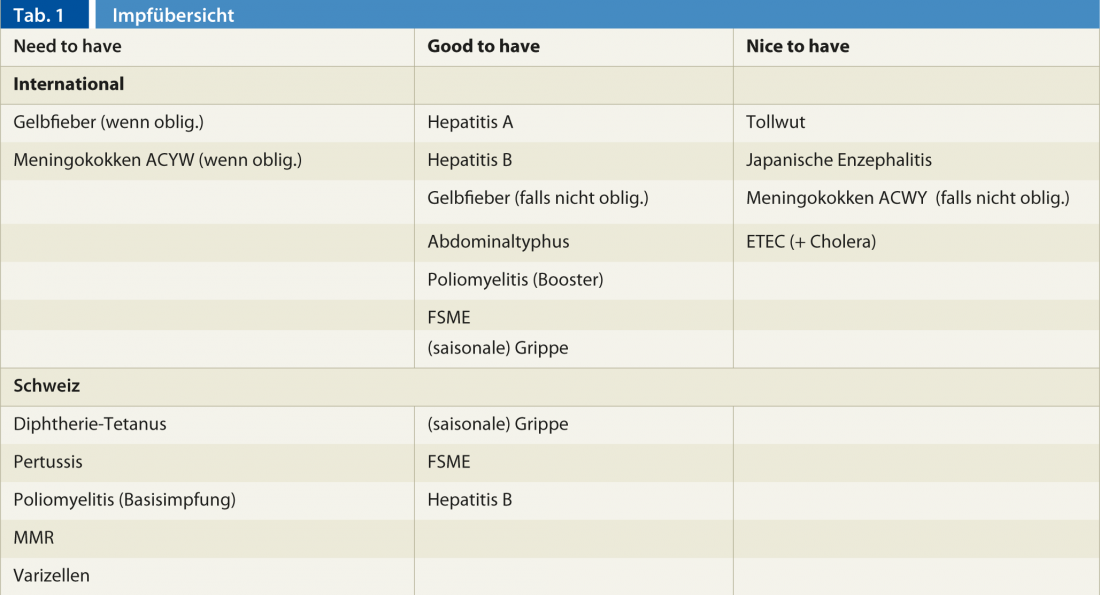
Immunization recommendations may be “individualized.” Not every traveler has the same needs in terms of protection and security. However, it is important that the same information is conveyed to all travelers. Accompanying written materials and fact sheets can help. A medical travel consultation is complex and usually takes 20 minutes or more. The following recommendations are divided into three sections according to necessity: “Need to have,” “Good to have,” and “Nice to have” (Table 1). They affect adults without significant underlying immunomodulatory disease or medication. For patients with severe or chronic illnesses, the consultation of a specialist in tropical and travel medicine is advisable.
Need to have
What must travelers be protected against?
Yellowfiber vaccination: The use of this vaccination is regulated by international treaties and regulations. Therefore, for some regions, this vaccination may be a requirement for entry, even without passage through an actual yellow fever area, e.g., when entering South Africa with a prior visit to Zambia. In other regions, however, vaccination is not mandatory but is strongly recommended for exposure reasons. As an example, the Amazon region of Brazil is considered a region with yellow fever occurrence, but vaccination is not mandatory. As a live vaccine, the yellow fever vaccine can only be given at a distance from other live vaccines. This should be urgently considered in the consultation and vaccination indication by the primary care provider.
Updated distribution maps can be found at www.safetravel.ch. Vaccination indication, vaccination certificate and issuance of the exemption letter are best left to the yellow fever vaccination center.
Meningococcal vaccination: (quadrivalent “ACWY”, validity 3 years) is mandatory for pilgrimage to Mecca (Saudi Arabia). Before the pilgrimage period, specific information from the Saudi Arabian authorities should be consulted because of possible last-minute changes (www.hajin formation.com).
What are travelers protected against – or do at least believe they are?
Here, above all, the basic vaccinations should be checked and, in most cases, supplemented. The chance of closing gaps in basic immunizations is rarely greater than with travelers who are motivated to talk about immunization prophylaxis. Here is an overview of the vaccinations that are especially relevant for adults:
- Diphtheria-tetanus (dT): If the basic vaccination is complete, it should be boostered every ten years (in the 25- to 65-year-old age group every 20 years!); for travel, rather generous indication due to the increased risk of injury. CAVE: Tetanus vaccination alone is obsolete, so combined vaccination should always be given. It should be noted that persons over 60 years of age have not yet been routinely vaccinated as children.
- Pertussis (Pa): Follow the new 2012/2013 recommendations and routinely vaccinate all 25- to 29-year-olds with pertussis combined with dT (IPV). Other vaccination indications: regular contact with infants under six months of age.
- Poliomyelitis: A complete basic vaccination should be available (see also remarks below).
- Measles-mumps-rubella (MMR): Revaccinate if basic vaccinations are not proven. Two vaccinations in total necessary, interval at least four weeks. Medical history unproductive (exception: birth before 1964 is considered protected), antibody measurement not recommended as routine (insufficient sensitivity of tests, cost). CAVE: Live vaccine (no pregnancy, no other live vaccines such as yellow fever applicable within 3-4 weeks).
- Varicella: Only forego vaccination if history is reliable, otherwise vaccinate (2 vaccinations required, at least 6-8 weeks apart). CAVE: Live vaccine (no pregnancy, no other live vaccines applicable within 3-4 weeks).
- TBE vaccination (basic vaccination in endemic areas of Switzerland): To be discussed in particular and also recommended if travel to Eastern Europe or northern Central Asia is planned.
Ask about possible future travel as early as routine immunizations (polio, for example, can be given in combination with plans to travel to Africa in the next 10 years).
Good to have
What vaccination should the traveler have before departure?
- Hepatitis vaccinations(Hepatitis A/Hepatitis B) are among the generally recommended travel-associated vaccinations. Combination vaccines are preferable despite differences in transmission and prognosis. Here, it is important on the one hand to give travelers the right protection (last-minute vaccinations) and on the other hand to correctly assess booster vaccinations. Principle: Hepatitis A: (single vaccine) one vaccination is sufficient until shortly before departure; hepatitis B and combined hepatitis A/B vaccines require at least two vaccinations for acceptable protection.
- Poliomyelitis (vaccine only available inactivated as IPV): If basic vaccination is available, vaccinate only if travel to areas with possible risk of transmission is planned (generally: entire continent of Africa as well as regions in south-central and central Asia with Pakistan, Afghanistan, western China and surrounding states). If possible, vaccinate together with diphtheria-tetanus (see above).
- Abdominal typhoid: Primary protection, consistent with protection against traveler’s diarrhea, is careful choice of food and drink. Vaccination is considered secondarily for travelers with a high probability of exposure who will be living in poor sanitary conditions or whose destination is South Central Asia (India/Nepal region). Allow enough time for this oral vaccination (start at least 3 weeks before).
- Influenza: The flu, which is seasonal in our country, is transmitted somewhere in the world at any time, and in tropical areas often throughout the year. The same indications for a ream apply as in our country before the flu season.
- Unfortunately, there are no vaccinesagainst: Arthropod bites (mosquitoes, ticks), nor against diseases transmissible through these bites such as malaria, dengue, chikungunya, West Nile fever or most sexually transmitted infections (STIs).
Nice to have
What vaccination is offered to the traveler before departure? Against what does the traveler (usually) not need vaccination, but must know disease prevention?
- Rabies ( “vaccine-preventable, but not treatable”): Knowledge of the disease and the measures to be taken after contact with a mammal are much more important than vaccination! Pre-trip discussion should include items such as “no petting cats,” “no jogging at night on the beach,” i.e., avoiding exposure. In addition, false assumptions such as “rabies-carrying animals foam at the mouth” or “after returning, the disease can still be treated” need to be corrected. All travelers must be clearly shown and given written post-exposure measures (PEP), including rabies vaccination recommendations. Indications for pre-exposure vaccination (at least three times, shortest interval 0-7-21 days) include: Children under eight years of age or destinations with increased risk such as South Central Asia (India/Nepal region), longer stay than four weeks duration, planned contact with (unvaccinated) mammals, bicycle tours or vaccine shortage at the destination. These previously vaccinated travelers must also be informed about the post-exposure measures that must nevertheless be taken (keyword: 100% fatal disease requires 100% protection).
Against what do travelers (mostly) not need vaccination?
- Japanese encephalitis: Here, knowledge of the possibility of transmission and mosquito protection in the affected regions of Asia is important. For the infrequent indication for vaccination, the vaccination intervals (2 doses 4 weeks apart, starting no later than 5 weeks before departure), the possibility of booster vaccination after 15 months, and the importance of protecting children in the off-label use of vaccination must be clearly communicated.
- Meningococcal meningitis: Vaccination is indicated only during the high-risk season when traveling to endemic areas of Africa and when traveling during the Hajj. The correct vaccine, quadrivalent conjugate vaccine, must be used. For routine meningococcal vaccinations of persons in Switzerland who have planned a trip to an endemic area during the protection period of the vaccination, the quadrivalent vaccination “ACWY” and not only a “C” should already be given.
- Vaccination against heat-labile enterotoxin-producing Escherichia coli (LT ETEC): This vaccination may be of some help to patients who frequently experience traveler’s diarrhea, especially during the first week of their stay. The vaccine is combined with the cholera vaccine, but this is (almost) never indicated in travelers.
And by the way…
Use follow-up vaccination appointments before departure to refresh important knowledge (malaria prophylaxis, rabies prophylaxis) and answer remaining questions (first-aid kit). This can also be done by trained MPAs.
Always carry out vaccination entries immediately and correctly (in the right place) according to the principle: one vaccination, one entry, one glue. Never write dates into the vaccination record in advance and use separate slips of paper or leaflets to remind people of revaccinations.
“Every vaccination counts”: Don’t start over if vaccinations are interrupted, just keep going, even after years or decades.
Literature:
- Neumayr A, et al: Vaccinations during foreign travel 2010, Switzerland Med Forum 2010; 10(43): 753-756.
- Boggild AK, et al: Vaccine preventable diseases in returned international travelers: Results from the GeoSentinel Surveillance Network. Vaccine 28(2010): 7389-7395.
- Zimmermann R, et al: Risk Perception of Travelers to Tropical and Subtropical Countries Visiting a Swiss Travel Health Center. J Travel Med 2013; 20(1): 3-10.









