Menisci are components of joints and consist of cartilage tissue. An important function of the knee meniscus is secondary stabilization of the knee joint. The disc meniscus is an anatomical norm deviation, whereby different subtypes are distinguished on the basis of morphological criteria.
The normal meniscus, crescent-shaped in plan view, functions as a pressure absorber between the femur and tibia in the leg axis and is composed mainly of type 1 collagenous material [1]. It compensates for the space between the differently shaped articular surfaces of the femoral condyle and tibial head and thus also secondarily stabilizes the knee joint. The medial meniscus is more C-shaped than the lateral meniscus and is in contact with the joint capsule. The lateral meniscus is more freely mobile [14].
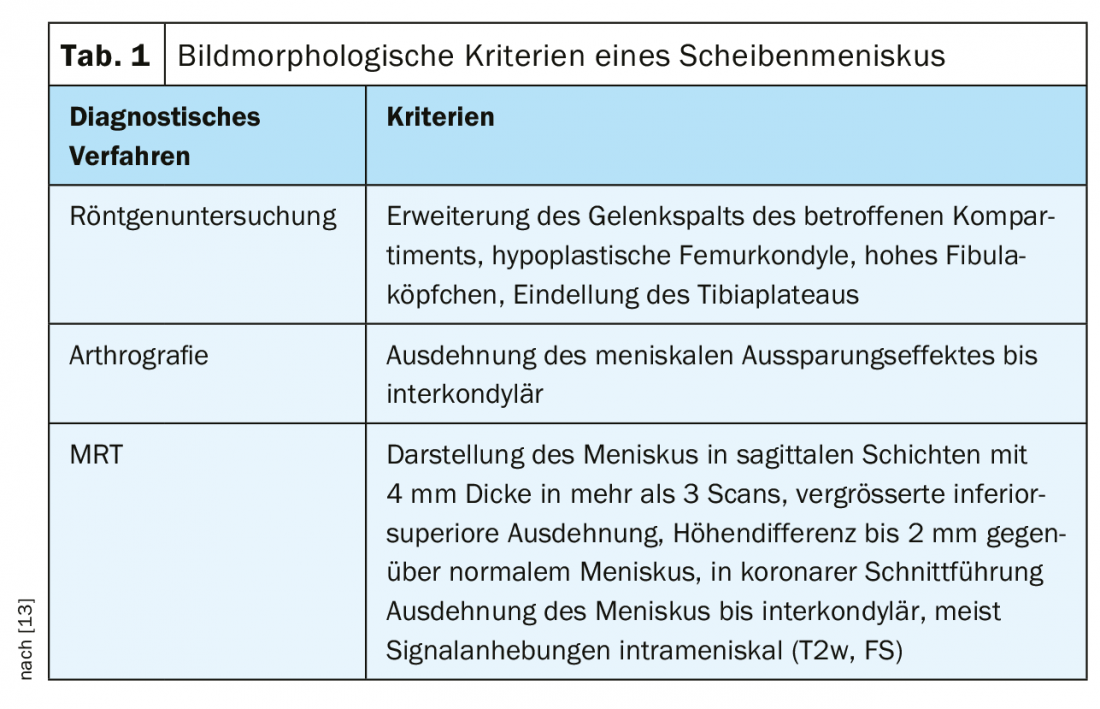
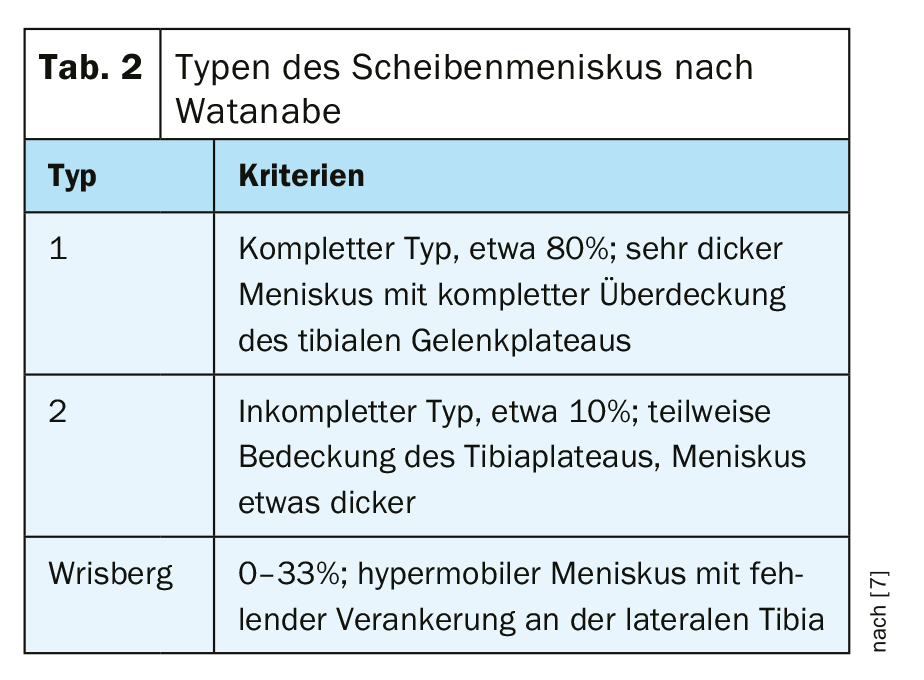
A disc meniscus is an enlarged, disc-like meniscus [2,10,11]. Table 1 summarizes image morphologic criteria that may indicate a disc meniscus [13]. It is ten times more common in the lateral knee joint compartment than medially, but can also occur laterally and medially, and unilaterally or bilaterally. The incidence is reported to be 3 to 5% of the population. Publications on bilateral, medial, and lateral disc menisci are available [6], but these constellations are very rare. Primarily asymptomatic, however, there is a greater predisposition to degeneration, rupture and formation of ganglia. Also typical is the acoustically perceptible popping during stronger movement, the “popping knee syndrome”. According to Watanabe [7], three types of disc meniscus are distinguished (Table 2).
Disc menisci are more common in Asians than in the Western world [8], including the bilateral anomaly. In connection with the formation of the meniscal anomaly, accompanying bony variants of the knee joint have also been described, affecting the formation of the shapes of the joint contours or the position in relation to each other [3]. Disc menisci may occur along with achondroplasia, the most common skeletal dysplasia [5]. This is caused by a mutation in the fibroblast growth factor receptor 3 (FGFR3) gene. Diagnosis was usually made in childhood in symptomatic disc meniscus, which can cause blockage, pain, and joint swelling [9]. However, a disc meniscus often remains clinically silent for a long time.
The therapeutic consequence depends on the type of anomaly, the age of the patient, the symptomatology or joint stability, and the presence of a meniscal rupture. Symptomatology is more likely to occur with bilateral anomaly, and surgically treated children with bilateral disc meniscus are on average younger than those with unilateral findings [4,12]. Improved arthroscopic techniques have also led to improved surgical outcomes and postoperative course. Increasing attention is paid to the integrity of the meniscal contour through partial meniscectomy and, after reduction of the volume, to reparative measures of tears.
Computed tomographic ex aminations, as native joint examinations, are of little value in the diagnosis of the disc meniscus; only in combination with an intra-articular application of contrast medium analogous to the earlier X-ray arthrography can a corresponding statement then be made with the multiplanar reconstruction.
Magnetic resonance imaging suggests a disc meniscus when the hypointense meniscal structure becomes detectable in sagittal scans in more than 3 to 5 mm thick layers, and the anterior and posterior horns of the meniscus present on only one or two sagittal layers near the intercondylic fossa [2]. The centrally tapering configuration is absent and the height of the disc meniscus is usually 1 to 2 mm above the normal contralateral meniscus.
Case studies
Case report 1 demonstrates a lateral disc meniscus (Fig. 1 A-D, arrows) in a 38-year-old man who reported load-dependent, recurrent knee pain bilaterally for several years. Bilateral lateral disc meniscus was present.

Take-Home Messages
- The disc meniscus is a normal variant and occurs more frequently in Asians.
- The lateral disc meniscus is ten times more common than the medial, but it can also occur medially and laterally as well as bilaterally.
- The asymptomatic forms have no consequence; if clinical symptoms are present, arthroscopic treatment is indicated.
- Concomitant bony abnormalities may occur in the knee joint, including achondroplasia.
Literature:
- Birchard Z, Tuck JA: Discoid meniscus [Updated 2019 Dec 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan. Available from: www.ncbi.nlm.nih.gov/books/NBK470370/
- Burgener FA, Meyers SP, Tan RK, Zaunbauer W: Differential diagnosis in MRI. Stuttgart, New York: Georg Thieme Verlag 2002; 393.
- Chen XX, Li J, Wang T, Zhao Y, Kang H: Anatomical knee variants in discoid lateral meniscal tears. Chin Med J (Engl) 2017; 130(5): 536-541.
- Hagino T, et al: Arthroscopic treatment of symptomatic discoid meniscus in children. Arch Orthop Trauma Surg 2017; 137(1): 89-94.
- Hoernschemeyer DG, Atanda A Jr, Dean-Davis E, Gupta SK: Orthopedics 2016; 39(3): e498-503.
- Kann H, et al: Medial and Lateral Discoid Menisci of Both Knees. Knee Surg Relat Re 2016; 28(4): 330-333.
- Kelly BT, Green DW: Discoid lateral meniscus in children. Curr Opin Pediatr 2002; 14(1): 54-61.
- Kim JG, Han SW, Lee DH: Diagnosis and Treatment of Discoid Meniscus. Knee Surg Relat Res 2016; 28(4): 255-262.
- Kushare I, Klingele K, Samora W: Discoid Meniscus: Diagnosis and Management. Orthop Clin North Am 2015; 46(4): 533-540.
- Liu WX, et al: Prevalence of Bilateral Involvement in Patients with Discoid Lateral Meniscus: a Systemic Literature Review. Acta Orthop Belg 2016; 83(1): 153-160.
- Mahapatra S, Ambasta S: Bilateral Discoid Medial Menisci: A Case Report. JBJS Case Connect 2016; 6(3):e53.
- Patel NM, Cody SR, Ganley TJ: Symptomatic bilateral discoid menisci in children: a comparison with unilaterally symptomatic patients. J Pediatr Orthop 2012; 32(1): 5-8.
- Stoller DW: Magnetic Resonance Imaging in Orthopaedics and Sports Medicine. Volume One: Lower Extremity. Third Edition. Baltimore: Lippincott Williams&Wilkins 2007; 440-444.
- Thiel HJ: Anomalies and norm variants: disc meniscus. Deutscher Ärzteverlag, MTA Dialog 2018; 19(12): 36-39.
HAUSARZT PRAXIS 2020; 15(1): 34-35