In St. Gallen, interested parties were able to attend a series of lectures for the seventh time, which focused on an annual review of developments in the field of neurology. HIFUS ultrasound highly focused to set lesions in a controlled manner and ultrasound examination of peripheral nerves will be introduced in the future. Patches for pain and new oral therapies for multiple sclerosis are expanding treatment options.
Update events are popular, as they offer a valuable compilation, in this case by subject matter experts from the Cantonal Hospital of St. Gallen. Prof. Barbara Tettenborn, MD, and Thomas Hundsberger, MD, called for a “hussar ride” through neurology, with the senior physicians of neurology at the Cantonal Hospital of St. Gallen holding the reins with their respective specialties. Progress in the individual areas may not be as rapid as hoped, but there are nevertheless developments in diagnostics and therapy that will soon gain clinical significance, the chief physician introduced the event.
News on Parkinson’s syndrome
REM sleep disturbances are likely the first indication of α-synucleinopathy, which may develop into Parkinson’s disease in subsequent years and decades. Stefan Hägele-Link, MD, discussed the role of α-synuclein as a potential biomarker to diagnose Parkinson’s disease very early. According to a widely accepted hypothesis, the disease begins in the intestine and then ascends to the brainstem via the autonomic nerve pathways of the vagus nerve. Like a prion disease, α-synuclein could spread through the brain by direct contact between the pathological with the healthy variant of the protein.
An important message: A movement disorder needs movement – in other words, the facts about the benefits of physiotherapy in the treatment of Parkinson’s patients are corroborating. There is also a positive work on Tai-Chi. There are data that smokers are less likely to get Parkinson’s. Will nicotine be used as a protective substance in the future? Probably not.
Only rasagiline showed a possible protective effect on the course of Parkinson’s disease in one paper. Pramipexole did not meet the study objective last year.
St. Gallen now offers the DaTSCAN™ technique (Ioflupan [123I]), which can be used to distinguish essential from parkinsonian tremor in differential diagnostic issues. The loss of neurons in the striatum that release dopamine points to Parkinson’s as the cause. St. Gallen cooperates with the USZ in the technique of neurostimulation and now treats a Parkinson’s patient almost every week with this technique.
Pelvic nerve compression syndromes
The most dangerous fashion in the world presented Stephan Nitschke, MD: Skinny jeans are “garments with their own disease,” according to Cosmopolitan. Meralgia paraesthetica can develop with too much tightness in too skimpy pants. If the lateral cutaneal femoral nerve is overstretched or compressed in its course under the inguinal ligament, hypoesthesias and dysesthesias may occur anterolaterally on the thigh. Tinel’s sign, a pain on palpation, becomes positive. Detection is by neurography, SEP, or, newly, nerve ultrasonography. As therapy, occasionally the disposal of the causative garment is sufficient. However, local anesthesia with steroids or rarely surgical exposure and neurolysis may be needed.
Pelvic nerve compression syndromes are usually treatable conservatively (anti-inflammatories, injections of local anesthetics and glucocorticoids possibly EMG/ultrasound/CT guided). Anticonvulsants acting on neuronal calcium channels (pregabalin, gabapentin) and antidepressants (e.g., amitryptiline, duloxetine) are helpful. Only after conservative options have failed should surgical neurolysis or the ultima ratio – destructive procedures such as cryoablation, neurectomy – be considered.
Capsaicin in pain therapy
Jessica Müller-Westermann, MD, gave a very practical overview of the use of the capsaicin patch Qutenza® (Tab. 1) for the therapy of peripheral neuropathic pain in adult patients (except in diabetic neuropathy – according to Dr. Müller-Westermann’s report, only the studies are missing for this, the efficacy would be given) [1]. Using the patient case of a 52-year-old breast carcinoma patient with Taxol-induced therapy-resistant pain on the dorsum of the foot, she described the procedure in the pain outpatient clinic. One plaster each under occlusion (household foil) brought the hoped-for relief of pain for the patient.
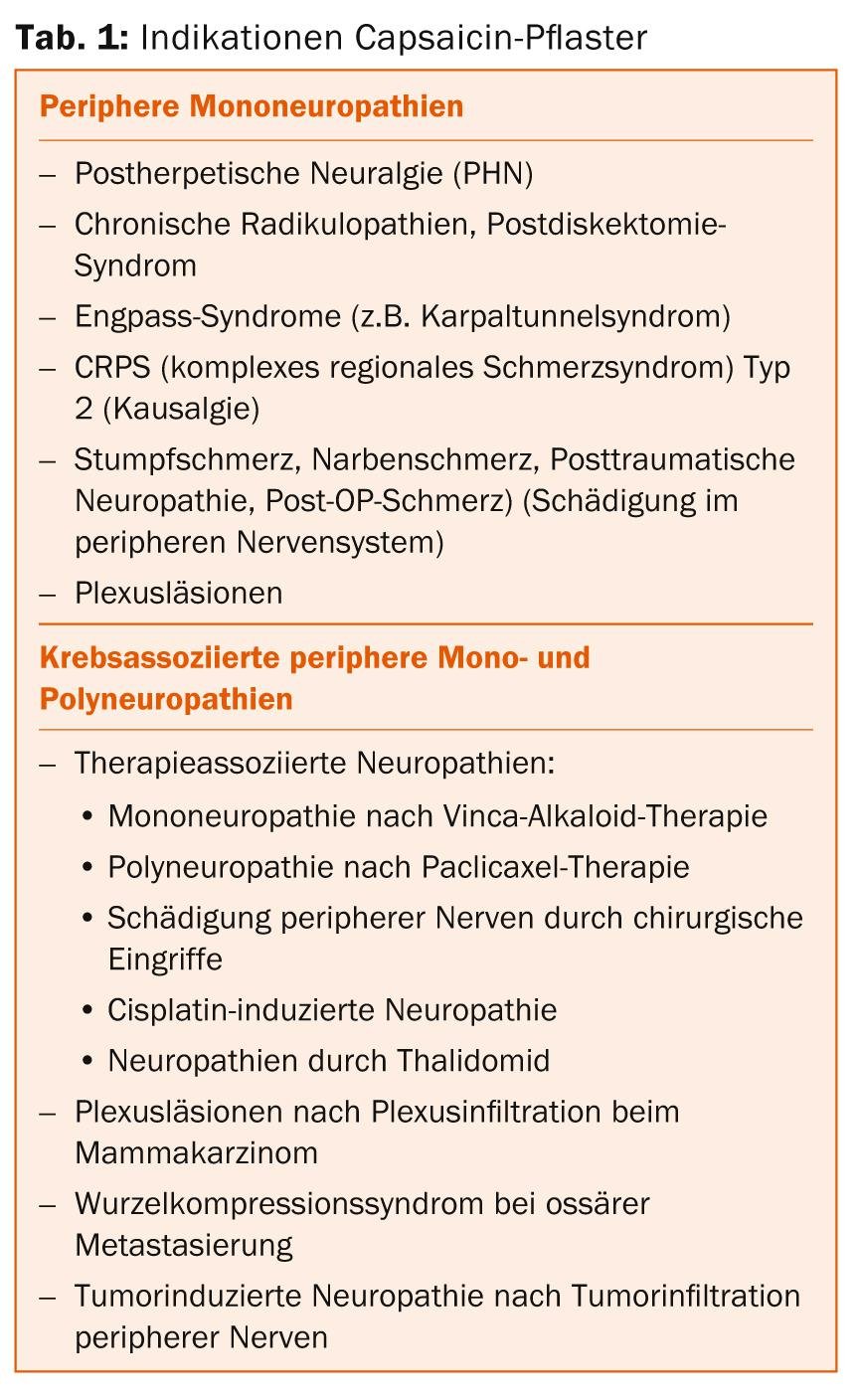
Capsaicin acts selectively at the site of pain by reversible defunctionalization of cutaneous nociceptors. It is a highly selective agonist for the TRPV1 receptor (“Transient Potential Receptor Vanilloid 1”), which belongs to the family of thermoreceptors. These are located on the surface of nociceptive neurons in the peripheral and also central nervous system. Binding to TRPV1 leads to an increase in intracellular calcium levels and the release of vasoactive neuropeptides, including substance P. Local vasodilation leads to the perception of painful heating with hyperemia and local redness. Therefore, patients must be appropriately prepared analgesically. Depletion of substance P makes nociceptors less sensitive to various stimuli and leads to defunctionalization via depletion of epidermal nerve fibers, especially C-fibers. Analgesic efficacy has been demonstrated in several neuropathic pain models (PHN/HIV-AN), she said.
Limbic encephalitis
Dr. med. Monika Kapauer referred to a clinical picture that unfortunately leads again and again at least initially to admission to psychiatry. In limbic encephalitis, a psychotic state with hallucinations, delusions, and anxiety and an alternating state between agitation and somnolence are suggestive of a psychiatric disorder [2]. Only when extrapyramidal movement disorders in the sense of orofacial dyskinesia, autonomic dysregulation and hyperventilation occur, the inflammatory genesis of the clinical picture becomes clear. If somnolence, fever, and stupor increase, transfer to an IPS is often required.
The list of differential diagnoses is long: herpes encephalitis, varicella-zoster encephalitis, cytomegalovirus, Creutzfeld-Jakob disease, metabolic/toxic encephalopathy, primary cerebral vasculitides, etc. It is recommended to differentiate a paraneoplastic from an autoimmune form in limbic encephalitis for therapeutic and prognostic considerations. In around 60% of cases, the underlying cause is a tumor. If antibodies against intracellular antigens (HU, Ma2, CV2) are found, this almost always indicates a tumor. Early immunotherapy is associated with a better prognosis, and tumor therapy has the greatest impact on clinical remission. Cell-based tests in serum and CSF are recommended for diagnostic purposes due to their higher sensitivity. The rapid discovery of additional specific pathogenic antibodies will continue.

Multiple sclerosis pills
Med. pract. Stefanie Müller gave a brief summary of the study results from TEMSO and TOWER on teriflunomide (Aubagio®) in MS. The optimal dosage is 14 mg once a day. Most common side effects involved the gastrointestinal tract with diarrhea, nausea, and slightly elevated levels of alanine aminotransferase ALT. The hair density decreases, but there is no hair loss. The potential for interaction involves antibiotics (OAT3 inhibitor), statin and glitazone, and warfarin. Before starting therapy, it is particularly important to exclude contraindications: liver disease, immunodeficiency, anemia, bone marrow dysfunction, screening for latent tuberculosis. Reliable contraception in women of childbearing age is required. At the beginning of a therapy, regular blood pressure, liver value and blood count checks are necessary.
Normal pressure hydrocephalus
Approximately 5-6% of all dementias are due to normal pressure hydrocephalus. Dominik Zieglgänsberger, MD, presented this clinical picture, for which surgery was often performed in the past with little success and a high complication rate. Today, more precise diagnostics make early surgery possible with often astonishing results.
The first symptom and leading symptom is often dizziness. The so-called Hakim triad of dementia, gait disorder (wide, small-stepped gait sticking to the floor with disturbance in turning, feet rotated outward), and urinary incontinence points to the diagnosis. The partial areas deteriorate at different rates individually, and the complete triad does not develop until the advanced stages. Psychomotor slowing, attention and concentration deficits, and short-term memory impairment are typical. In the advanced stage apathy up to mutism can be found. Differential diagnoses include Alzheimer’s disease, other neurodegenerative diseases, or vascular dementia.
First therapy attempt can be CSF drainage (at least 30, better 40-70 ml). With today’s shunt surgery methods and thanks to new valves, improvement can be achieved in about 81% of those affected. Especially in case of prominent gait disorder, a positive result is to be expected. If dementia is the primary cause, the prognosis is much less favorable.
CSF diagnostics for dementia clarification
“There are currently about 120,000 dementia patients living in Switzerland,” said Ansgar Felbecker, MD. Since there is as yet no treatment for the disease, an early diagnosis is often more stressful than reassuring for an affected person and their relatives. The right not to know must be balanced against the desire to clarify symptoms. The pathological processes start 10-20 years before clinically manifest dementia. Biomarkers that appear at different points in the course of dementia could on the one hand enable early diagnosis, and on the other hand also help in the differential diagnosis of dementias that are not always clearly distinguishable clinically and neuropsychologically.
Tau protein, phospho-tau protein, β-amyloid, and combined analyses are available for specific CSF diagnosis in dementia. Dementia markers can only ever be a diagnostic criterion in the overall assessment of history, clinic, neuropsychology, and cMRI, as their specificity is moderate, Dr. Felbecker emphasized.
Source: Update Neurology, February 6, 2014, St. Gallen, Switzerland.
Literature:
- Professional information QUTENZA®; www.swissmedic.ch
- Prüss H: Neuroimmunology: news on limbic encephalitis. Act Neurol 2013; 40: 127-136.
InFo NEUROLOGY & PSYCHIATRY 2014; 12(3): 43-45.