
For skin diseases, herbal preparations can often be used, which sometimes work as well as steroids. In the following, two types of dermatoses are presented for which the use of a herbal preparation can bring help: Contact dermatitis and atopic dermatitis.
Corticosteroids are often used for dermatological problems, and although they are very often effective, they are not popular with large sections of the population. As an alternative, herbal medicines can be used for various dermatological problems – but the choice has to be made carefully. Unfortunately, there are a lot of unqualified promotions of herbal preparations, which have nothing to do with serious phytotherapy.
In the following, some skin diseases are presented for which the efficacy of herbal applications is partly proven with clinical studies.
Tea tree oil against contact dermatitis
The effectiveness of a preparation with tea tree oil from the Australian tea tree (Melaleuca alternifolia) was proven with a study published in 2011 [1]. The following subjects were recruited for this purpose:
- Patients diagnosed with nickel allergy, in whom contact dermatitis was provoked with nickel.
- Volunteers in whom contact dermatitis was induced with benzalkonium chloride.
- Volunteers in whom an immediate reaction was induced with histamine or benzoic acid.
- The allergizing substances were applied to the subjects in a standardized manner on the upper arm or forearm, and the degree of allergy was determined after 48 hours. The affected skin sites were then randomized and treated according to the standard of care with (alternative):
- 50 mg clobetasone butyrate ointment
- Ichthyol 10%
- Zinc paste 20%
- Camphor 20%
- Levomenthol 20%
- Tea tree oil 20% or 50%.
Because a 50% solution of tea tree oil caused redness in some subjects, only a 20% solution was used in the remaining subjects.
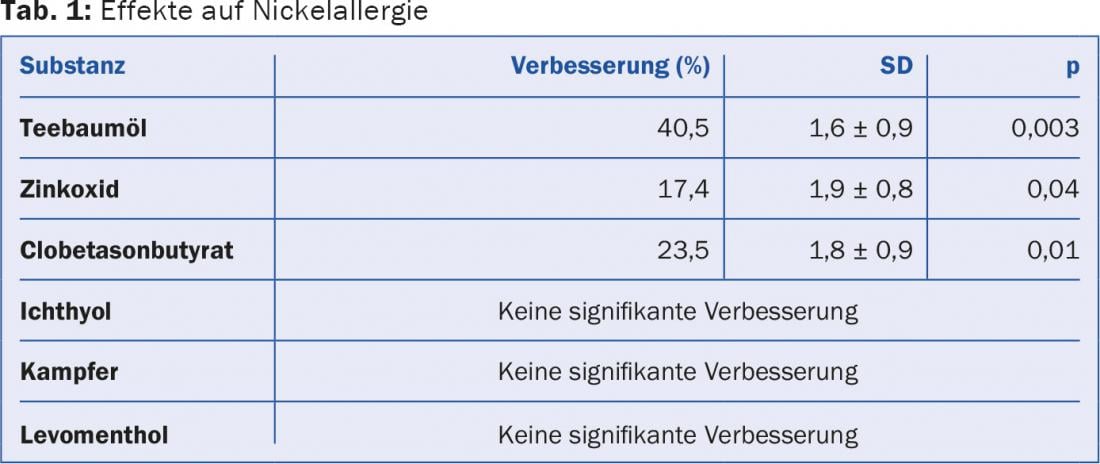
The applied substances produced the average improvements in nickel allergy shown in Table 1.
Allergies induced by histamine or benzoic acid were not improved by any of the applied substances. Clobetasone butyrate produced a non-significant improvement in benzalkonium chloride exposure (p=0.07).
This study demonstrated that tea tree oil, clobetasone butyrate, and zinc oxide provided significant improvement in the treatment of triggered nickel allergy. Tea tree oil proved to be more effective than clobetasone butyrate and zinc oxide and is therefore particularly suitable for the treatment of a corresponding allergy.
Atopic dermatitis
Various medicinal plants are available for the treatment of episodes of atopic dermatitis or neurodermatitis, the efficacy of which has been documented with clinical studies.
Balloon vine (Cardiospermum halicacabum): Merklinger and coworkers published a study in 1995 [2] that confirmed the narrow superiority of an ointment containing an extract of Cardiospermum over placebo in atopic dermatitis.
St. John’s wort (Hypericum perforatum): St. John’s wort, best known for its effect against mild to moderate depression, also has potential for treating neurodermatitis. However, it is not ingested, but applied as a cream. A double-blind study investigated a hypericum preparation with a high content of hyperforin in patients with subacute atopic dermatitis in a half-side comparison [3]. In this randomized and placebo-controlled trial, the verum drug was superior to placebo. Further, it was very well tolerated by the patients.
Mahonia (Mahonia aquifolia): The use of Mahonia preparations in atopic dermatitis has a long folk medical tradition. Donsky et al. published a prospective non-comparative study [4]. During twelve weeks, 42 patients with diagnosed neurodermatitis were treated with an ointment whose active ingredient was Mahonia aquifolium. The Eczema Area and Severity Index (EASI) served as the outcome variable, showing significant improvement over baseline. In a post-treatment survey, the subjects attested to a clearly positive result for the study preparation in terms of efficacy and itching. However, because of the lack of control, some doubt remains.
Evening primrose (Oenothera biennis, Fig 1): Preparations with evening primrose seed oil have often been investigated since the 1980s and yielded varying results. A meta-analysis by Morse and Clough [5] reached a positive result. Twenty-six clinical studies were included, all of which were conducted with the same evening primrose oil preparation (the preparation is commercially available in Switzerland as Epogam® 1000 Vergicaps and is distributed by the company Max Zeller Söhne & Co). The total number of included patients diagnosed with atopic dermatitis was 1207.

In the subgroup of patients treated with potent corticosteroids for pruritus, no additional benefit was identified with the additional administration of the study drug. In contrast, an advantage was seen in the subgroup treated with a low-potency corticosteroid only. Here, an improvement of 4-6 cm recorded on the Visual Analogue Scale (100 mm) was found.
Other authors came to a negative conclusion and denied the efficacy of evening primrose seed oil in atopic dermatitis. In terms of responders and non-responders, fatty acid metabolism and the immune system seem to play an important role in affected patients.
In a study published in 2014, Simon et al. [6] 21 patients with atopic dermatitis during twelve weeks daily 4-6 g of evening primrose seed oil rich in gamma linolenic acid (GLA). The plasma content of this substance is very low in patients with atopic dermatitis due to a deficit of delta-6-desaturase and seems to be one of the triggering factors for the skin disease. After four and twelve weeks of treatment, a significant increase in GLA as well as its metabolite dihomo-gamma-linolenic acid (DGLA) was measured in the pre-protocol population (n=12). Further, a significant correlation was documented between the increase in GLA or DGLA and improvement in the SCORing Atopic Dermatitis (SCORAD) Index, a scale for clinical improvement in atopic dermatitis. The authors concluded from these results that in evening primrose oil therapy, the plasma increase in GLA is a predictive parameter of response to therapy.
Summary
For skin problems, corticosteroids are used very often and without discussion, which lead to success in many cases, but are unpopular among broad sections of the population. Herbal medicines are an alternative, e.g. in the cases presented here with contact dermatitis or atopic dermatitis.
Literature:
- Wallengreen J: Tea tree oil attenuates experimental contact dermatitis. Arch Dermatol Res 2011; 303(5): 333-338.
- Merklinger S, Messemer RC, Niederle S: Eczema treatment with Cardiospermum halicacabum. Journal of Phytotherapy 1995; 16: 263-266.
- Schempp CM, Hezel S, Simon JC: Treatment of subacute atopic dermatitis with St. John’s wort cream. Dermatologist 2003; 54: 248-253.
- Donsky H, Clarke D: Relieva, a Mahonia aquifolium extract for the treatment of adult patients with atopic dermatitis. Am J Ther 2007; 14: 442-446.
- Morse NL, Clough PM: A meta-analysis of randomized, placebo-controlled clinical trials of Efamol evening primrose oil in atopic eczema. Where do we go from here in light of more recent discoveries? Curr Pharm Biotechnol 2006; 7: 503-524.
- Simon D, et al: Gamma-linolenic acid levels correlate with clinical efficacy of evening primrose oil in patients with atopic dermatitis. Adv Ther 2014; 31(2): 180-188.
HAUSARZT PRAXIS 2015; 10(10): 4-5









