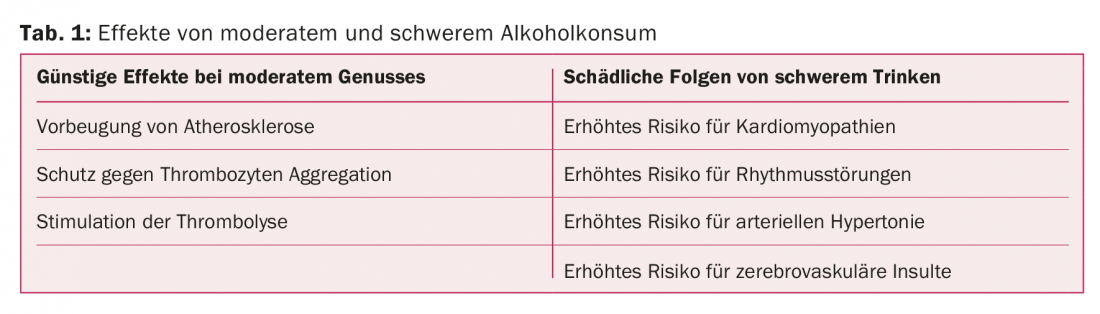
With moderate consumption, equivalent to two to three alcoholic drinks per day, a protective effect against coronary heart disease can be observed. As for the different types of alcohol (beer, wine, liquor), no difference in protective effect has been found so far. But wine drinkers have a healthier lifestyle. Moderate alcohol consumption cannot simply be defined by quantity: Seven drinks on the weekend have a different effect than one drink a day per week. The adverse cardiac consequences of alcohol abuse include cardiomyopathies, arrhythmias, hypertension, and cerebrovascular insults.
The question of whether and how healthy or harmful alcohol is for the heart has long been debated. Often this topic is connected with emotions, be it from the side of the abstainers, but also from the side of the so-called bon vivants. Numerous publications and reputable studies have evaluated the risk and benefits of alcohol consumption. If it is clear that alcohol in excess can be unhealthy to fatal, moderate consumption of alcohol (20 g/day, about ¼ l of wine or 0.5 l of beer) does not seem dangerous and may be healthy.
Historical background
Hippocrates introduced wine around 400 BC. “officially” into the art of healing. He used it as a tonic for convalescents, as a sedative and sleep aid, for headaches and mood disorders, as a painkiller, for heart and circulatory disorders, and even for eye diseases. He also prescribed wine for bloating, for bacterial and toxic intestinal diseases, and as a diuretic. Externally, it was used for wound treatment. In the Old Testament, wine is mentioned in connection with the heart: Psalm 104:15 “…that wine may gladden the heart of man…” Also, in the New Testament, Paul recommends wine to his friend Timothy: I Timothy 5:23 “No longer drink only water, but add a little wine to it for the sake of your stomach, and because you are often sick.” The abbess of Rupertsberg and mystic Hildegard of Bingen (1098-1179) in her work “Causae et Curae” recommended the heart wine (parsley stalks, a little vinegar, white wine and bee honey) for the treatment of circulatory disorders. In 1892, the local health insurance fund in Heidelberg, in consultation with the panel doctors, declared a bottle of wine to be a prescribable therapeutic agent. As early as 1931, Dr. Timothy Leary described the “therapeutic benefits” of alcohol by reducing the risk of diabetes and atherosclerosis in an article in the New England Journal of Medicine. And still in 1979, the Pharmacopea Helvetica mentions wine as a therapeutic agent: Vinum Condurango and Vinum Meridianum Dulce.
Biological effect of alcohol
In ethanol, two functions act together, although sometimes in competition with each other: the lipophilic ethyl group and the hydrophilic hydroxyl group. This amphiphilic dual character enables rapid diffusion of ethanol into the blood. The lipophilic property allows it to easily penetrate cell membranes composed of lipids. Therefore, when ethanol is consumed, a portion is already absorbed in the oral cavity. Blood ethanol levels are almost exactly the same as brain ethanol levels.
Potential beneficial biochemical cardiovascular effects.
Of the multiple cellular and molecular mechanisms that might explain the beneficial effects of alcohol intake, the following four are probably the most important: 1. high density lipoprotein, 2. Biochemical signals, 3. platelet function in thrombosis and 4. stimulation of thrombolysis.
- The stimulatory effects of alcohol on HDL levels are based on epidemiological studies: an increase of approximately 0.1-0.2 mm/l HDL is observed with moderate consumption. However, the biochemical mechanisms remain unclear.
- Endothelial cells send biochemical signals (cellular signaling) that stimulate inflammatory processes in the development of fatty streaks, with trapping of LDL and phagocytes in the subendothelial space. Subsequently, LDL particles oxidize and transcription factors (e.g., NF-κB in endothelial cells) are activated, which contribute to the development of atherosclerosis. It is postulated that alcohol inhibits this NF-κB function. The antioxidant effects of wine could also inhibit the oxidation of LDL.
- Alcohol could alter the structural integrity of platelets, thereby inhibiting their aggregation. Chronic alcohol consumption significantly reduces platelet function, increasing bleeding time.
- Plasma fibrinolytic activity is stimulated by moderate but not heavy alcohol consumption. Epidemiological studies have shown a positive association between alcohol consumption and fibrinolytic activity, which stimulates the conversion of plasminogen to plasmin. Plasmin promotes lysis of thrombus, which may explain the protective effect of alcohol against acute coronary events. However, it should be emphasized that this could also explain the increased risk of bleeding. Mention is also made of another mechanism that has not been proven with certainty: Alcohol is supposed to improve the effectiveness of insulin and thus slow down the development of insulin resistance and, accordingly, diabetes mellitus.
Wine drinkers with healthier lifestyles
Of the numerous studies that have evaluated the association of alcohol and coronary heart disease, Mukamal et al. at best, a favorable effect: among 38 007 men working in health care, the risk of coronary heart disease was lowest among those who consumed three or more alcoholic beverages per week and less than 25 g of alcohol or three alcoholic beverages per day, preferably at mealtimes. With one or two glasses of wine (20 g/day), a protective effect against coronary heart disease was observed.
No positive effect could be demonstrated in people who had never drunk alcohol before. Therefore, wine consumption cannot be recommended in general. However, it must be emphasized that certain non-abstainers probably have the healthiest lifestyles: Those who drink wine regularly also tend to have a healthier lifestyle. When comparing lifestyle habits, it was found that moderate wine drinkers, in contrast to beer or liquor drinkers, but also to teetotalers, smoke less, eat less fatty food and exercise more.
Cardiovascular consequences of heavy alcohol consumption.
There are four specific cardiovascular diseases known to be caused by alcohol.
Ethylic cardiomyopathy: The association of excessive alcohol consumption and enlargement of the heart with insufficiency was described more than 100 years ago. Approximately 20% to 50% of cardiomyopathies in the Western world are caused by alcohol. All cellular substructures can be adversely affected by acetaldehyde, a degradation product of ethanol: Na/K ATPase, mitochondria, contractility via reduction of calcium release from the sarcoplasmic reticulum, and elastic elements.
Arrhythmias: It is very well known that excessive alcohol consumption can lead to the so-called Holiday Heart Syndrome with atrial fibrillation and with signs of heart failure the day after. Compared with individuals with the lowest alcohol consumption, individuals with the highest consumption (men: two alcoholic drinks or more per day; women: one alcoholic drink or more per day) had a 51 percent higher relative risk of atrial fibrillation. This increase in risk was dose-dependent: For each 10 g increase in the amount of alcohol ingested, the risk of atrial fibrillation increased by 8 percent in relative terms. The pathophysiologic changes underlying this association are unclear. Alcohol could increase adrenergic tone, reduce vagal activity, lead to direct structural myocardial damage, or even electrophysiological changes in atrial tissue. Alcohol also lowers the threshold for ventricular fibrillation.
Prolonged excessive alcohol consumption may contribute to the development of hypertension or chronic heart failure, which in turn provides the structural basis for the development of arrhythmias. The type of alcoholic beverage – high-proof, red, white wine or beer – does not appear to be important for arrhythmia risk.
Arterial hypertension: numerous epidemiological studies demonstrate the association between chronic alcohol consumption (more than two alcoholic beverages per day) and hypertension, independent of obesity and smoking, as well as a decrease in blood pressure after reduction of consumption (≤2 alcoholic beverages per day). Several mechanisms have been postulated: Increase in sympathetic activity, decrease in baroreceptor sensitivity, decrease in sympathetic activity, decrease in baroreceptor sensitivity, decrease in ionized magnesium in plasma with consecutive increase in ionized calcium, leading to vasoconstriction.
Cerebrovascular insults: arterial hypertension, atrial fibrillation, and cardiomyopathy are risk factors for cerebrovascular insults, which are correspondingly more common in alcoholics. Cerebral hemorrhages are also more common in heavy drinkers. Increased bleeding time, low platelet aggregation, and tendency to fall probably play a major role.
Conclusion
To illustrate the problem of alcohol, Zakhari proposes the image of the Roman god Janus: A forward and backward looking double face: the effect of alcohol can have opposite forms, depending on the amount consumed: with moderation (2-3 drinks/day) a protective effect against coronary heart disease can be observed. However, no definite difference can be found between wine, beer or liquor, but the wine drinkers have a healthier lifestyle. Moderate alcohol consumption, however, cannot simply be defined by quantity: Seven drinks on the weekend do not have the same effects as one drink per day. The downside of alcohol is the negative effects of alcohol abuse on the heart: cardiomyopathy, arrhythmias, hypertension, and cerebrovascular insults. Calorie intake must not be forgotten. Ultimately, the quote from Paracelsus still applies: Sola dosis facit venenum.
Further reading:
- Mukamal KJ, et al: N Engl J Med 2003; 348: 109-118.
- Naimi TS, et al: Am J Prev Med 2005; 28369-73.
- Sam Zakhari, ALCOHOL HEALTH & RESEARCH WORLD, Vol. 21, no. 1, 1997. https://pubs.niaaa.nih.gov/publications/arh21-1/21.pdf
CARDIOVASC 2017; 16(1): 4-6