
At this year’s Melanoma Congress in Hamburg, the question was raised whether the most commonly used treatment options for actinic keratosis (AK) are the most effective and cost-effective. Furthermore, the advantages of a holistic approach for targeted therapy were emphasized: AK does not only consist of isolated lesions, but is predominantly an area disease, which must also be addressed as such.
Diagnosis of actinic keratosis (AK) is usually clinical, according to Prof. Bruce H. Thiers, MD, Charleston. However, there are different subtypes here: keratotic, atrophic, hypertrophic, verrucous, cornu cutaneum, pigmented or lichenoid. Histopathological examinations are sometimes necessary to exclude squamous cell carcinoma (SCC). Histologic subtypes include adnexal involvement and acantholytic process.
“AKs can be precancerous, but equally the first intra-epidermal manifestation of non-melanocytic skin cancer (NMSC). The fact is that the incidence of NMSC is significantly increased in individuals with AK,” said Prof. Thiers.
The concept of surface disease
“Most often, such lesions occur on light-damaged skin sites and occur areally. All stages of this disease (from subclinical AK to SCC) may coexist simultaneously. It is useful to speak of an areal disease: The transitions between normal and photodamaged skin and between AKs and SCCs are smooth. Field cancers must be recognized and addressed early” (Table 1). Classic techniques to assess such diseased areas are:
- Physical inventory
- Histopathological examinations
- Dermoscopy
- Reflection confocal microscopy.
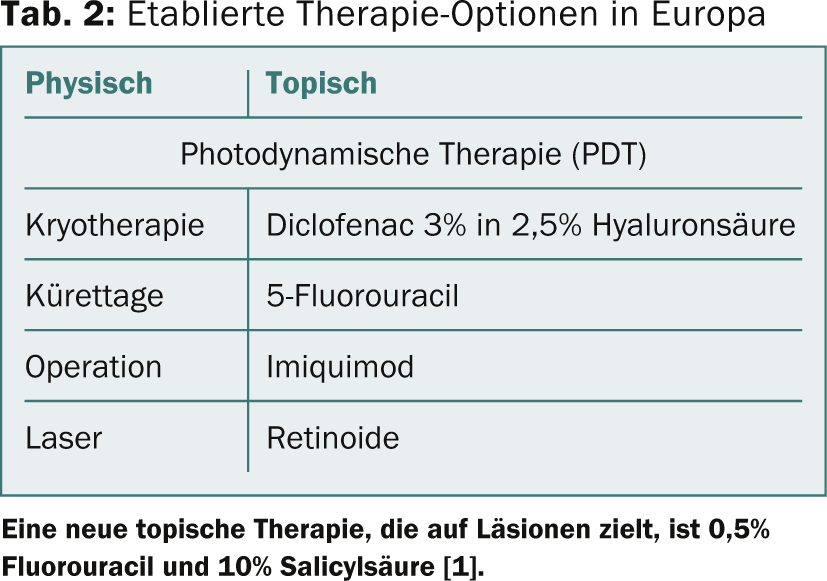
“Physical or ablative therapies that directly target the entire field include chemical peeling, dermabrasion, and laser or photodynamic treatments. Topical options include diclofenac, 5-fluorouracil, imiquimod, ingenol mebutate and tretinoin,” Prof. Thiers summarized.

How good is cryotherapy?
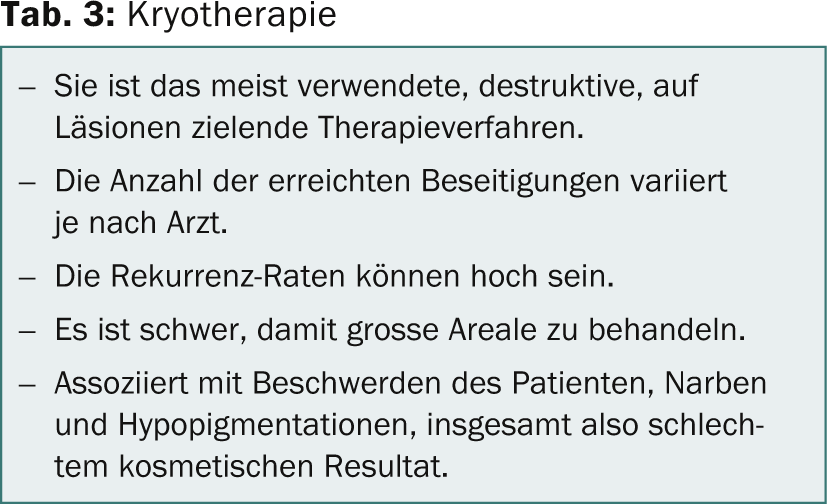
Overall, various procedures are established in the treatment of AK throughout Europe (Tab. 2), including cryotherapy, which is, however, lesion-oriented and does not affect the entire field. “It is often used for single, clinically visible lesions because it is a quick and easy method. However, it is also associated with post-therapeutic hypopigmentation and a so-called checkerboard effect. Furthermore, the efficacy of cryotherapy is variable, difficult to standardize between different physicians, and dependent on the duration of cryogenic application as well as the technique. Recurrence rates are unclear,” explained Prof. Jan-Christoph Simon, MD, Leipzig. Even after repeated cryotherapy, many patients continue to have numerous AK lesions. The procedure is unsuitable for treating large areas (Tab. 3).
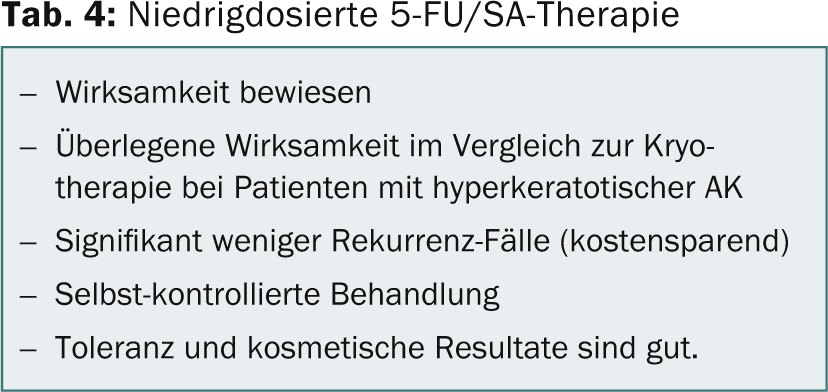
“New studies, not yet published, suggest that low-dose, short course 5-FU/SA therapy (0.5% fluorouracil, 10% salicylic acid) provides significantly better histologic and complete clearance compared with cryotreatment, and also significantly lower rates of recurrence. Furthermore, the procedure is effective against AK-III lesions (Tab. 4),” said Prof. Simon. “So it’s time for physicians to question their habits in treating AK.”
Economic considerations
The importance of AK from an economic point of view was presented by Prof. Dr. med. Matthias Augustin, Hamburg: “Very few studies have so far investigated the economic burden of this disease. A meta-analysis from 2004 calculated the direct and indirect costs of AK management for the U.S.: It comes to considerable values of 1.2 billion and 295 million U.S. dollars, respectively. The main cost drivers are physician visits and related procedures.”
Other North American data from 2002 show that 8.2 million physician visits are required annually in this context, and the financial burden increases significantly if progression to NMSC, particularly SCC, occurs. As the incidence of NMSC continues to grow, significant cost increases must also be expected in the future [2].
“For more than six AK lesions, topical treatment with low-dose (0.5%) rather than high-dose (1 or 5%) 5-FU appears to be the most cost-effective [3]. Compared with other forms of therapy, the use of 5-FU also has a good cost-benefit ratio. The overall cost of low-dose 5-FU/SA therapy is ultimately lower than that of cryotherapy. Regarding combination therapies, the greatest financial burden arises from a joint application of imiquimod and cryotherapy. Sometimes this is because cryotherapy often requires multiple treatments,” Prof. Augustin concluded.
Source: “Making proper judgment when choosing a treatment for actinic keratosis,” Symposium at the 8th World Congress of Melanoma, July 17-20, 2013, Hamburg, Germany.
Literature:
- Stockfleth E, et al: Low-dose 5-fluorouracil in combination with salicylic acid as a new lesion-directed option to treat topically actinic keratoses: histological and clinical study results. British Journal of Dermatology 2011; 165( 5): 1101-1108.
- Housman TS, et al: Skin cancer is among the most costly of all cancers to treat for the Medicare population. J Am Acad Dermatol 2003 Mar; 48(3): 425-429.
- Gupta AK, et al: The Management of Actinic Keratoses in the United States With Topical Fluorouracil: A Pharmacoeconomic Evaluation Cutis 2002; 70(2): 30-36.
InFo Oncology & Hematology 2013; 1(1): 41-42.









