
Onychomycoses remain difficult to treat despite highly effective antifungal agents. How to proceed with the most common nail disease ever?
Infections of the nail organ with fungi are commonly referred to as onychomycoses. They represent a group of different diseases, which differ in pathogen, duration and especially the primary diseased nail structures. This differentiation is particularly important for therapy.
Pathogen spectrum
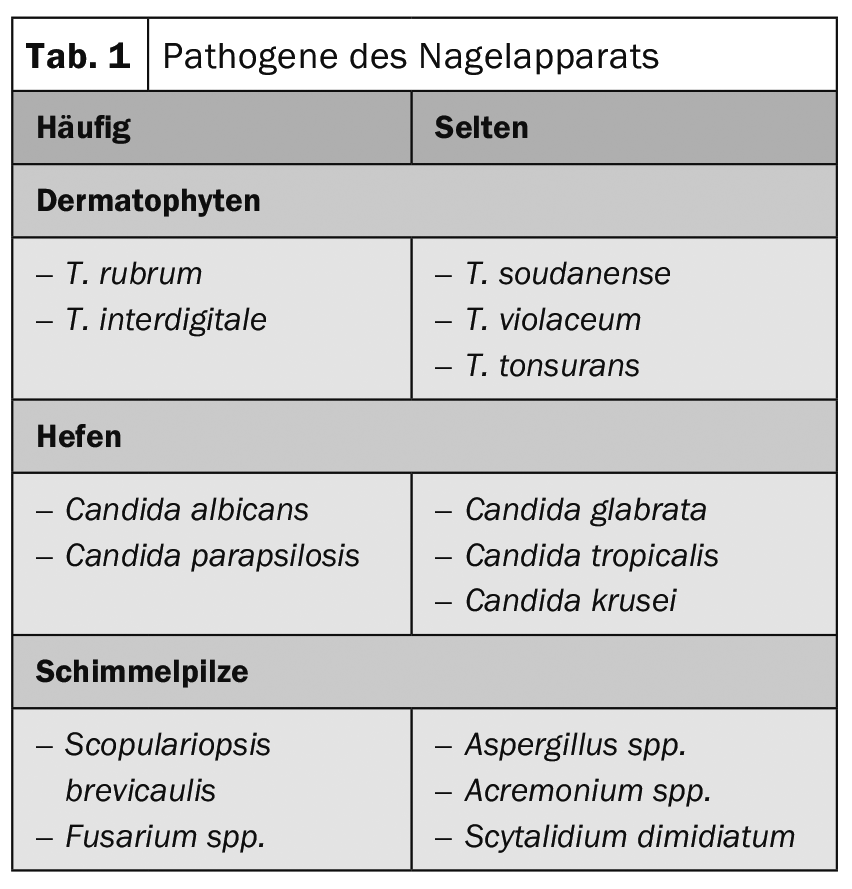
The most common pathogens of classic onychomycoses are dermatophytes, which possess special enzymes for digesting keratin. By far the most common dermatophyte is Trichophyton (T.) rubrum, followed by T. interdigitale (mentagrophytes) . All other dermatophytes cause onychomycosis much less frequently. Among yeasts, Candida species are the most common – they are preferably found in chronic paronychia of the fingers. Molds have long been controversial as pathogens, but species that were once very rare are now being observed with increasing frequency, e.g., Fusarium species. In most cases, it is not possible to identify the causative agent from a clinical point of view (Table 1) [1].
Frequency
The prevalence of onychomycosis is reported very differently. Men appear to be slightly more likely to develop the disease, e.g. a prevalence of 2.6% for women and 2.8% for men was found in the UK. Overall, approximately 3-8% of the population is thought to have onychomycosis, but frequencies of 8-40% have been demonstrated in various occupational groups. Nail infestation is found in 20-30% of patients with tinea pedum. The incidence increases proportionally with age [2]. Apparently, there is an autosomal dominant susceptibility to onychomycosis, meaning that vertical spread is preferentially observed in the family [3]. Psoriasis sufferers are more likely to have a nail fungus infection. Toenails are affected seven to ten times more often because of their three times slower growth. In immunocompromised patients, rare pathogens must always be considered, which are often very difficult to treat. Mixed infections account for approximately 5% of all onychomycoses [4].
Onychomycosis types
The differentiation of onychomycoses (OM) according to the route of infection and the resulting clinic is clinically useful because it also explains the severity and helps determine the prospects of treatment [5].
By far the most common form is distal-lateral subungual OM, in which the pathogenic fungus penetrates from the skin of the tip of the finger or toe into the hyponychium and from here into the nail bed. Initially, there is mild hyperkeratosis of the distal nail bed, which slowly increases and may lift the nail. Gradually, the distal part of the nail becomes cloudy and opaque. Histologically, it can be seen that the fungi are predominantly located in the subungual keratosis and the overlying nail is a barrier rather than the main target of infection. The fungus slowly spreads proximally and may reach the matrix (Fig. 1-3) . The proximal border is very often irregularly shaped. A yellow stripe tapering proximally occasionally develops under the toenails – it is extremely rich in fungi, which here consist of spores and very short fungal filaments and have a very thick cell wall. This phenomenon is also called dermatophytoma. After often lasting for years, the entire nail can be affected and eventually destroyed.

White superficial onychomycosis (WSO) is characterized by chalky white irregular patches on the surface of toenails. It is predominantly caused by T. mentagrophytes . This classic form must be distinguished from the rarer WSO of the fingernails, which is caused by T. rubrum and is found almost exclusively in AIDS patients. Here the white coloring is cloudy rather than chalky.
Another form of OM is proximal white subungual OM, in which the fungus spreads across the cuticle and along the underside of the proximal nail wall toward the matrix. When it is reached, the fungus becomes properly embedded in the newly formed nail and can penetrate all layers of the nail. This impairs the optical coherence of the nail plate and the nail appears white.
A rare form is endonyx OM. Pathogens are almost exclusively T. soudanense and T. violaceum, which are also known pathogens of tinea capitis. Here, only the nail plate is affected. Histologically, the fungi are seen in the middle layers of the nail.
Candida albicans has enzymes that can also cleave keratin. In warm countries, an infection very similar to distal subungual onychomycosis may be produced, but in temperate climates it is usually an infection of the proximal nail with paronychia. In neonates, Candida albicans occasionally causes proximal subungual OM.
All different forms of OM can develop into total dystrophic OM, in which the nail is completely destroyed. From the beginning, the nail infection occurring in the context of chronic mucocutaneous candidiasis is totally dystrophic [6].
Differential diagnosis
The most important differential diagnosis is nail psoriasis (Fig. 4), which has many clinical and histologic features in common with OM. Spotting, pitting, oil spots, distal onycholysis, and yellowing are characteristic. On the toes, mechanically induced onycholysis is often found due to overlapping toes and friction. Lichen planus unguium shows predominantly longitudinal grooves and surface defects and is prone to irreversible scarring with pterygium formation. In nail eczema, irregular pits and transverse grooves and ridges are found, as well as often paronychia due to involvement of the nail wall. The so-called “20-nail syndrome” occurs preferably in children and is characterized by rough nails. It may be idiopathic or occur in the setting of atopic eczema, psoriasis, or lichen planus. Onychogryposis is characterized by a massive thickening of mostly the toenails, occasionally mycotically infected. Pseudomonas aeruginosa also likes to colonize fungus-infected nails. It is not uncommon for psoriasis nails to have an additional fungal infection, and mycosis is also possible in other nail diseases. Paronychia is more often due to allergies than to Candida. It can also be difficult to differentiate artifacts, such as compulsive retraction of the proximal nail wall or onychotillomania.

Diagnostics
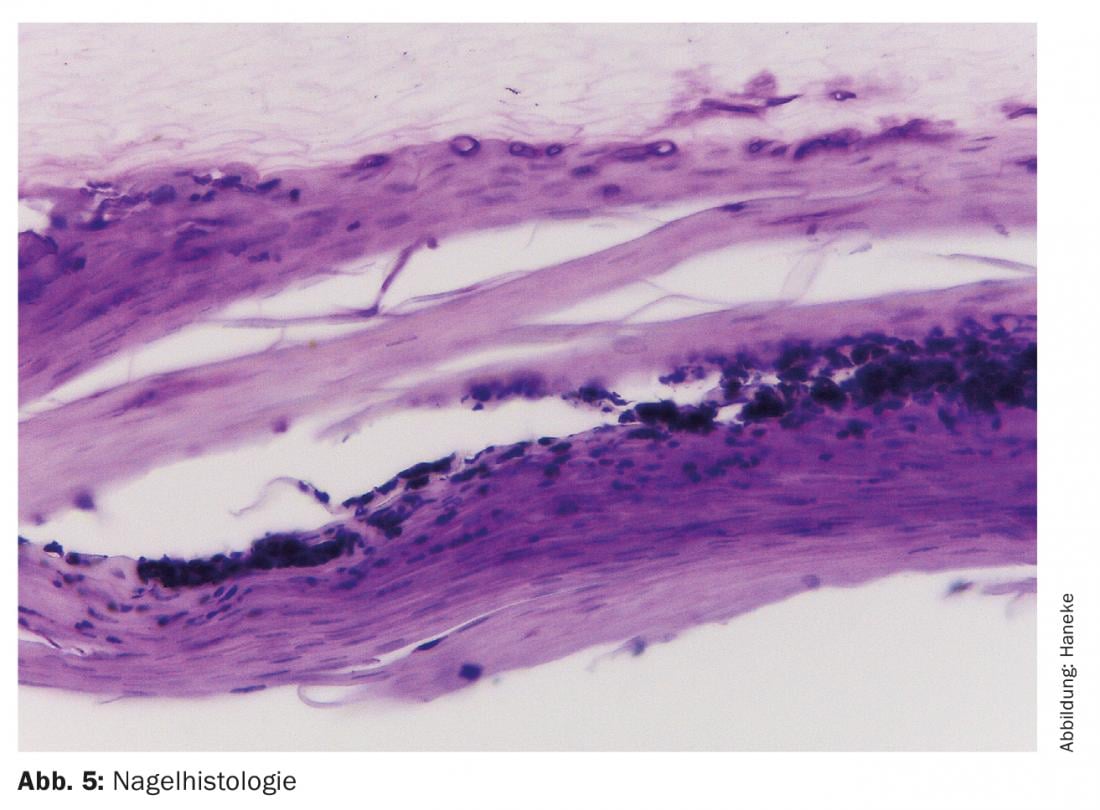
If onychomycosis is suspected, the diagnosis should always be confirmed, e.g. by a direct preparation, culture or/and nail histology. The latter is about twice as likely to be positive as culture, which is often falsely negative, and it can distinguish between contamination and true infection (Fig. 5) [7]. Material should be collected from the proximal edge of the infection under the nail in distal-lateral subungual onchyomycosis (DLSO), scraped from the nail surface in WSO, and a punch from the nail plate can confirm the diagnosis in proximal subungual OM. Newer techniques include polymerase chain reaction (PCR) and matrix-assisted laser desorption ionization/”time-of-flight” mass spectroscopy (MALDI-TOF), but these are expensive and not yet widely available. Not only the detection of fungi in general, but also the differentiation of the various pathogenic fungi is of great importance for treatment. If mycological tests are negative and fungal infection is still suspected, the tests should be repeated. A positive result is also the justification for the usually prolonged antifungal therapy.
Treatment
Onychomycoses are the most difficult mycoses of the skin to treat, and therapy usually takes the longest. Basically, it includes general hygienic measures as well as mechanical, topical and systemic treatments.
Keeping the feet dry, treating tinea of the surrounding skin and avoiding airtight shoes are important, especially for recurrence prevention. In paronychia, contact with moisture should be minimized and avoided altogether with meat, fish, fresh vegetables and fruits.
Thickened nails and subungual hyperkeratosis should be removed mechanically as much as possible, preferably after softening the horny masses with 40% urea paste. The surrounding skin is taped off with plaster and the paste is applied to the nail as thick as the back of a knife, then left under an occlusive dressing for three to five days. Diseased parts of the nail soften much faster and can be easily cut or scraped off. Generally, this needs to be repeated a few times until all the infected material is removed. This is followed by the actual fungal treatment.
According to general consensus, local treatment alone is only useful for infestation of a maximum of one third of the nail and when the matrix has not yet been reached. Antifungal solutions and creams are not effective. Amorolfine 5% and ciclopirox 8% are available in varnish form. Amorolfine varnish is applied once a week, and ciclopirox is applied daily. A novel water-soluble coating base based on hydroxypropyl chitosan appears to be superior. Nevertheless, the cure rates of varnish treatment alone, even after prior chemical nail lavulsion, are only 5 to a maximum of 15%. New drugs for topical OM treatment are efinaconazole 10% and tavaborole 5%. They are approved in the U.S. and are very expensive; success rates are slightly better than with the coatings available here. Luliconazole for nail treatment is also available in Japan. Terbinafine 10% in varnish base is not commercially available but has been tested on various occasions.
Systemic treatment with antifungal agents is superior to local therapy [8]. The first orally active agent against dermatophytes was griseofulvin, which is, however, practically hardly used today. Cure rates were low and treatment duration was very long. The first systemically used azole preparation was ketoconazole, which caused isolated severe idiopathic liver toxic reactions and is now marketed only for other indications. Success in the treatment of onychomycosis and chronic mucocutaneous candidiasis has been impressive. The follow-up drug itraconazole is now the broad-spectrum antifungal agent against dermatophytes, yeasts and molds. For fingernail mycoses, a treatment period of two to three months is recommended, and for toenails, three to four months. The so-called pulse therapy with 400 mg/day for one week per month is equal to the continuous therapy with 200 mg daily and saves half of the substance. Tolerance of itraconazole is generally very good; interference with other drugs is possible. The drug of choice for dermatophyte onychomycosis is terbinafine, which is recommended at 250 mg daily for two to three months for finger and three to four months for toe onychomycosis. In comparative studies, terbinafine was clearly superior to both itraconazole and fluconazole. Fluconazole was recommended as an alternative at the dosage of 150-450 mg/week and should be given until cure. Despite good in vitro values, cure rates of oral antifungals have fallen short of expectations.
Various studies have shown that combined topical and oral treatment with varnishes and tablets is clearly superior to monotherapy. This applies to terbinafine and itraconazole as well as to amorolfine and ciclopirox.
Lasers have been approved for “temporary improvement of nail appearance” by the FDA. Critical studies have shown no effect beyond the cosmetic [9].
Recurrence prophylaxis
Patients with onychomycosis have a very high risk of relapse even after healing. On the one hand, this may be due to subclinical residues of the fungal infection, inadequately treated mycosis of the surrounding skin, persisting predisposing factors such as inadequate peripheral circulation, traumatic nail damage, immunodeficiencies, etc., but on the other hand, it may also be due to re-infection in the patient’s own household, where horny scales have remained, in which fungal spores can survive for more than 20 years. Therefore, a long-term topical treatment, the use of antifungal powders for the shoes and disinfection appear useful [10].
Outlook
Onychomycoses still represent a therapeutic challenge despite highly effective antifungal agents. They should still be treated, as they are much more than a cosmetic problem. It is hoped that research will continue to find well-tolerated and highly effective drugs.
Literature:
- Haneke E: Fungal infections of the nail. Semin Dermatol 1991; 10: 41-53.
- Burzykowski T, et al: High prevalence of foot diseases in Europe: results of the Achilles Project. Mycoses 2003; 46: 496-505.
- Zaias N, et al: Autosomal dominant pattern of distal subungual onychomycosis caused by Trichophyton rubrum. J Am Acad Dermatol 1996; 34: 302-304.
- Denning DW, et al: Fungal nail disease: a guide to good practice (report of a Working Group of the British Society for Medical Mycology). Br Med J 1995; 311: 1277-1281.
- Haneke E: Nail biopsies in onychomycosis. Mycoses 1985; 28: 473-480.
- Baran R,et al: A new classification of onychomycoses. Br J Dermatol 1988; 139: 567-571.
- Haneke E: Significance of nail histology for the diagnosis and therapy of onychomycosis. Ärztl Kosmetol 1988; 18: 248-254.
- Gupta AK, Daigle D, Folley KA: Network meta-analysis of onychomycosis treatments. Skin Append Dis 2015; 1: 74-81.
- Gupta AK, Simpson FC: Laser therapy for onychomycosis. J Cutan Med Surg 2013; 17: 301-307.
- Baran R, et al: Onychomycosis.2nd ed. Taylor & Francis, Oxon 2006.
DERMATOLOGIE PRAXIS 2019; 29(1): 17-20









