
Lunate malacia is a disease of a carpal bone in which all or part of the os lunatum necrotizes. This progressive disintegration of the small bone bellows in the lunar bone is caused by a lack of blood circulation. Possible causes of these circulatory disorders are, in addition to a corresponding predisposition, extreme pressure loads (e.g. from compressed air machines) or accidents. Prompt use of imaging is indicated for suspected diagnosis of lunate malacia.
The wrist joint has a complex structure and is subject to considerable mechanical stress every day due to numerous movements and force influences. These can add up to an osseous circulatory disorder. The Os lunatum, the lunate bone of the wrist, is frequently affected. As a result, aseptic osteonecrosis may develop, lunate malacia. Also known as Kienböck’s disease, osteonecrosis is the most common of the upper extremity [1,3,4]. The bilateral occurrence is rather rare.
The cause is thought to be vascular pathology leading to infarction of the bone. Ulnar minus variants may predispose to lunate malacia with a correlation of 78%. The disease has its peak age between 20 and 40 years. Men are affected twice as often as women. The symptomatology is in Overview 1 summarized. Overview 2 shows the differential diagnoses according to the clinical symptoms.
If there is a corresponding clinical suspicion of lunate malacia and also a possible occupational history (construction worker, jackhammer), imaging diagnostics should be performed as soon as possible. The radiographic classification (according to Lichtman) includes 4 stages, to which the staging in MRI diagnostics is also based [2]. The early form (degree I) with cancellous bone edema cannot be detected radiographically and can only be visualized by magnetic resonance imaging. From stage II, changes in the shape and contour of the os lunatum are then present.
The advantage of cross-sectional imaging is also to better visualize perilunate changes with malpositions of the adjacent carpal bones than x-rays in 2 planes. At the stage IIIb there is a structural disturbance of the carpus with proximal migration of the Os capitatum and rotational malposition of the Os naviculare to palmar. Stage IV progresses to osteoarthritis with complex articulation dysfunction centered in the radiocarpal compartment of the wrist. Often, corpora libera and chondromatosis are also detectable.
The therapeutic consequences depend on the stage of the disease. Immobilization and NSAID preparations are used in the early phase of lunate malacia. Discharge also helps to prevent transient ischemia of the bone from the M. Kienböck to differentiate. If the course is frustrating, various surgical treatments are possible and indicated already from stage II.
Radiographs are unable to demonstrate cancellous edema in the early stages of lunate malacia. In the course, however, deformations and fragmentations can be verified radiographically. The length variants of the ulna are very easy to detect radiographically.
Computed tomographic examinations are very good at documenting bony changes in the carpus with primary axial scans and subsequent multiplanar reconstruction, especially demonstrating small fragments or even perilunate disintegration of the bones.
Magnetic resonance imaging is a valuable tool, especially in the early phase of lunate malacia, to detect cancellous edema and accompanying synovitis, including possible lesions of the small ligaments. This is not possible with any other imaging technique. Also, avital spongiosa districts can be detected in the course. The method also represents the standard procedure for therapy control.
Case studies
In case report 1 , a 58-year-old Russian-German with occupational history of heavy physical activity shows, in addition to significant degenerative changes in all joints of the hand, incipient sintering of the os lunatum without fragmentation (Fig. 1), compatible with lunate malacia.

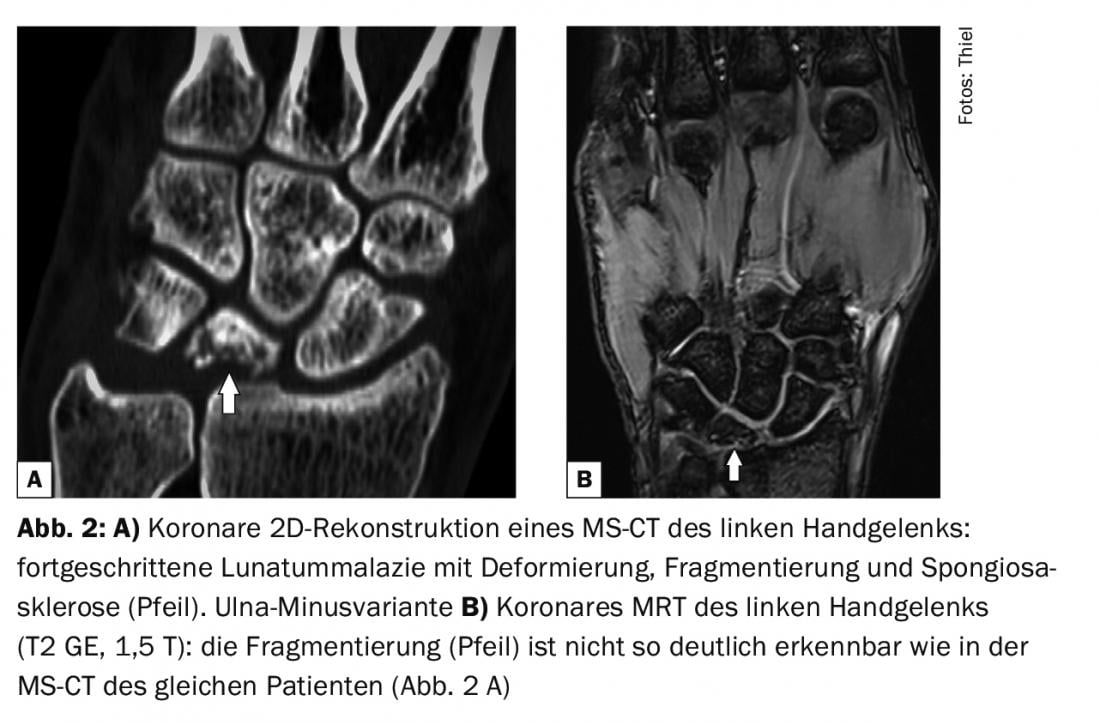
Case report 2 documents advanced lunate malacia with computer and magnetic resonance imaging diagnosis in an athletic 38-year-old man after bicycle fall 10 months earlier. Progressive pain, limited wrist motion, and swelling prompted preoperative diagnostic imaging (Fig. 2A and B).
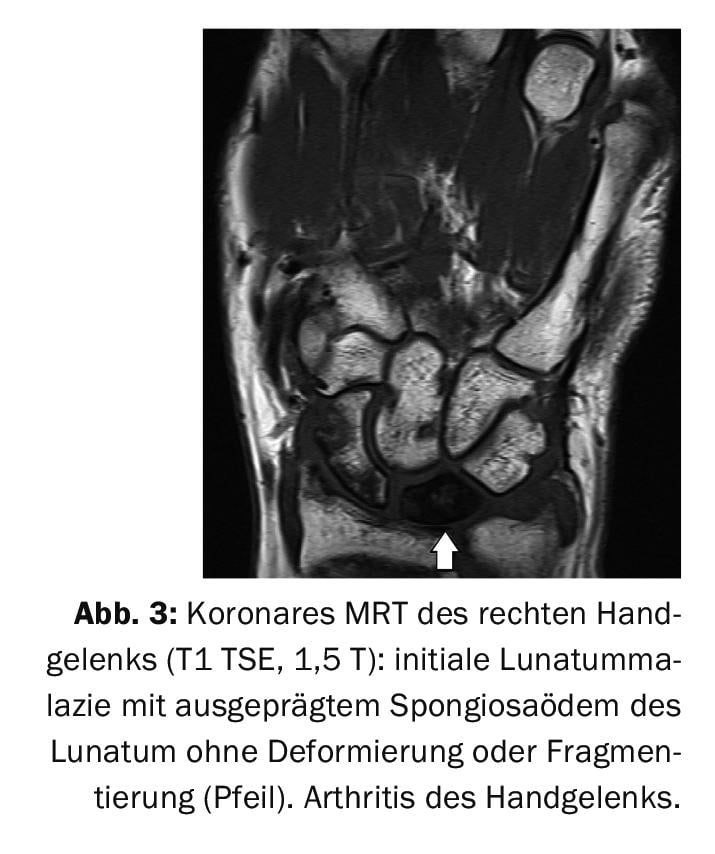
Case report 3 shows a 65-year-old man also with post-traumatic lunate malacia with deformity and significant edema of the cancellous bone (Fig. 3) with wrist arthritis including destruction of the TFCC (triangulated fibrocartilaginous complex).
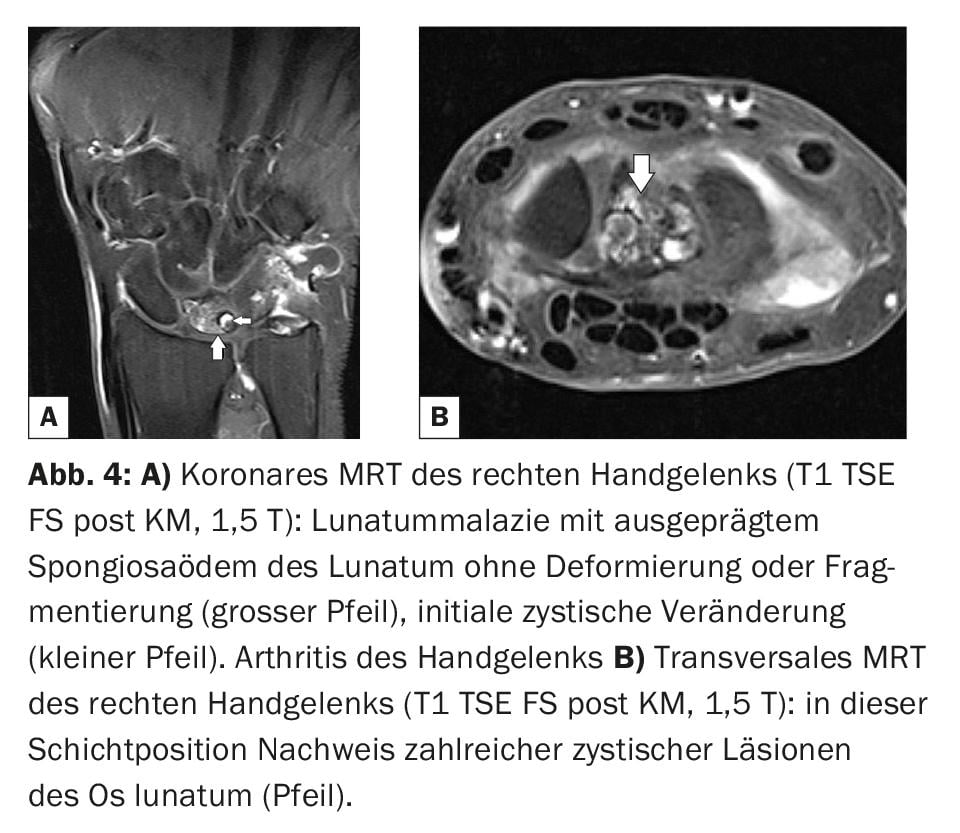
In case report 4 , inflammatory activated osteoarthritis of the wrist of a 61-year-old female patient from agriculture also shows evidence of lunate malacia (Fig. 4A and B).
Take-Home Messages
- Lunate malacia is an aseptic osteonecrosis, the most common in the upper extremity.
- The main age of manifestation is between 20 and 40 years, and men are more frequently affected than women.
- Long-term mechanical stress predisposes to Kienböck’s disease (jackhammer).
- MRI can detect bony disease at all stages.
- Therapy is conservative in the early phase; various surgical techniques are available for progression.
Literature:
- Kristensen SS, Thomassen E, Christensen F: Ulnar variance in Kienböck’s disease. J Hand Surg 1986; 11(2): 258-260.
- Lichtman DM, Lesley NE, Simmons SP: The classification and treatment of Kienbock’s disease: the state of the art and look at the future. J Hand Surg Eur 2010; 35: 549-554.
- Schöffl V: Kienböck’s disease (lunate malacia), www.springermedizin.de/emedpedia (last accessed Jan. 22, 2022).
- Stoller DW: Magnetic Resonance Imaging in Orthopaedics and Sports Medicine.3rd Edition. Volume two. 2007: Lippincott Williams&Wilkins, Baltimore: 1779-1789.
HAUSARZT PRAXIS 2022; 17(2): 34-35









