The plantar fascia is a strand of connective tissue that runs from the lower heel bone to the metatarsophalangeal joint. Inflammation of the tendon plate on the sole of the foot at the level of the tendon insertion on the heel bone can lead to pain, which occurs particularly with pressure and strain. Plantar fasciitis is usually self-limiting but can be long-lasting. Imaging techniques are used in cases of suspected diagnosis or for differential diagnostic evaluation.
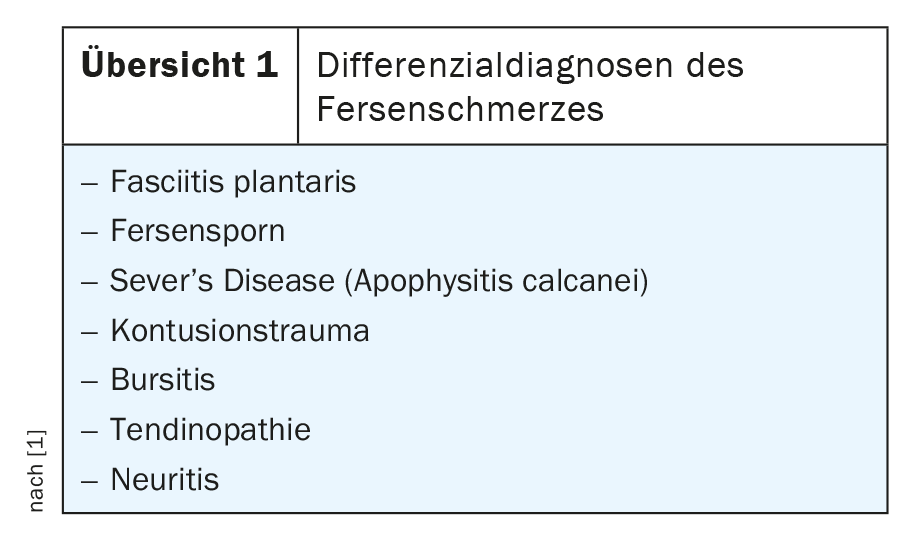
Fasciitis plantaris is a relatively common inflammatory reaction of the plantar fascia that is painful and limits mobility and weight-bearing [4]. Several differential diagnoses [1] must be considered (overview 1) .
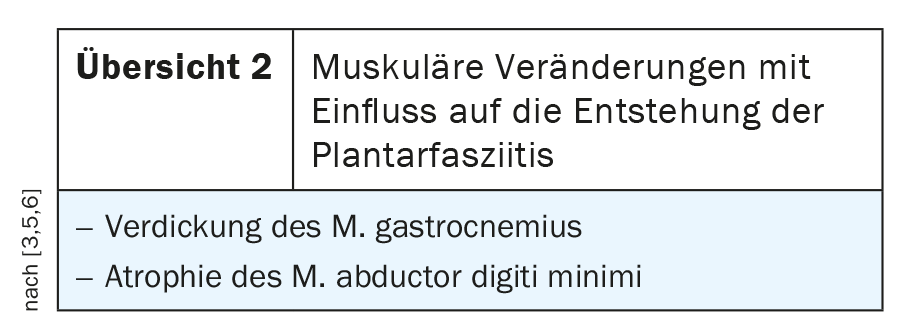
Taking a medical history can at least rule out relevant traumatic causes of the heel symptomatology. Short-term unusual stress [2] should also be recorded as a cause of the plantar inflammatory reaction. MRI studies have also demonstrated the influence of adjacent muscular changes on the development of plantar fasciitis [3,5,6]. These are listed in overview 2. The symptoms are similar to those of plantar calcaneal spurs: stabbing pain when stepping on, dull, irregular pain in the heel area even without weight-bearing, typically also start-up pain especially early in the morning, tenderness at the tendon insertion [9].
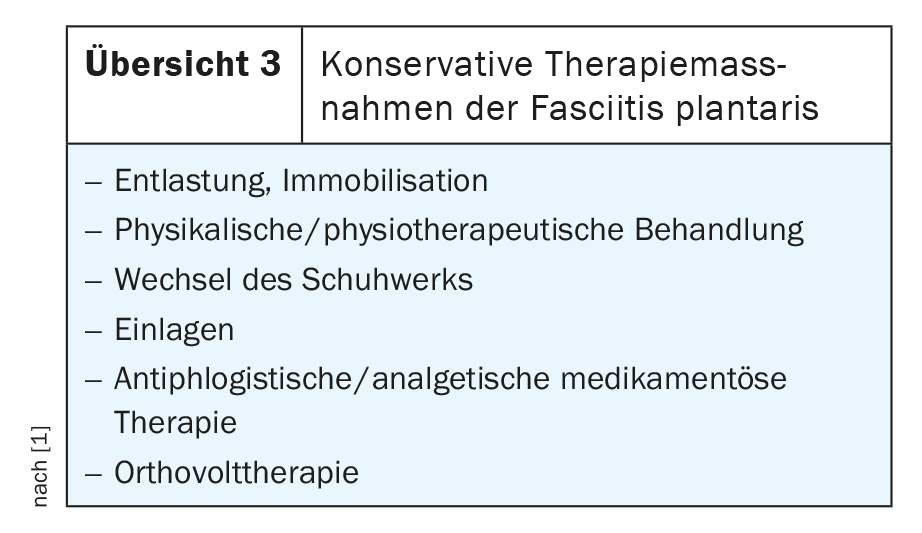
Therapeutically, a wide range of conservative measures is initially available (overview 3).
Surgical treatment should be performed only after conservative treatment has been exhausted.
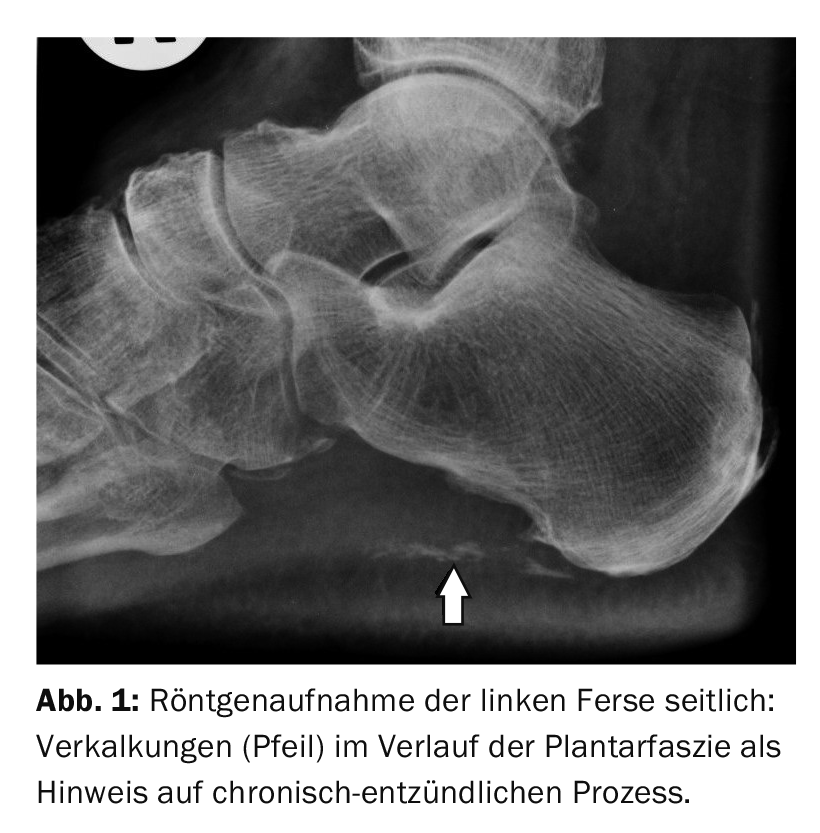
Radiographs in lateral projection cannot capture the inflammatory response of the plantar fascia. If a plantar heel spur is visible, people tend to think that it is the cause of the symptoms. However, it is important to remember that fasciitis and spur can occur simultaneously. If no heel spur is recognizable, fasciitis plantaris may be suspected as the trigger of the load-dependent complaints, often also in combination with rarefying fibroostitis calcanei. Calcifications in the area of the plantar fascia indicate a chronic inflammatory course (Fig. 1).
Sonographically, the plantar fascia can be delineated in the insertion area at the calcaneus as a maximum 4 mm thick double line, more echo-rich than muscle. Inflammation leads to thickening and reduced echogenicity [7]. Surrounding fluid collections are often detectable when inflammation is pronounced.
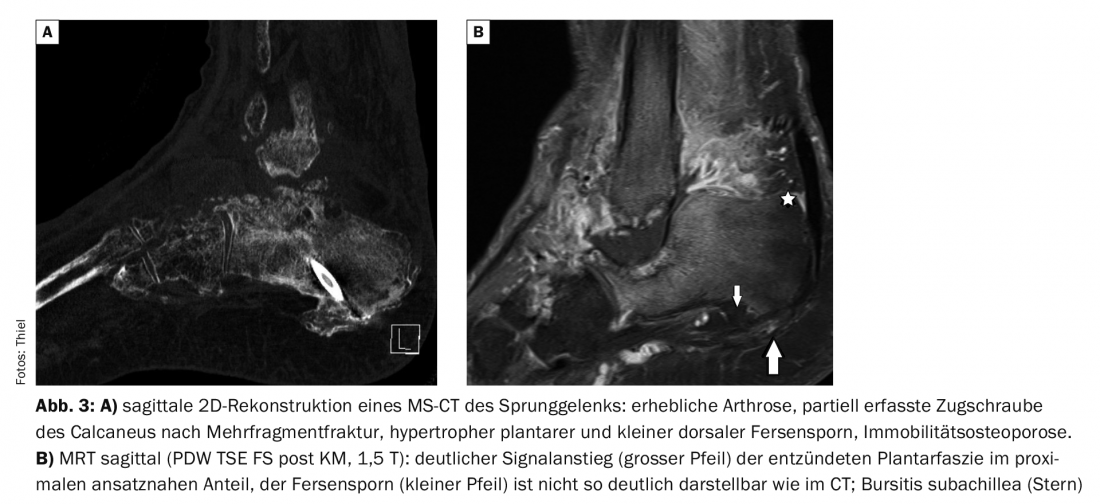
Computed tomographic examinations can visualize associated bony changes, such as the plantar calcaneal spur and calcifications of the plantar fascia, very well (Fig. 3A); the extent of inflammation of the aponeurosis itself is poorly assessable.
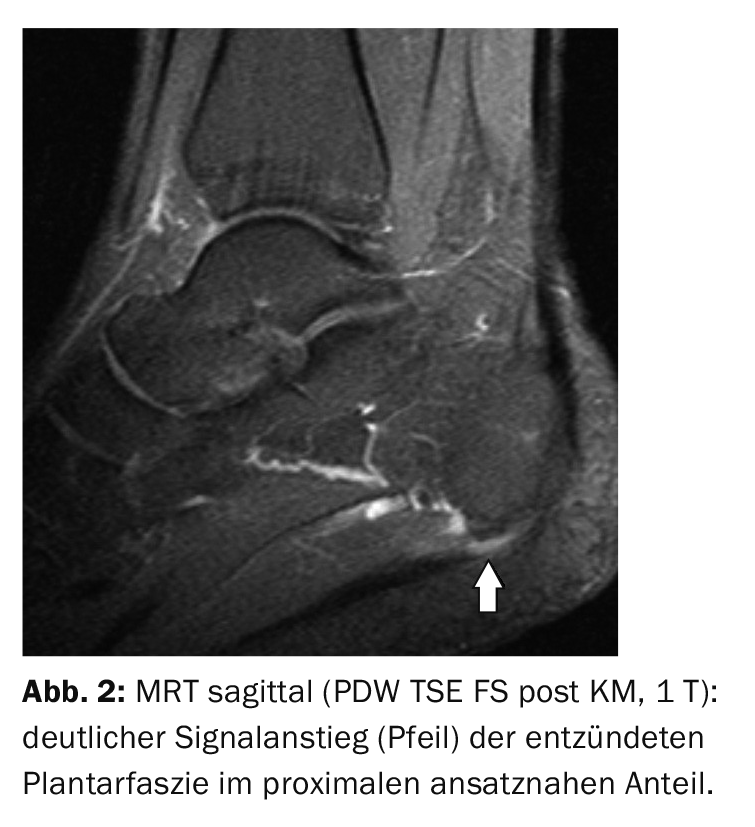
Magnetic resonance imaging already shows fasciitis plantaris (Fig. 3B) in native sequences, especially fat-suppressed sequences [8] . The detection and assessment of adjacent inflammatory soft tissue and bone changes is even better with contrast support.
Case studies
In case report 1, the lateral radiograph of the right heel demonstrates complex enthesiopathy in a 70-year-old patient with load-dependent pain in the plantar and dorsal heel area and in the tarsal area with osteoarthritis. Plantar and dorsal heel spurs as well as calcifications of the plantar fascia and in the attachment of the Achilles tendon are indications of chronic inflammatory degenerative changes.
In case 2, the high soft tissue contrast of MRI and intravenous contrast injection (Gd-DTPA) can reliably demonstrate florid inflammation of the plantar fascia (Fig. 2) . The 67-year-old patient had load-dependent plantar pain that limited her mobility.
Case report 3 demonstrates a 48-year-old man (postoperative condition after calcaneus fracture) with hypertrophic plantar calcaneal spur in addition to significant secondary arthrotic changes of the ankle and tarsal on CT (Fig. 3A). Fasciitis plantaris can only be confirmed on KM-assisted MRI (Fig. 3B).
Literature:
- Agyekum EK, Ma K: Heel pain: A systematic review. Chin J Traumatol 2015; 18(3): 164-169.
- Best N, Smolenski UC: Plantar fasciitis due to driving lessons? Sports Injuries Sports Injury 2012; 26(2): 121-123.
- Chundru U, et al: Plantar fasciitis and calcaneal spur formation are associated with abductor digiti minimi atrophy on mri of the foot. Skeletal Radiol 2008; 37(6): 505-510.
- Cutts S, Obi N, Pasapula C, Chan W: Plantar fasciitis. Ann R Coll Surg Engl 2012; 94(8): 539-542.
- Huerta JP: The effect of the gastrocnemius on the plantar fascia. Foot Ankle Clin 2014; 19(4): 701-718.
- Nakale N, Strydom A, Saragas NP, Ferrao PN: Association between Plantar Fasciitis and Isolated Gastrocnemius Tightness. Foot Ankle Int 2018; 39(3): 271-277.
- Schueller-Weidekamm C. Sonography of the musculoskeletal system. Radiology up2date 1; 2009: 15-29.
- Weishaupt D, Zanetti M. Radiological diagnosis of the foot. Radiology up2date 2; 2002: 237-257.
- Orthopedic Surgery, Rolf F. Oetiker, MD, www.orthozentrum.ch/de/Fuss-Sprunggelenk/Fersensporn-Fasziitis-plantaris (last accessed 05/17/2021)
HAUSARZT PRAXIS 2021; 16(6): 32-33









