With a prevalence of 7% in the Swiss population over 60 years of age, symptomatic gout is a frequently seen guest in the family practice. In men over 40, it is even the most common inflammatory joint disease. Depending on the stage, there are different therapeutic approaches. Fueled by obesity, high meat consumption and lack of exercise, lifestyle changes can often go a long way. However, these modifiable factors take a back seat in the treatment of the acute episode.
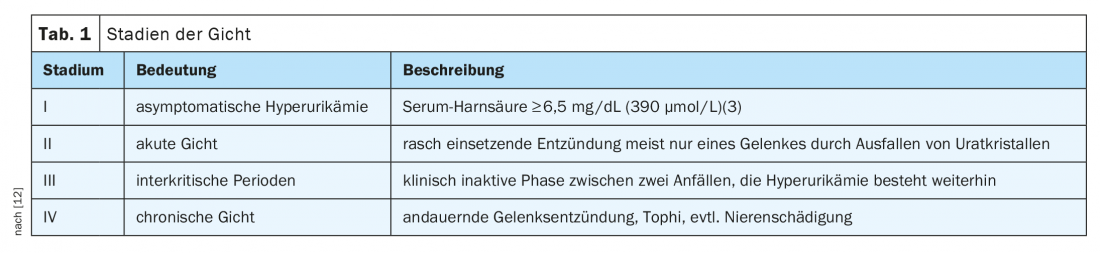
In order to adequately treat gout, knowledge of its stages is essential. In principle, a distinction is made between the four stages of asymptomatic hyperuricemia, acute gout, intercritical periods and chronic gout (Tab. 1). The more the disease progresses, the shorter the asymptomatic intervals become. This is another reason why it is important to treat hyperuricemia despite the absence of symptoms. However, this is often not recognized until the first gout flare, which could often be prevented by appropriate preventive measures.
Prevention and nutrition
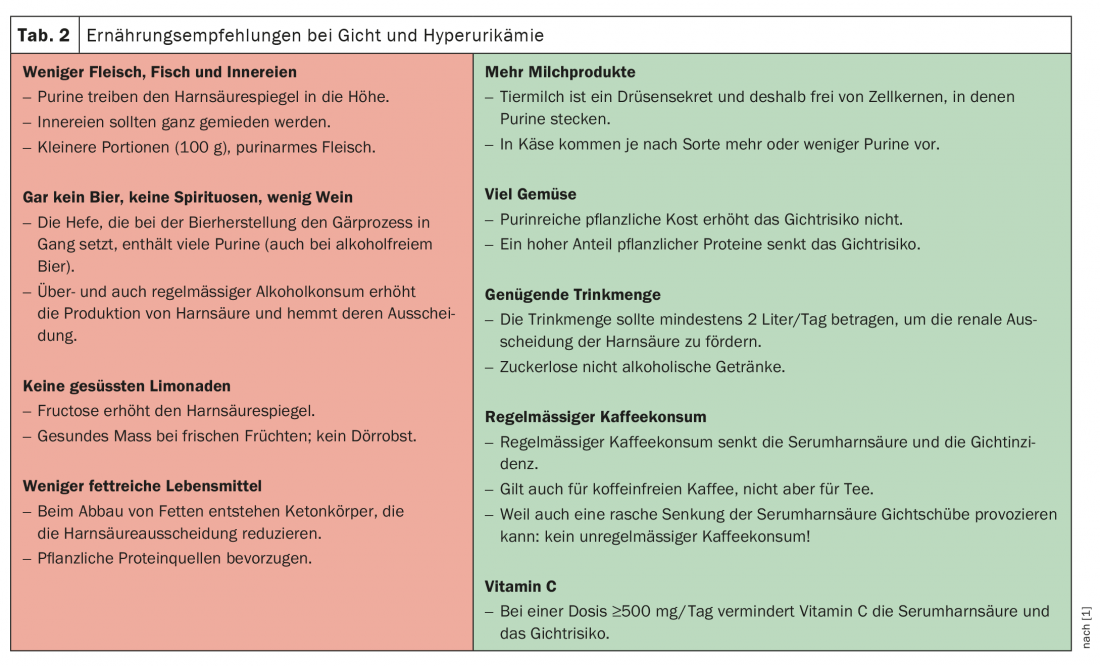
Even if the tendency to hyperuricemia is congenital in primary gout, acute gout attacks can be prevented by lifestyle changes. In case of a positive family history, the determination of the uric acid level is therefore quite reasonable [2]. The preventive measures that can be taken in the case of elevated uric acid levels coincide with the dietary measures that are recommended after an initial attack of gout and also support gout therapy with medication. Every gout patient should receive nutrition and lifestyle counseling [1]. Obesity and weight gain are independent risk factors for gout, whereas weight reduction has a protective effect [4]. A gout diet therefore also targets the frequently associated metabolic syndrome and serves not only to lower serum uric acid. Based on recent observational studies, a traditional low-purine diet, which also prohibits foods that are difficult to eliminate from the menu, is no longer recommended [1,2,5]. Thus, despite the high purine content, a high-protein plant-based diet actually appears to reduce the risk of seizures [5,6]. However, it is still true that meat, fish and offal should be avoided as much as possible [1,2,5]. Further dietary recommendations include increased consumption of dairy products, avoidance of beer and spirits, and restriction of fructose intake (Tab. 2). In addition, care should be taken to ensure adequate drinking of more than 2 liters per day; coffee consumption and vitamin C supplementation appear to have a protective influence [5].
Although weight loss in gout patients is generally considered positive, it must be remembered that not only feasting but also fasting can trigger gout flare-ups. Accordingly, weight loss should be induced slowly and without excessive ketone body production.
Therapy of the gout attack
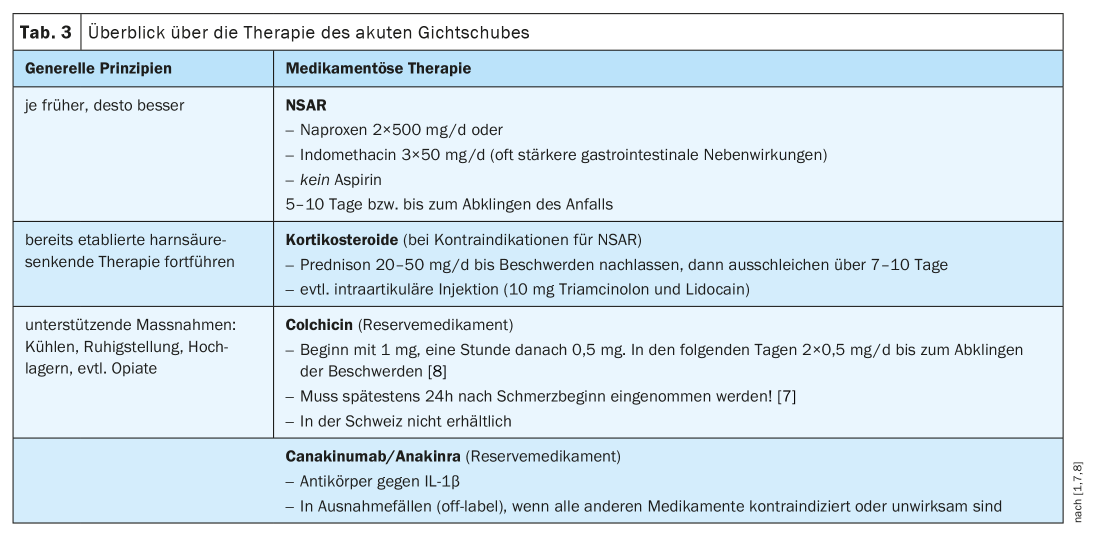
NSAIDs, oral or intra-articular corticosteroids, colchicine, and antibodies against interleukin-1β (canakinumab) are used to treat an acute gout attack (Table 3) [7]. Regardless of the choice of medication, there are some principles that should be followed in any case. This includes treatment as early as possible, continuation of urate-lowering therapy if already established, and implementation of supportive measures.
Gout attacks can last from a few days to several weeks, depending, among other things, on when adequate therapy was initiated [7]. Early treatment is thus crucial for the course, both for the duration of the seizure and for symptom control. Anti-inflammatory medication should be continued for the entire duration of the relapse [7].
Existing urate-lowering therapy should never be interrupted during an acute gout attack, as a pause in treatment provides no therapeutic benefit and reintroduction after an attack has passed may provoke a new exacerbation [7]. Acute gout is treated the same in patients already receiving basic uric acid lowering therapy as in those patients without urate-lowering medication. Uric acid-lowering agents have no benefit in acute treatment.
In addition to anti-inflammatory drug treatment, supportive measures such as cooling and immobilization of the affected joint can also relieve pain. Since various effective substance classes are available for the treatment of acute gout flares, the decision must always be made individually according to the side effect profile and patient risk. If infectious arthritis cannot be excluded by differential diagnosis, glucocorticoids should be avoided, whereas NSAIDs are contraindicated in renal insufficiency. While the other drugs can be discontinued after the episode has subsided, oral glucocorticoids must be phased out slowly to avoid a so-called “rebound flare” [7].
NSAIDs and corticosteroids represent the drugs of choice [1]. Here, primarily naproxen and indomethacin are recommended. Aspirin, on the other hand, is contraindicated because it inhibits uric acid excretion [1]. If there is an increased risk of gastrointestinal bleeding, a proton pump inhibitor can be given prophylactically. Oral therapy with prednisone is recommended for contraindications to NSAIDs [1]. With often very high efficacy, intra-articular steroid injection can also be performed.
Colchicine remains one of the first-line agents according to international guidelines [7], but it is not available in Switzerland. It has the disadvantage of high toxicity and often causes gastrointestinal side effects, especially in the presence of pre-existing renal or hepatic impairment. It must be administered rapidly after symptom onset, but is an alternative to NSAIDs in this case, especially in anticoagulated patients [7]. In cases where all other therapeutic options are contraindicated or fail, a monoclonal antibody against interleukin-1 such as canakinumab or anakinra may be used.
Medicinal prophylaxis of seizures in chronic gout
Although lifestyle modification is recommended for all patients with elevated serum uric acid, asymptomatic hyperuricemia does not require drug treatment [1,9]. The optimal timing of uric acid-lowering therapy is controversial, and so it is also unclear whether starting it while the patient is still having an attack is beneficial [7]. Usually, treatment is started after it subsides. It must be kept in mind that gout attacks may occur more frequently during the first weeks to months of urate-lowering therapy. This is the reason why treatment should not be interrupted during gout attacks. In addition, anti-inflammatory prophylaxis is recommended during the first 6 months [1,7,10]. However, no randomized clinical trials are available for this and this step can certainly be discussed with the patient himself [10]. To keep the risk of gout attacks as low as possible, it is important in any case – with or without anti-inflammatory prophylaxis – to slowly phase in the uric acid-lowering therapy.

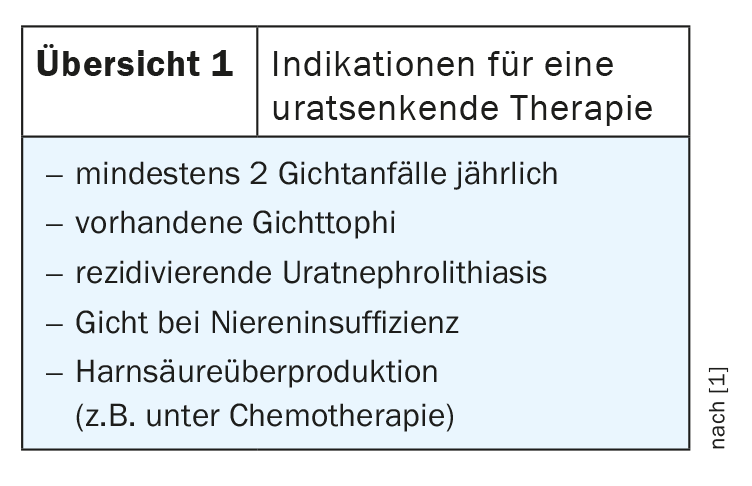
The question of when to start prophylaxis with drugs is a delicate debate. Current indications include at least two gout attacks per year, existing gouty tophi, recurrent urate nephrolithiasis, gout in renal insufficiency, and known uric acid overproduction (review 1) [1]. Various substances are available for the treatment of chronic gout, all of which must be taken on a long-term basis [2,9]. These include so-called uricostats, which inhibit the breakdown of purines to uric acid, and uricosurics, which promote renal excretion. Far less common are uricolytics, which convert uric acid into the more excretible allantoin (Table 4). The goal of treatment is to achieve a uric acid level below the critical threshold at which uric acid begins to form crystals. If gouty tophi are present, the urate should be lowered even further to below 300 µmol/l. However, due to the neuroprotective properties of uric acid, care must be taken to ensure that the level does not fall below 180 µmol/l [1]. Serum uric acid monitoring is recommended 2 to 4 weeks after dose adjustment and annually otherwise [1]. Drug therapy for chronic gout is a long-term therapy, which should be discontinued at the earliest after five years in the form of a discontinuation trial [2]. Continuous treatment with allopurinol is shown to be more effective than intermittent therapy [11] and unfortunately gout often returns after discontinuation of continuous medication. Despite good therapeutic options, this disease is not curable, but adequate therapy allows patients to enjoy a good quality of life.
Literature:
- Huber F, Sajdl H, Beise U: medix Guideline Gout 2017 [updated 12/2017], www.medix.ch/media/gl_gicht_2017_28.5.19_mh.pdf.
- Rheumaliga Schweiz: Gout. www.rheumaliga.ch/rheuma-von-a-z/gicht.
- Schäffler A: Functional diagnostics in endocrinology, diabetology and metabolism: indication, test preparation and performance, interpretation. Springer 2015, 3rd ed.
- Choi HK, et al: Obesity, weight change, hypertension, diuretic use, and risk of gout in men: the health professionals follow-up study. Arch Intern Med 2005; 165(7): 742-748.
- Forster A, Krebs A: Gout – the traditional low purine diet is out. Swiss Journal of Nutritional Medicine 2013; 01/2013: 20(4).
- Teng GG, et al: Food Sources of Protein and Risk of Incident Gout in the Singapore Chinese Health Study. Arthritis Rheumatol 2015; 67(7): 1933-1942.
- Gaffo AL: Treatment of gout flares UpToDate 2020, www.uptodate.com/contents/treatment-of-gout-flares.
- Terkeltaub RA, et al: High versus low dosing of oral colchicine for early acute gout flare: Twenty-four-hour outcome of the first multicenter, randomized, double-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum 2010; 62(4): 1060-1068.
- Perez-Ruiz F: Pharmacologic urate-lowering therapy and treatment of tophi in patients with gout UpToDate 2020, www.uptodate.com/contents/pharmacologic-urate-lowering-therapy-and-treatment-of-tophi-in-patients-with-gout.
- Richette P, et al: 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis 2017; 76(1): 29-42.
- Bull PW, Scott JT: Intermittent control of hyperuricemia in the treatment of gout. J Rheumatol 1989; 16(9): 1246-1248.
- DocCheck Flexikon, https://flexikon.doccheck.com/de/Gicht
HAUSARZT PRAXIS 2020; 15(11): 29-31









