There are no established screenings for endometrial and ovarian cancer. Therefore, any woman with postmenopausal or atypical bleeding premenopausally must be examined and, if necessary, further clarified. Early ovarian cancer is often discovered incidentally. Only cervical cancer can be efficiently screened with PAP smears.
While breast carcinoma is the most common cancer in women in Switzerland, accounting for 32.5% of all new cancer diagnoses, endometrial carcinoma ranks fifth in terms of incidence. Ovarian cancer is slightly less common, but has the higher mortality or worse prognosis. Only in 15th place is cervical carcinoma, the incidence of which has decreased over the past two decades thanks to cervical dysplasia screening. Vulvar carcinoma is even less common, accounting for just under 1% of all new cancer diagnoses in women [1].
The endometrial carcinoma [2–4]
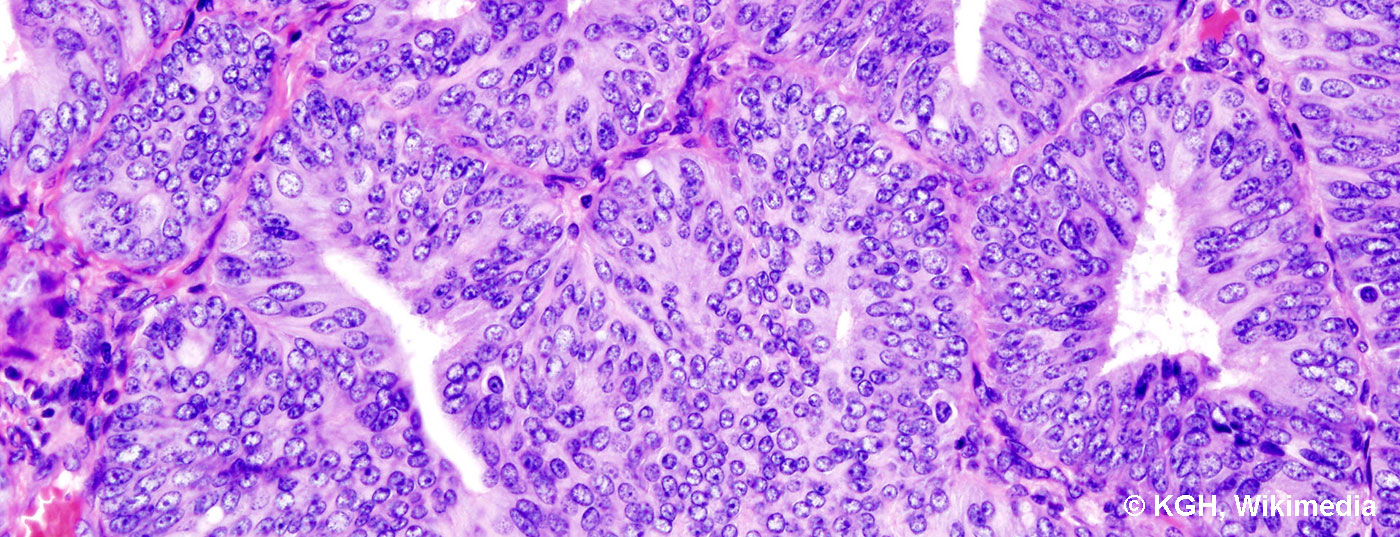
Endometrial carcinoma is considered a carcinoma of the older woman. However, it does occur at younger ages, particularly in the presence of familial tumor syndromes such as hereditary non-polyposis colon cancer (HNPCC or Lynch syndrome). Two types of endometrial carcinoma are distinguished. Type I endometrial carcinoma corresponds histologically to endometrioid endometrial carcinoma, which is estrogen-associated and tends to be well-differentiated and accordingly has a more favorable prognosis. Influenceable risk factor for this carcinoma is metabolic syndrome, especially obesity and hypertension. Type II endometrial carcinoma histologically usually corresponds to a serous or light cell type. It is not estrogen-associated and is comparable to ovarian carcinoma in terms of prognosis and therapy to be performed, i.e., associated with a much less favorable prognosis. There are no typical risk factors for type II carcinoma.
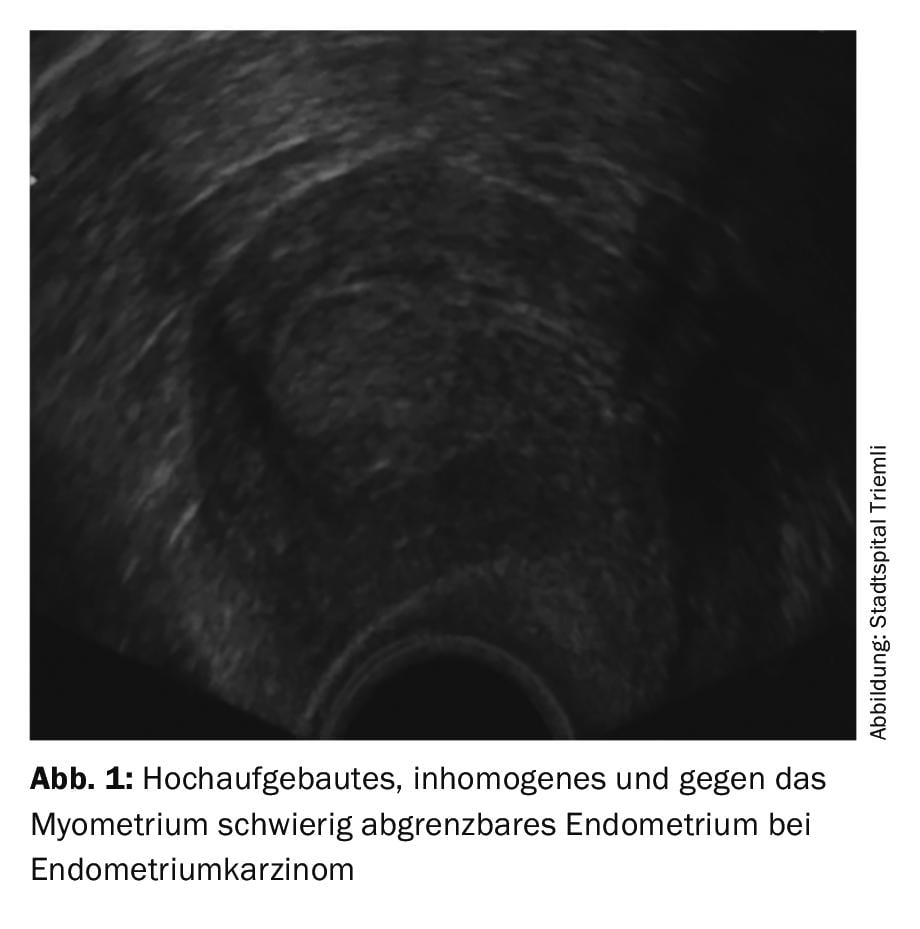
General screening for endometrial cancer or its precursors with transvaginal ultrasound is not recommended in the asymptomatic woman because no benefit has been demonstrated to date. This also applies to women on tamoxifen therapy for breast cancer. However, any woman with postmenopausal bleeding or atypical bleeding in premenopause must be examined gynecologically and by transvaginal ultrasonography and, if necessary, further clarified. It should be noted that type II carcinomas in particular do not always show the typical sonographic image with highly built-up and inhomogeneous endometrium (Fig. 1).
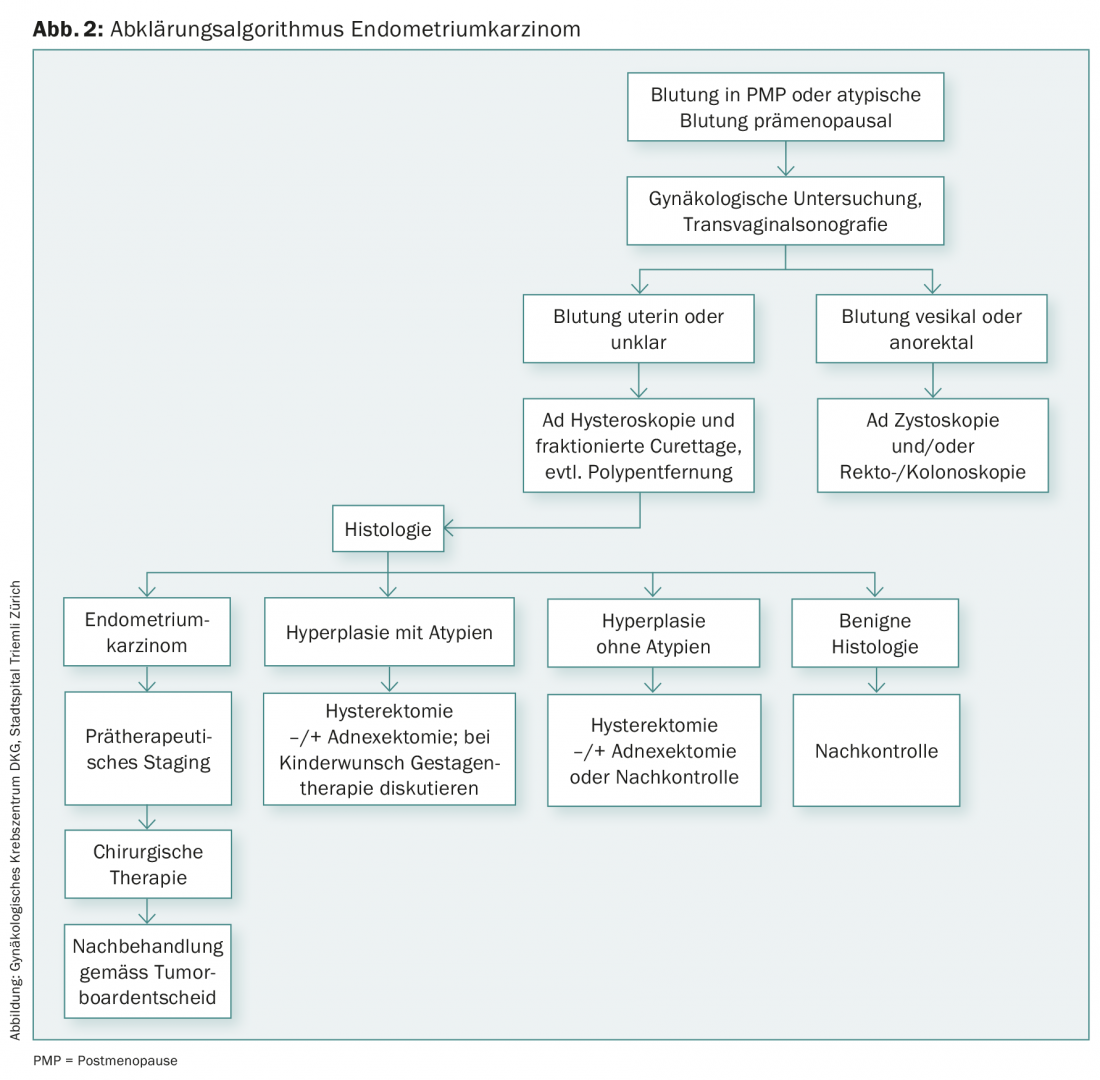
Histological clarification, usually performed by hysteroscopy and curettage, is mandatory, especially in cases of repeated postmenopausal bleeding and in the presence of risk factors such as obesity, hypertension, diabetes mellitus, but also in cases of PCO (polycystic ovaries), HNPCC syndrome or tamoxifen therapy (Fig. 2).
Once the histologic diagnosis is available, radiologic staging, e.g., by computed tomography of the abdomen and thorax, is recommended before definitive therapy is undertaken. Treatment of endometrial carcinoma consists primarily of hysterectomy with adnexectomy. In well or moderately differentiated type I carcinomas without extensive myometrial infiltration and with unremarkable retroperitoneal lymph nodes on imaging, this surgical therapy is usually sufficient. In addition, intravaginal radiotherapy should be evaluated postoperatively.
In G3 endometrioid carcinomas and all type II carcinomas, in addition to hysterectomy, pelvic and para-aortic lymphonodectomy is indicated, as well as tumor debulking in analogy to ovarian carcinoma in case of peritoneal involvement, according to the current guidelines. In addition, chemotherapy (carboplatin and paclitaxel) and, if necessary, percutaneous radiotherapy of the pelvis are recommended in most cases during follow-up. The value of systematic retroperitoneal lymphonodectomy is controversial and several studies are currently underway. Especially in combination with subsequent radiotherapy, lymphedema of the legs may occur in up to 40% of patients. Currently, we are evaluating whether sentinel lymphonodectomy may have a place in the treatment algorithm for endometrial cancer.
On the one hand, follow-up is symptom-oriented, but on the other hand, it is also important to find the central recurrence at the vaginal stump as early as possible, since this can still be treated under curative aspects. For this reason, six-monthly cytologic smears from the colpotomy are performed, as well as a transvaginal ultrasound at each checkup. Control intervals are scheduled every three to four months for the first three years after therapy, and every six months thereafter. Annual check-ups can be performed from five years after therapy. Routine imaging such as computed tomography or MRI and laboratory tests are not recommended and should be performed when specific symptoms are present [5].
The ovarian carcinoma [6–8]
A distinction is made between early ovarian cancer, which is limited to the adnexa and uterus (up to FIGO stage IIA), and advanced ovarian cancer, which spreads peritoneally and often involves extensive involvement of the Douglas, omentum, and upper abdominal organs, including the abdomen. Diaphragm domes and liver capsule shows. 10% of all ovarian cancers are genetic, mainly due to a BRCA mutation (“hereditary breast-ovarian cancer syndrome”). The lifetime risk of developing ovarian cancer with a confirmed gene mutation is up to 60%.
In ovarian cancer, there is also no evidence to date for effective screening, particularly in women with known BRCA mutations.
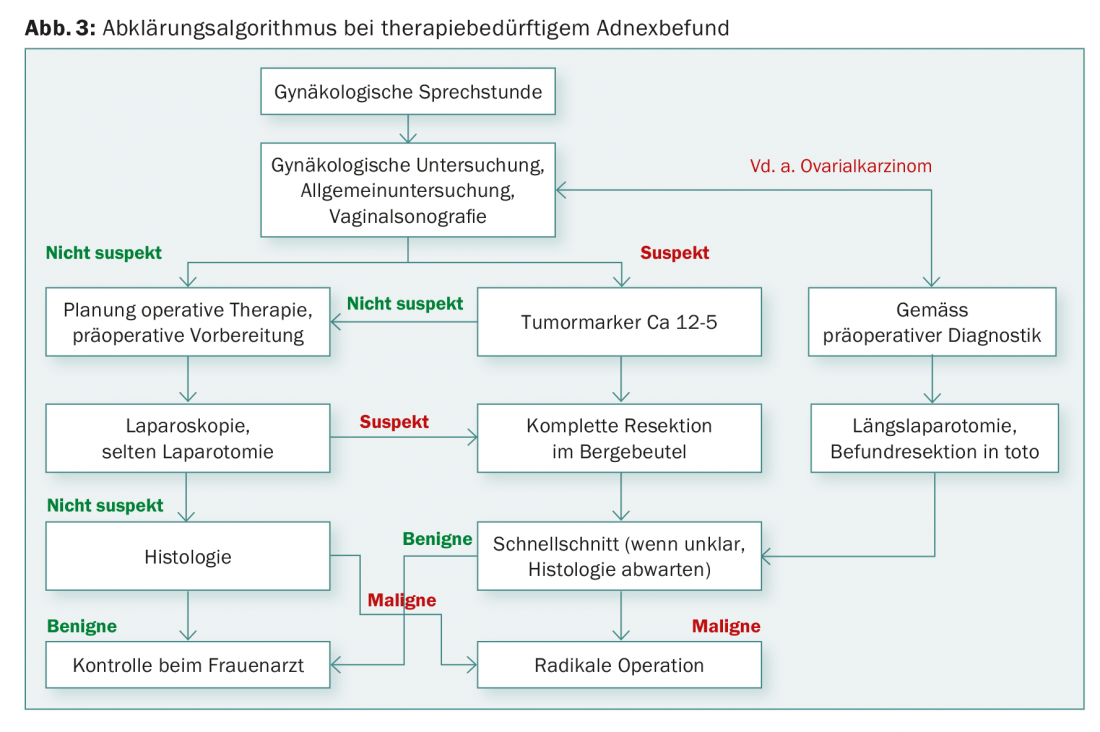
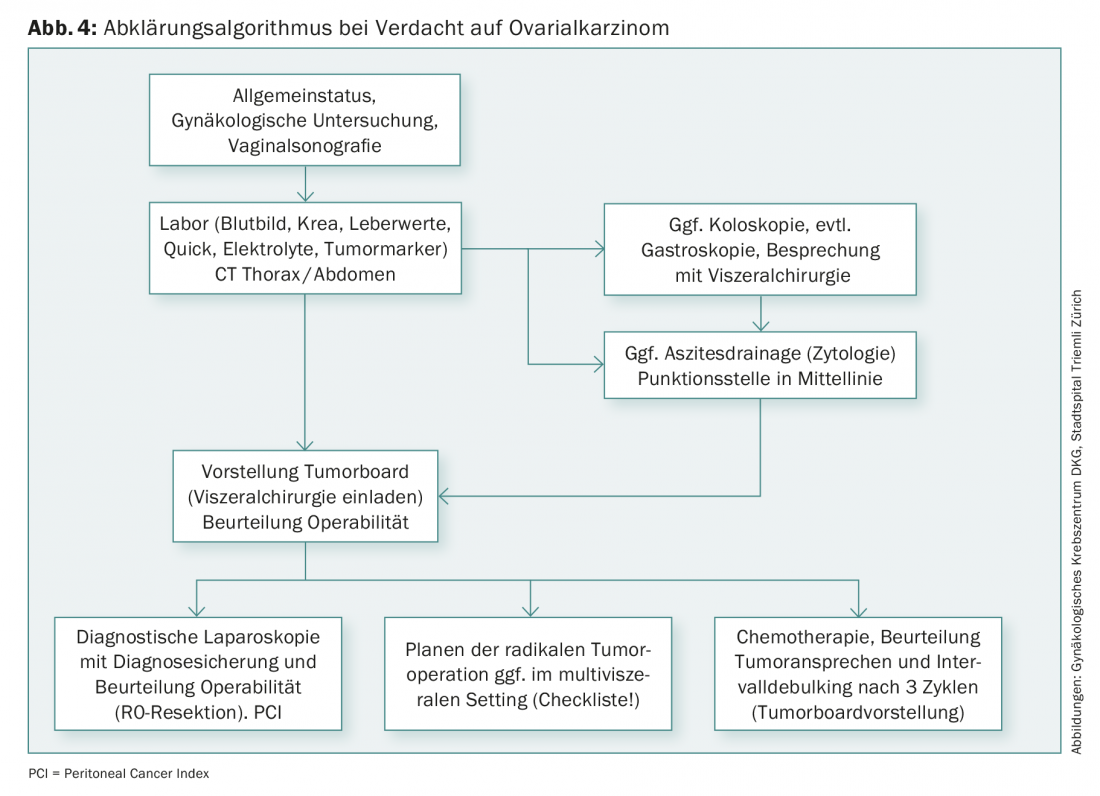
Early ovarian cancer is often an incidental finding in the sense of an unclear adnexal finding with absent or nonspecific symptoms. Advanced ovarian cancer usually presents with nonspecific symptoms due to peritoneal carcinomatosis – bloating, increase in abdominal girth, malaise, diffuse abdominal discomfort, etc. (Figs. 3 and 4).
Therapy for ovarian cancer consists of surgery followed by chemotherapy (usually six cycles of Carboplatin/Taxol®). Surgically, hysterectomy is performed with bilateral adnexectomy, omentectomy, peritoneal biopsies, and pelvic and paraaortic lymphonodectomy, and in certain cases appendectomy. In the case of peritoneal involvement, complete removal of all tumor-involved areas, if possible, is associated with a better prognosis than incomplete tumor surgery. This means that multivisceral resection with, for example, rectosigmoid resection, further partial bowel resections, diaphragm mastripping, liver capsule resection, and/or splenectomy must often be performed if the general condition is appropriate. Accordingly, the surgical setting must be planned in an interdisciplinary manner with adequate anesthesiological and intensive care requirements. If, on the basis of the clarifications, the diagnosis remains unclear or surgical complete removal is only questionably possible, a diagnostic laparoscopy is primarily performed or, if necessary, chemotherapy is started directly. If response is good, surgical therapy can be performed as interval debulking after three cycles of chemotherapy. If complete resection could not be achieved in stage FIGO III, chemotherapy is combined with bevacizumab followed by maintenance therapy.
Follow-up of ovarian cancer is mainly symptom-based with the same follow-up intervals as for endometrial cancer. At each check-up, in addition to the gynecological examination, a transvaginal sonography is performed and once a year a cytological smear is taken from the colpotomy. Computed tomography and tumor markers should be performed only when symptoms are present and recurrence is suspected, because early detection of asymptomatic recurrence results in poorer quality of life with advancement to the palliative phase and adverse effects of therapy with no impact on overall survival.
The cervical carcinoma [9,10]
Virtually all cervical cancers are HPV-associated (Fig. 5), with HPV types 16 and 18 responsible for 70-80% of all cervical cancers. These two types have been covered by HPV vaccination under the national vaccination program since 2008. Screening regarding precancerous lesions of the cervix is performed with annual cytologic cervical smears (PAP smears) and is first recommended at age 21. If the last three smears were unremarkable and there are no other risk factors, the intervals can be extended to every two or three years. In addition, HPV screening is currently being discussed instead of cytologic examination [11].
Histological diagnosis of cervical carcinoma is followed by clinical and imaging evaluation of tumor stage. Early cervical carcinoma up to FIGO stage Ib1 (tumor size <4 cm) is usually treated surgically by extended hysterectomy and pelvic and deep paraaortic lymphonodectomy; more advanced stages are treated by primary combined radio-chemotherapy. The value of sentinel lymphonodectomy is also currently being evaluated in cervical cancer.
During follow-up, it is important to detect central recurrence or pelvic wall recurrence early. Therefore, a cytologic smear of the colpotomy, transvaginal sonography, and sonography of the renal pelvic system should be performed at all checkups.
Take-Home Messages
- There is no established and effective screening for endometrial and ovarian cancer.
- Virtually all cervical cancers are HPV-associated. For cervical cancer, cytologic cervical smears (PAP smears) are an effective screening tool. In the future, this will probably be done by HPV screening.
- Any woman with postmenopausal bleeding or atypical bleeding in the premenopausal period must undergo gynecologic and transvaginal
- sonography and, if necessary, clarified by means of hysteroscopy and curettage.
- Surgical therapy of advanced ovarian cancer requires a well-coordinated interdisciplinary team. The careful
- pre-therapeutic planning and interdisciplinary discussion of the therapeutic concept are crucial for the outcome.
Literature:
- Swiss Federal Statistical Office (SFSO), National Institute of Cancer Epidemiology and Registration (NICER): Cancer in Switzerland, Status and Development from 1983 to 2007.
- Emons G, et al: Consultation version. Guideline report. S3 guideline diagnosis, therapy and follow-up of patients with endometrial cancer. AWMF registry number 032/034OL. 2017.
- Colombo N, et al: Endometrial cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2013; 24(Suppl 6): vi33-8.
- NCCN Guidelines: Uterine Neoplasms. 2017.
- Gynecologic Oncology Working Group of the SGGG: Recommendations gynecologic oncology follow-up. 2009.
- DGGG: S3-Leitlinie Diagnostik, Therapie und Nachsorge maligner Ovarialtumoren. AWMF register number 032/035OL. 2017.
- Ledermann JA, et al: Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2013; 24(Suppl 6): vi24-32.
- NCCN Guidelines: Ovarian Cancer. 2017.
- DGGG, AGO: S3-Leitlinie Diagnostik, Therapie und Nachsorge der Patientin mit Zervixkarzinom. AWMF register number 032/033OL. 2014.
- NCCN Guidelines: Cervical Cancer. 2017.
- Gerber S, et al: Update of screening for cervical cancer and follow-up by colposcopy. Expert letter SGGG No 40. 2012.
InFo ONCOLOGY & HEMATOLOGY 2018; 6(1): 6-10.









