It is difficult to imagine a sport where the foot does not play a central role. No part of the body is used for such a wide variety of tasks as the human foot. In sporting use, it is a shock absorber, a means of locomotion, a rudimentary gripping organ and a tool for working the sporting object (sometimes even the opponent). Perhaps like no other part of the body, the human foot, especially that of an athlete, is subject to considerable forces.
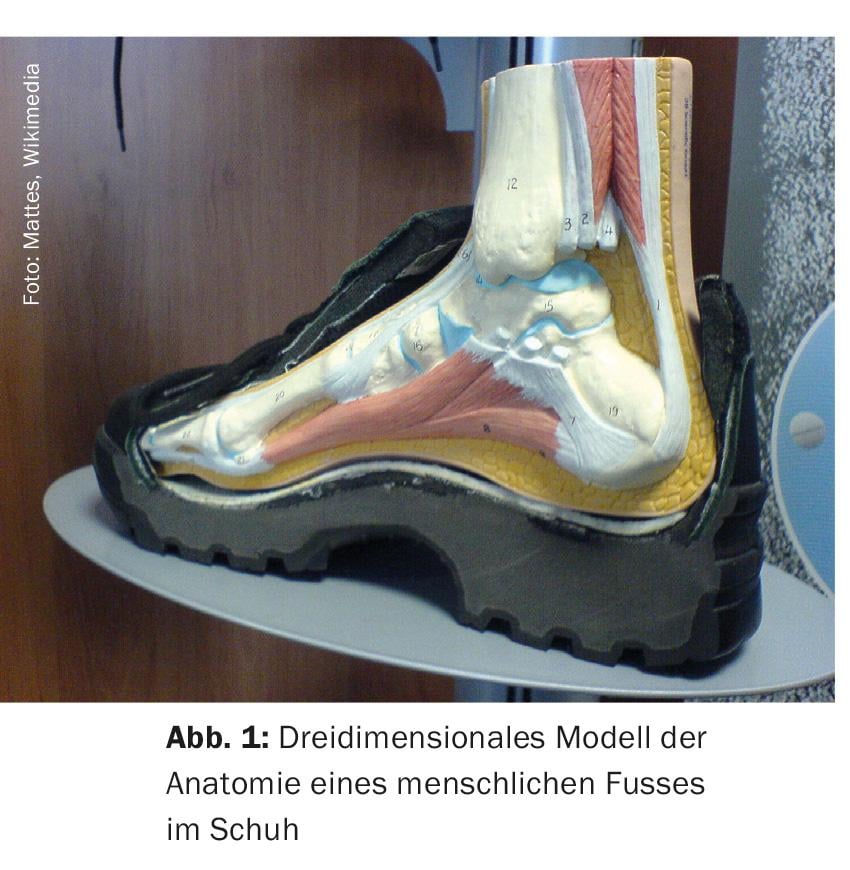
The human foot is an ingenious but correspondingly complex construct (Fig. 1). Both adult feet contain about a quarter of the bones of the human body, i.e. 26 per foot. These bones form 16 joints, which are held together by more than 100 ligaments and actuated by 20 muscles. These partly dynamic structures give the foot its stability, strength and thus also its extraordinary functionality. Depending on the running speed, the forces involved can be up to five times the body weight.
The shape of the foot, with longitudinal and transverse arches, distributes the body weight to the three points of the heel, metatarsophalangeal joint and metatarsophalangeal joint of the small toe, and therefore plays a central role in the function of the foot. The fat pad on the bottom of the foot is thickest at these three points. The many receptors in the sole of the foot are another indication of how important our feet are.
Foot types
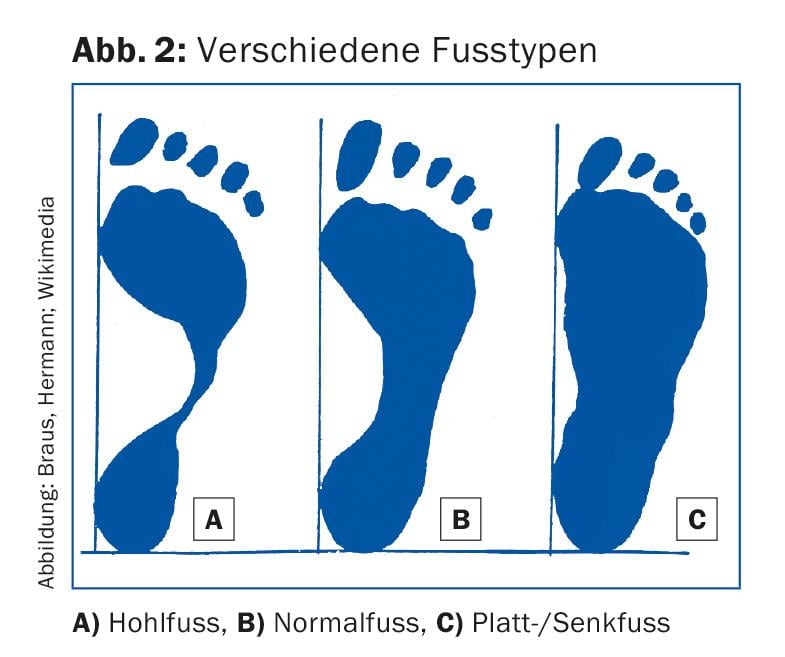
Classically, three types of feet are distinguished. The classification is based on the height of the longitudinal arch (Fig. 2):
- Normal foot: Usually has no particular biomechanical problems.
- Flat/Countersunk Foot: Here there is a lowering of the longitudinal arch. The foot is basically rather unstable. The flat/descent foot owner needs good control of motion and pronation, as well as optimal stabilization ability.
- Hollow foot: Hollow foot often presents various problems. Particularly problematic is its relative stiffness, which reduces its damping properties.
It must be pointed out at this point that the three types are basically variations of form, which by no means necessarily have pathological value.
What happens when you run?
Running is the most natural use of the feet. From a biomechanical point of view, running is a repetitive motion process. On average, 400-600 steps are taken per kilometer run. Every time the foot makes contact with the ground, forces occur that are referred to as vertical ground reaction forces. At a speed of 10 km/h, the ground contact is between 200 and 250 m/s (20-25% of a second).
The ground contact of the foot is divided into three phases: Landing phase or impact, stance phase and push-off phase.
The landing phase lasts from the first contact of the heel (or forefoot) with the ground until the moment when the entire foot is on the ground. In terms of time, the landing phase for the runner corresponds to 8-10% of the total ground contact.
The stance phase includes the time when the whole foot surface is on the ground. The stance phase corresponds to 40% of the stride for the runner. It is divided into:
- The weight transfer from the first contact to the lifting of the other leg
- The middle stance phase from standing on the whole foot to lifting the heel
- The final phase, when the other leg touches the floor.
The push-off phase begins when the heel lifts off the ground, and it lasts until the end of contact with the ground. The push-off phase corresponds to 50% of the stride for the runner. It is divided into:
- Lifting off the big toe
- Start of swing when the swing leg passes the stance leg
- Middle swing part (“mid swing”), until the lower leg is vertically above the floor
- The final swing, which lasts until the heel touches down.
This completes one gait cycle.
What forces are at work?
The highest force values are to be measured in the landing phase. The ground reaction forces (passive forces or impact forces) reach peak values of two to three times the body weight (KG). The loading time is very short.
In the repulsion phase, on the other hand, active or propulsive forces are generated with high peak values but long loading times. For an optimal rolling motion, only the passive impact forces may be reduced or damped. Reduction or attenuation of active/propulsive forces results in a loss of strength that must be compensated for by an increase in muscle activity.
Investigation modalities
While foot shape can be assessed reasonably easily “clinically” or with a podoscope (mirror table), it takes much more to analyze gait. Using sensitive measurement techniques, a run and gait analysis, details of the motion sequence can be brought to light that cannot be perceived with the naked eye. Such a special examination usually includes:
- A static assessment of the feet, knee, hip and spine axes is performed on the mirror table. Here, a qualitative assessment of posture is performed.
- A pressure distribution measurement using the Footscan analysis system: The test subject stands on a pressure measurement plate. The connected computer can be used to display, store and evaluate the load on the foot (static measurement to assess the shape or type of foot, dynamic measurement to assess the development of pressure during the ground contact phase of a running stride). For the dynamic measurement, the test person runs at a relaxed walking pace over a track in which the pressure measurement plate is integrated. This measurement technique enables a quantitative analysis of the load during the ground contact phase of a running stride.
- Video analysis on the treadmill to assess rolling is another assessment method. The test person runs on the treadmill in a relaxed continuous run. After a run-in phase, the runner is filmed from both the front and the back. Due to the high resolution of the film center section, it is possible to view the individual phases (heel strike, stance phase and push-off phase) in a very differentiated manner. In the single step, the stance and swing phases are distinguished (including even further subdivisions of these moments). Subsequently, the examiner explains the individual sequences to the test person on the basis of the video, points out any malpositions and their consequences, and discusses any necessary (possible) measures. The referring physician is informed by report. It is not uncommon for a custom orthotic to be made after this examination as a measure to correct the detected malpositions.
It goes without saying that an examination as complex, time-consuming, expensive and usually not covered by health insurance as video analysis is not the first step in the assessment of foot complaints – especially not in the case of overuse disorders, which are among the most common complaints. A conventional, simple gait examination in the practice room, a standing one- and two-legged examination, and a conventional “manual” examination of the various parts of the foot are indispensable before further technology is used.
HAUSARZT PRAXIS 2016; 11(6): 4-6