Case description: We report a 31-year-old patient who was medically evaluated for new-onset neck pain on exertion without accompanying neurologic symptoms.
MRI imaging performed revealed an intraosseous mass in the craniocervical junction (Fig. 1), which most closely resembled a chordoma in terms of image morphology. A transoral biopsy was performed to confirm the diagnosis, which confirmed the suspicion of chordoma [1].

MRI and CT diagnostics: T2-weighted sequences showed a hyperintense mass in the clivus with extension over the os occipitale at the foramen magnum and over the occipital condyles as well as over the atlas into the dens and corpus of the axis (Fig. 2 and 3). The mass extended ventrally at the level of the foramen magnum to the right extracranial internal carotid artery and had broad contact with the jugular foramen and the right jugular vein. The vertebral artery was walled by the mass at the level of HWK 2 on both sides, more so on the left than on the right. The mass showed vigorous, somewhat inhomogeneous contrast enhancement. On supplemental CT scan, the mass appeared as extensive osteolysis without calcifications.


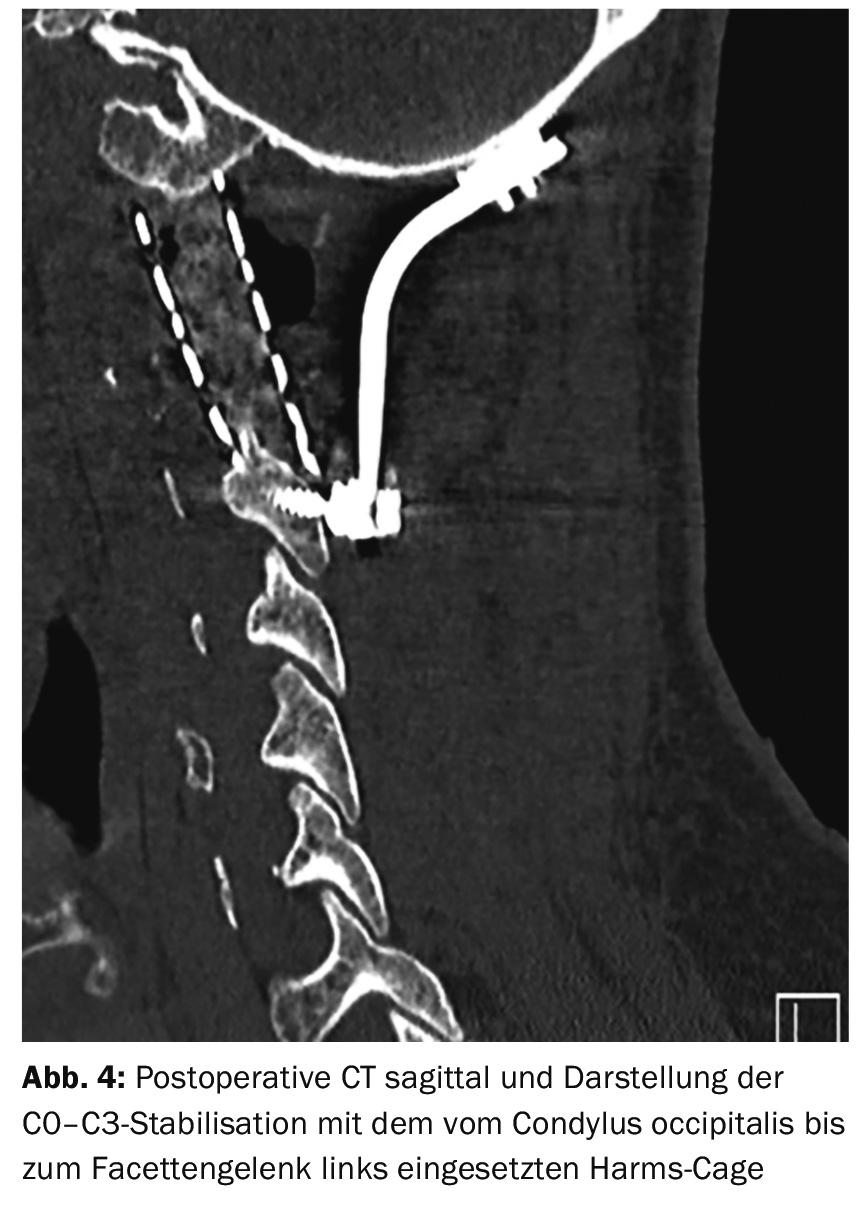
Course: Extensive infiltration and osteolysis of bony structures at the craniocervical junction necessitated dorsal stabilization prior to planned tumor resection. In a first step, orthopedic surgeons performed an occipitocervical fusion using a dorsal plate-screw system (Fig. 4). In the same operation, parts of the chordoma around the vertebral artery could be resected on both sides.
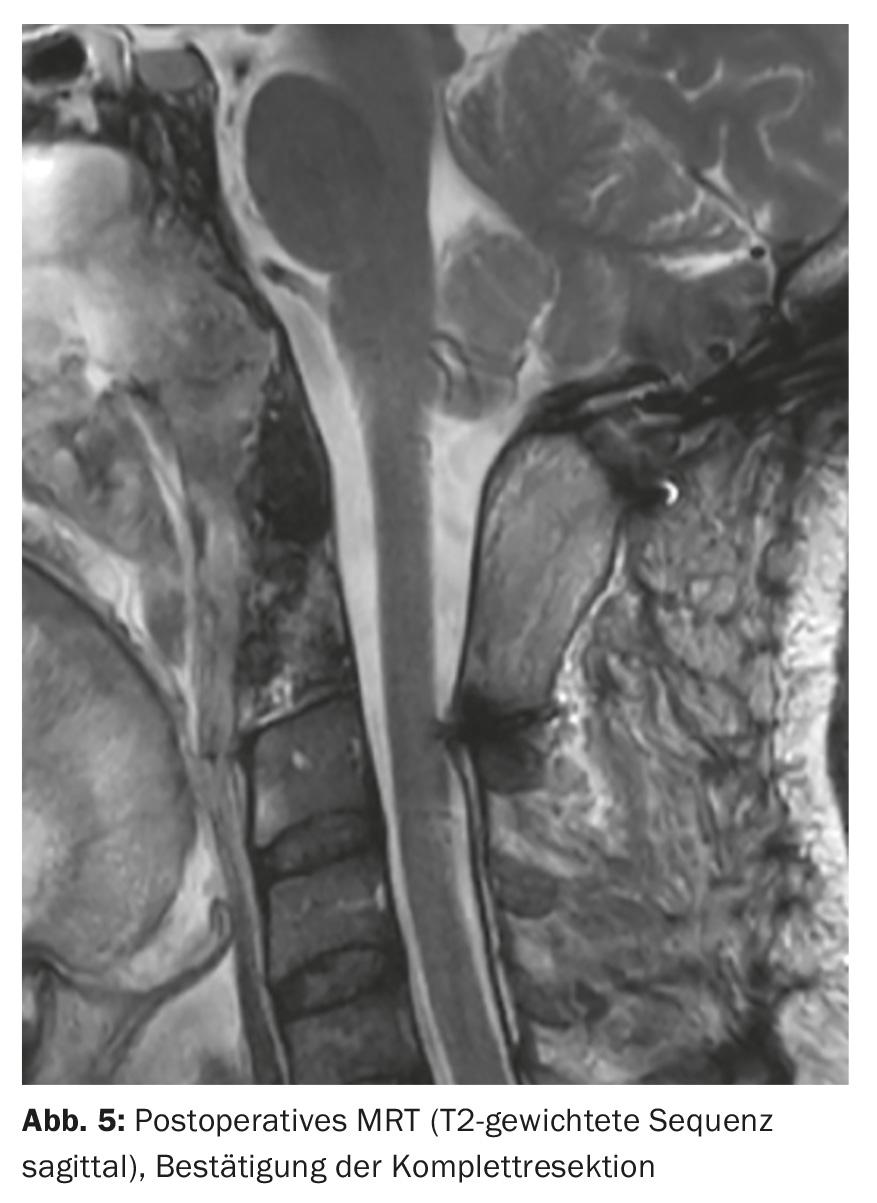
Nine days later, combined transnasal-transoral complete resection of the chordoma was performed with endoscopic-assisted technique by the colleagues of ORL and neurosurgery. A complete resection of the chordoma could be achieved with this procedure. In the postoperative MRI controls, the complete resection was confirmed (Fig. 5). The clinical postoperative course was free of complications. The patient was discharged home symptom-free after a good month and a half of hospitalization and adjuvant radiotherapy was planned. MRI follow-up at six months showed no recurrence.
Conclusion: The close interdisciplinary collaboration between neuroradiology, orthopedics, ORL and neurosurgery allowed to achieve the goal of a complete resection of this complex chordoma at the craniocervical junction.
Literature:
- Choi D, et al: Outcome of 132 operations in 97 patients with chordomas of the craniocervical junction and upper cervical spine. Neurosurgery 2010; 66(1): 59-65.
InFo NEUROLOGY & PSYCHIATRY 2016; 14(3): 36-37.