
Instrumental 3D gait analysis allows simultaneous measurement of kinematics, kinetics and electromyography (EMG), providing additional information to conventional diagnostic methods. This allows complex (neuro-)orthopedic and neurological disease patterns to be analyzed. The advantage is on the one hand the quantitative recording of the movement behavior of patients, on the other hand it is a non-invasive, radiation-free method. The different analysis methods complement each other and can only be interpreted meaningfully in combination.
Children and adolescents with abnormalities in posture and/or movement often present to pediatricians and family physicians. Musculoskeletal pathologies or neurological diseases can lead to gait disorders. In addition to the clinical examination, the physician has imaging methods at his disposal, such as conventional X-rays and computer tomography (CT). Here, the differentiation of diverse physiological developmental variants from pathological processes in children and adolescents is often difficult.
Quantitative representation through 3D analysis
In specialized hospitals, instrumental 3D gait analysis enables the interdisciplinary team of physicians, sports and exercise scientists, and physical therapists to confirm diagnoses for clinically relevant issues. On the one hand, methods for complex analysis of the human gait pattern are available in medicine (Tab. 1) . Supplementary information can lead to the review of initiated care/therapy measures and, if necessary, to the improvement of surgical planning. On the other side of the methods is descriptive gait analysis by the naked eye. It serves as a basic technique for detecting gait deviations through trained visual observation. The human eye can directly process about ten pieces of information per second. In contrast, infrared cameras, such as those used for 3D gait analysis, record data at a frequency of 200 Hz (frames/sec). In between is the apparatus-supported medical gait diagnostics, which uses simple video evaluation procedures and dynamic pressure load measurements.

Comparisons of walking patterns facilitate correct diagnosis
In a 3D gait analysis, the simultaneous measurement of kinematics (joint angle), kinetics (joint forces, torques, ground reaction forces) and EMG (muscle activity) provides us with information about possible asymmetries or deviations of the pelvis, ankle, knee and hip joints. Under dynamic conditions, occurring loads on the joints can be calculated. Complex gait disorders can thus be represented quantitatively, e.g. in the form of angle-time (kinematics) or force-time (kinetics) curves. In the anatomical planes sagittal plane (flexion/extension), frontal plane (abduction/adduction, varus/valgus) and transverse plane (external/internal rotation) movements between the segments can be recorded.
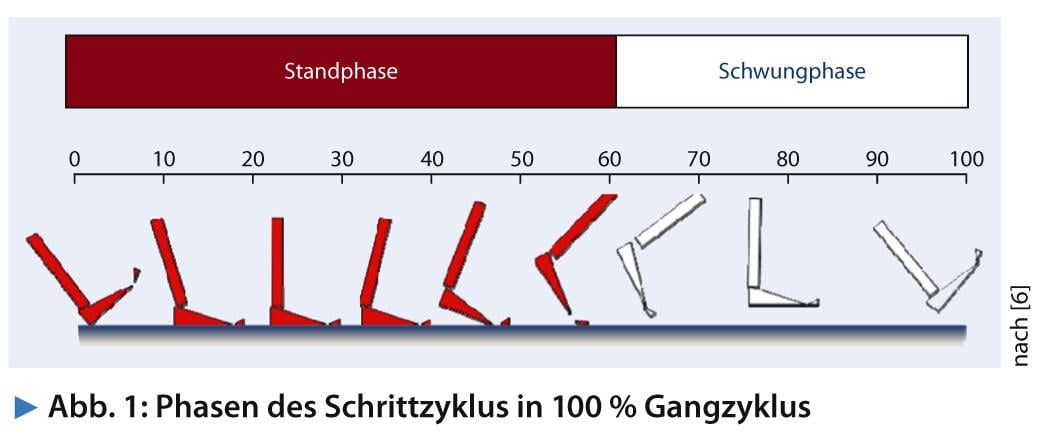
The basis for the evaluation is a normalized double step, defined as two consecutive initial ground contacts of the same foot. A gait cycle consists of approx. 60% stance and 40% swing phase (Fig. 1) . The comparison with healthy test subjects is just as suitable in practice as the relative reference in the sense of a pre- and postoperative comparison. Standard values are used to describe the physiological gait pattern. Knowledge of this enables the physician or therapist to make a correct diagnosis, develop an individual therapy, and evaluate a treatment based on data. Irrespective of this, standard values are used as orientation values.
Prerequisite for a physiological gait:
- Intact central and peripheral control
- Sufficient joint mobility
- Sufficient muscle strength
- Stable lever arms via stabilizing joints
- Intact energy supply
Advantages and disadvantages of different measurement methods
Kinematic data (angle-time curve) are recorded using high-resolution multi-camera systems. Using double-sided adhesive tape, markers are applied to anatomically defined, bony points. The infrared cameras emit light pulses that are reflected by the markers. The captured reflected pulses are transmitted from the cameras to the computer, which calculates the spatial coordinates from at least two camera views and reconstructs a line figure using connecting lines between each marker. Anatomical landmarks are used to determine segmental movements (e.g., between the upper and lower leg) relative to each other. Depending on the question, the markers are arranged using differently defined marker sets. These marker models differ in number of markers, positioning, application possibilities as well as output parameters. A disadvantage and limiting factor for the validity of the measurement data are artifacts due to skin displacement and soft tissue.
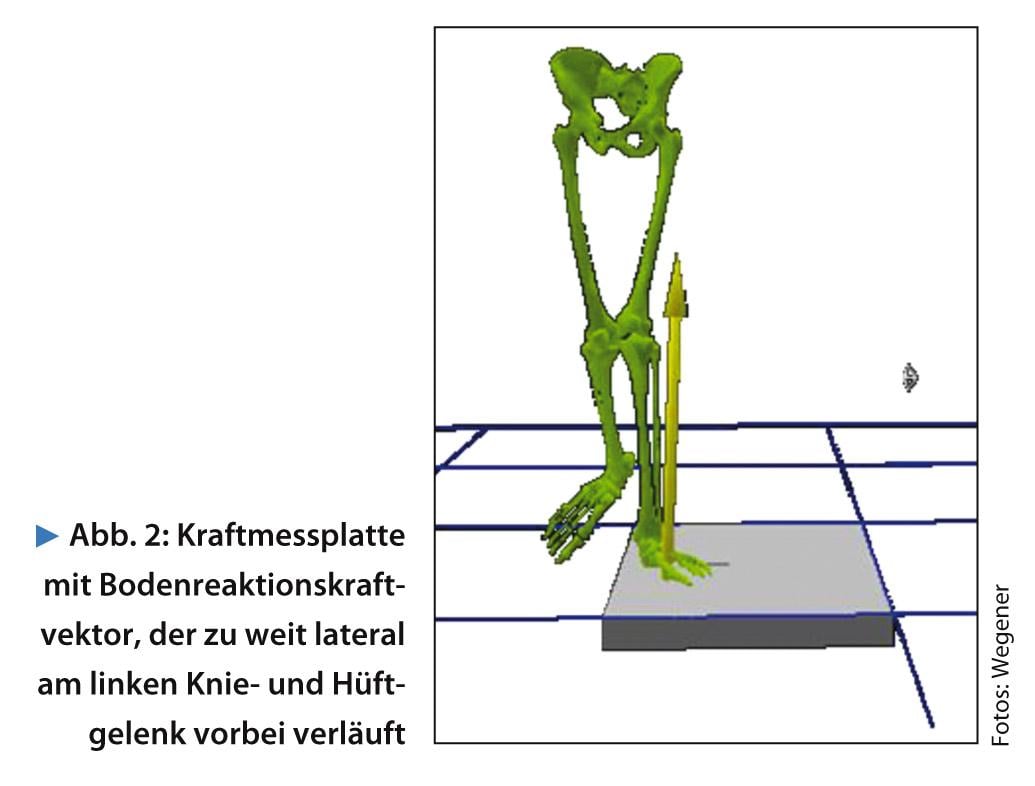
Kinetics (force-time progression) deals with the forces acting on a joint or body part. The interest is the cause and control of the movement. Vertical and horizontal ground reaction forces are measured by force plates embedded in the ground (Fig. 2). These measurements allow the calculation of the functional demands (loads) on the joints that occur during walking. Torques are calculated for the lower extremity joints using inverse dynamics mathematics. The aim of this method is to determine the torques and forces required for a kinematic movement.
Surface EMG measurements are performed to assess muscle activity. Electromyography is a method for determining the electrical potentials during muscle contraction at the musculature. The innervation behavior of the derived muscles can thus be objectively displayed. Surface electrodes are used to acquire the EMG signal. The use of EMG in clinical gait analysis reveals, among other things, when which muscle groups are active in the different phases of the gait cycle.
Kinematic, kinetic, electromyographic, and clinical methods complement each other and can only be meaningfully interpreted when combined. Mobility and muscle function tests are used to determine the patient’s movement status so that the results of the gait analysis can be interpreted. In patients with neurological disease, the muscles are additionally tested for spasticity.
Application example
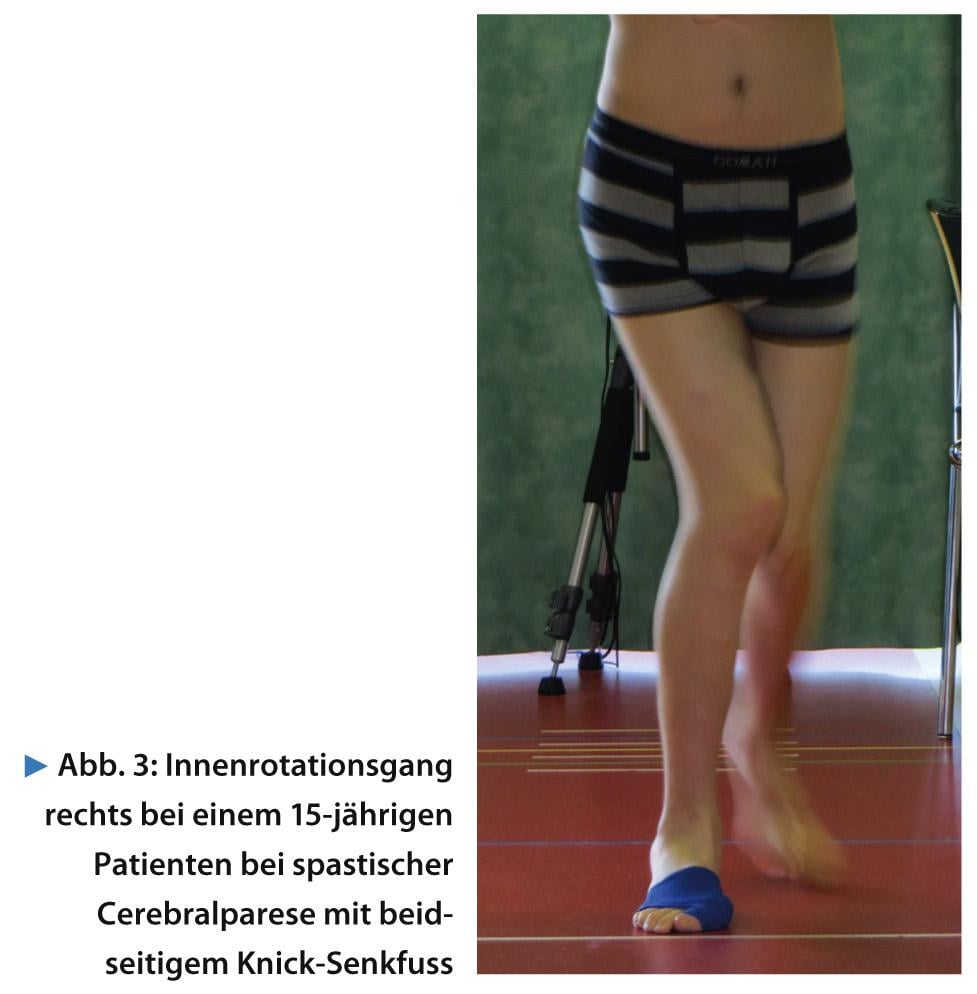
One of the most common gait disorders in cerebral palsy is the internally rotated gait pattern seen in the present patient (15 years) with right-sided spastic cerebral palsy (Fig. 3) .
However, the increased internal rotation of the right hip joint with simultaneous adduction contracture during walking does not lead to an inward gait but to an outward gait on both sides (foot progression angle) due to the increased tibial excursion of 51° on both sides (norm 33° ±8°) as well as the bilateral buckling feet. The cause of the increased right hip internal rotation is an increased internal rotation of the hip clinically measured at 90° flexed hip joint with abolished external rotation ability (right IRO/ARO 55/0/0°). In contrast, the left hip rotation angle is within the reference range during walking (Fig. 4). Differential diagnosis of coxa antetorta could be excluded.
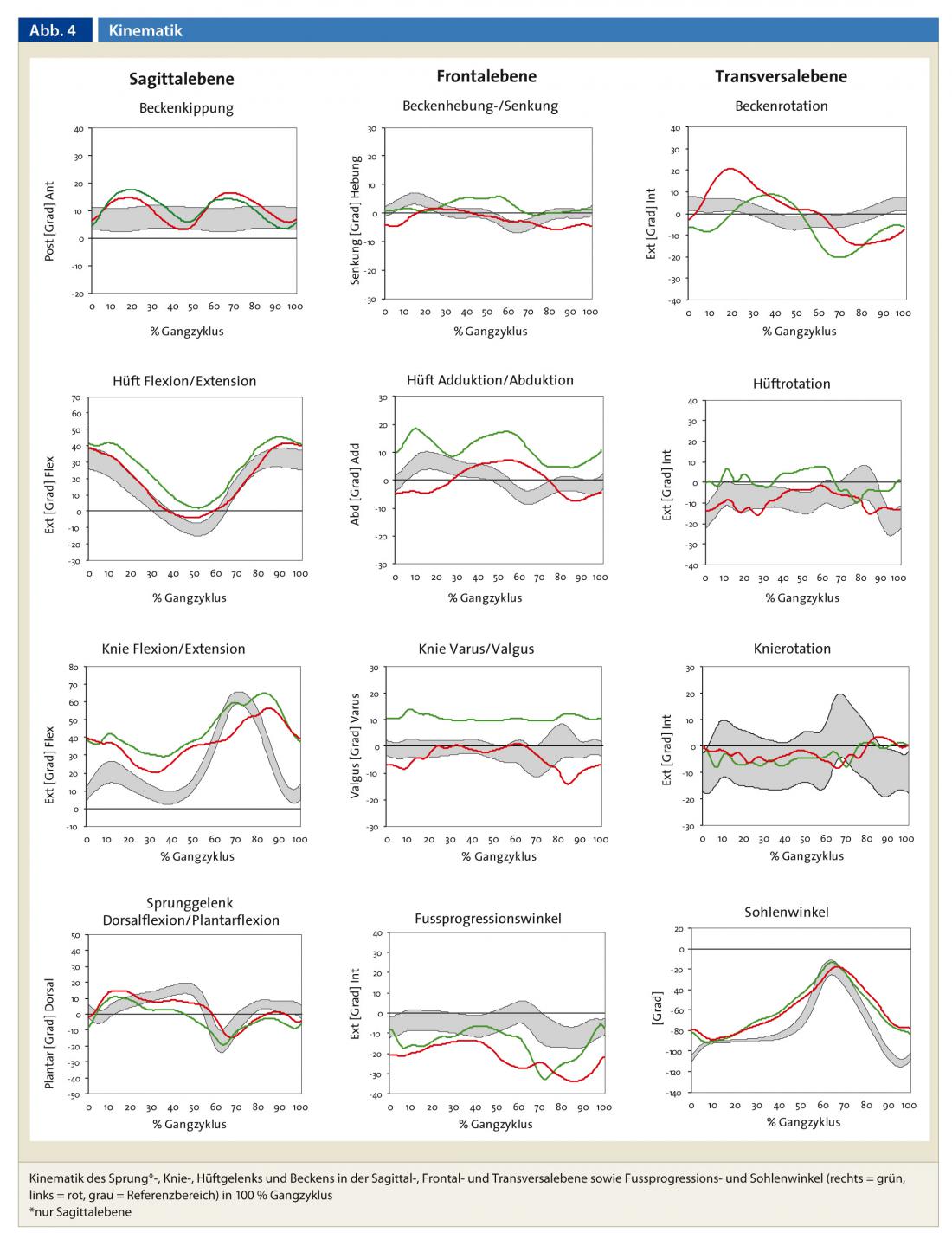
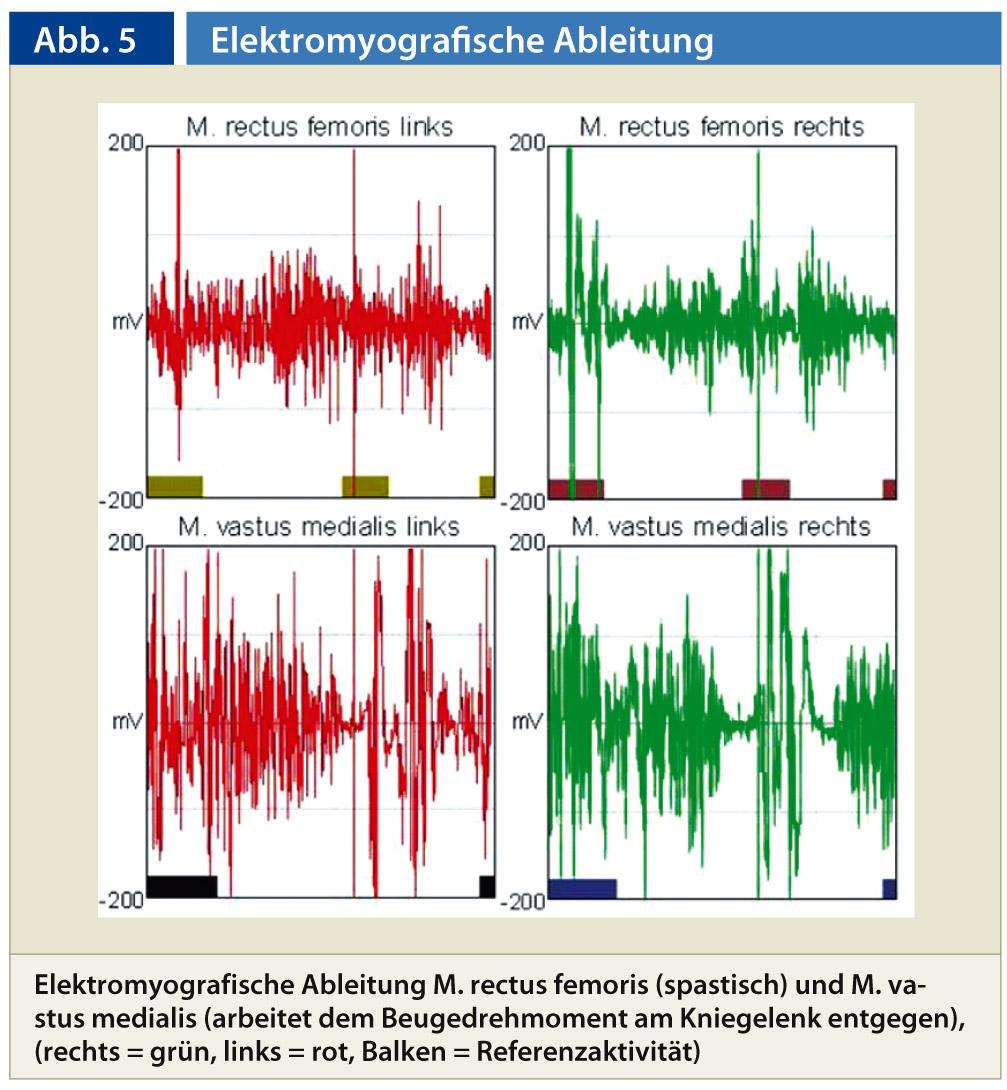
The double-peaked course of the sagittal pelvic motion and the clinical examination indicate that the iliopsoas muscle shows severe shortening bilaterally (Fig. 4). The spasticity test reveals that the hip flexors are spastic bilaterally. The shortening resulting from the spasticity in turn leads to the patient having to walk with bent knee joints in order to maintain balance. Both knee and hip joints are excessively flexed during the gait cycle, with flexion already contracted on both sides. The knee extensors must counteract the resulting flexion torques at both knee joints, which is indicated by a continuous stance phase activity in the dynamic EMG of the vastus medialis muscle. (Fig. 5).
In addition, the right hip joint is increasingly adducted due to contracture, with high forces (abduction torques) acting on both hip joints until the end of the stance phase with weak hip abductors (Fig. 6).
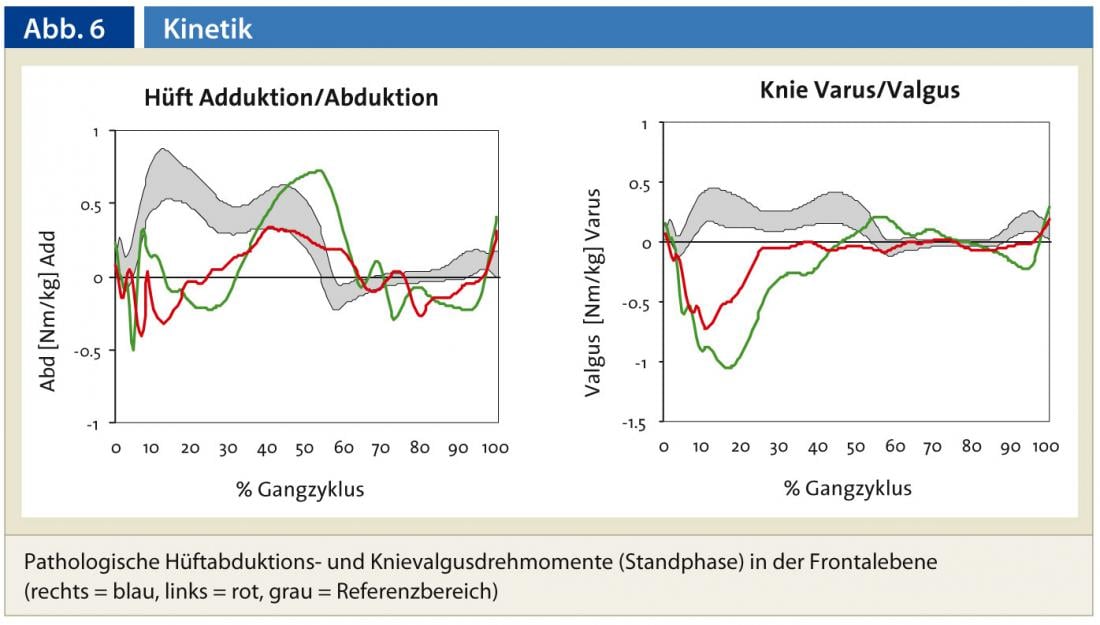
While the left knee angle in the frontal plane is almost in the normal range, the right leg shows a valgus knee angle in the stance phase. This valgus angle results from a combined internal rotation of the right hip joint and the knee flexion contracture (Fig. 4). In this case, loads (valgus torques) on the right > left are increased many times over at both knee joints, which can lead to premature misuse in the knee joints (Fig. 6, Fig. 2) . The valgus load in the left knee joint results from the increased external foot rotation (toeing-out) on the left as well as the lateral tilt of the upper body to the left side as a consequence of weak gluteal muscles, whereby the force vector is directed so far outward by foot position and lateral tilt of the upper body that high lateral (valgus and abduction) moments are triggered at the joints in both the left knee and hip joints.
The planned multilevel procedure includes torsion correction of both thighs, bilateral knee extension, and surgery of both feet. Thus, it is possible to differentiate even a complex and multifactorial gait pattern with the instrumented 3D gait analysis and thereby enable a targeted treatment and therapy.
Conclusion for practice
- 3D instrumental gait analysis provides essential additional information that cannot be captured by clinical means to assess walking ability.
- Complex orthopedic or neurological disease patterns can be analyzed (actual condition), diagnostic confirmation can be completed and therapy progress can be documented.
- The movement behavior of patients can be recorded quantitatively.
- It is a non-invasive, radiation-free measurement method.
- Under dynamic conditions, the examination provides information about the extent of movement (kinematics), acting torques and forces (kinetics) and muscle activity (EMG).
- Side differences between affected and unaffected sides can be displayed via a symmetry comparison.
- Comparison data sets of a healthy control group simplify the interpretation of conspicuous movement patterns.
Dr. phil. Regina Wegener
Literature:
- Bachmann C, et al: Measurement systems, measurement methods and examples for instrumented gait analysis. Schweiz Z Med Traumatol 2008; 56 (2): 29-34.
- Döderlein L, Wolf S: The value of instrumental gait analysis in infantile cerebral palsy. Orthopaedic 2004; 33 (10): 1103-1118.
- Kirtley C, 2004: Clinical gait analysis – theory and practice. Elsevier, Churchill Livingstone.
- Kleissen RFM, et al: Electromyography in the biomechanical analysis of human movement and its clinical application. Gait Posture 1998; 8: 143-158.
- Ludwig O, 2012: Gait analysis in practice. Application in prevention, therapy and care. C. Maurer: Geislingen.
- Sander K, et al: Instrumental gait and motion analysis in musculoskeletal disorders. Orthopaed 2012; 41 (10): 802-819.
- Waidelich HA, et al: Computed tomographic torsion-angle and length measurement of the lower extremity. The methods, normal values and radiation load. Rofo 1992; 157 (3): 245-251.
HAUSARZT PRAXIS 2013; 8(6): 14-18









