
“Three times a capsule of pill XY in the morning, at noon, and in the evening, each time at mealtime,” is a relatively classic prescription for any practicing physician. Or, “I prescribe nine sessions of physical therapy, twice a week, with follow-up at the end of those sessions.” And another example, “I am declaring you 50% fit for work again, effective immediately.” But what about prescribing physical activity in general? Here, today’s medicine has a lot of catching up to do, although very good results can be achieved, as this article shows.
The statement that physical activity has a proven incomparable breadth of health-promoting effects as no single current drug, and this even without significant side effects and very inexpensive (see HAUSARZT PRAXIS 3/2014), hardly causes controversy today. It cannot be emphasized enough how therapeutically effective sensible adapted physical activity can be – or “could” be, because in our present medicine far too little is made of this excellent possibility!
Complicated prescription
“Three times a tablet in the morning, at noon in the evening at dinner” is thus a habitual prescription that must nevertheless be based on hard data. Age, height, weight, gender are taken into account, depending on which not all patients with the same pathology get the same amount and dose. However, the information is very clear, countless references allow to do the right thing in specific situations.
Prescribing physical activity is a lot more complicated. It is true that age, height, weight, gender are also important parameters to consider. Much more important and much more difficult to grasp, however, is the patient’s initial physical condition: How well is he already trained? What kind of “work” will it endure? What do you have to take into consideration? Only knowing this can tell how he needs to continue training to get his health even more under control.
There are good ways to do this, and we can only highly recommend that anyone who needs advice on physical activity get as accurate a baseline as possible. A sports medical examination, i.e. an examination from head to toe by a physician experienced in sports medicine, a specific blood analysis and an ECG are recommended . However, it is essential that this also includes a performance test, at least one that determines aerobic endurance capacity. It would also be optimal to still perform a strength determination of the main muscle groups, but this clearly becomes a bit more time-consuming. Such examination packages are routinely supplied by specialized institutions, they are the objective basis on which a good training program for maintaining and improving health can be built.
Aim of the stress
Another important variable that needs to be precisely defined is the goal of the stress: improving aerobic capacity, strength, or agility and coordination? Ideally, all the above-mentioned condition factors should be taken into account, with endurance clearly taking priority from a health point of view.
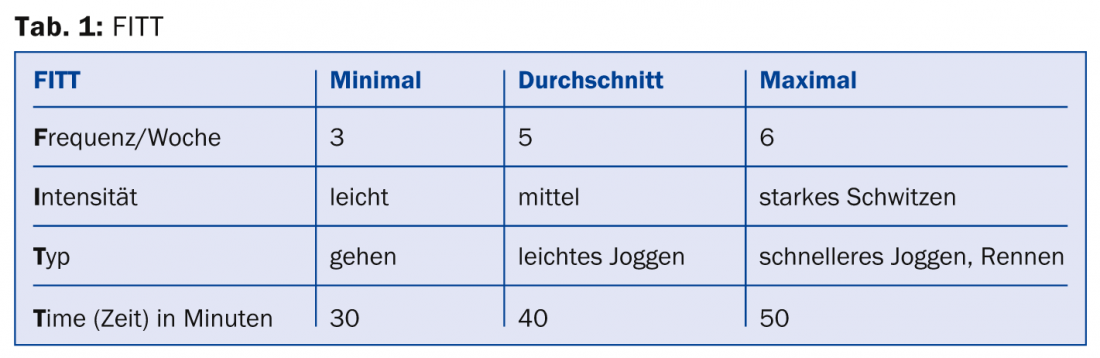
Then the frequency, intensity and duration of the training must be marked (Tab. 1).
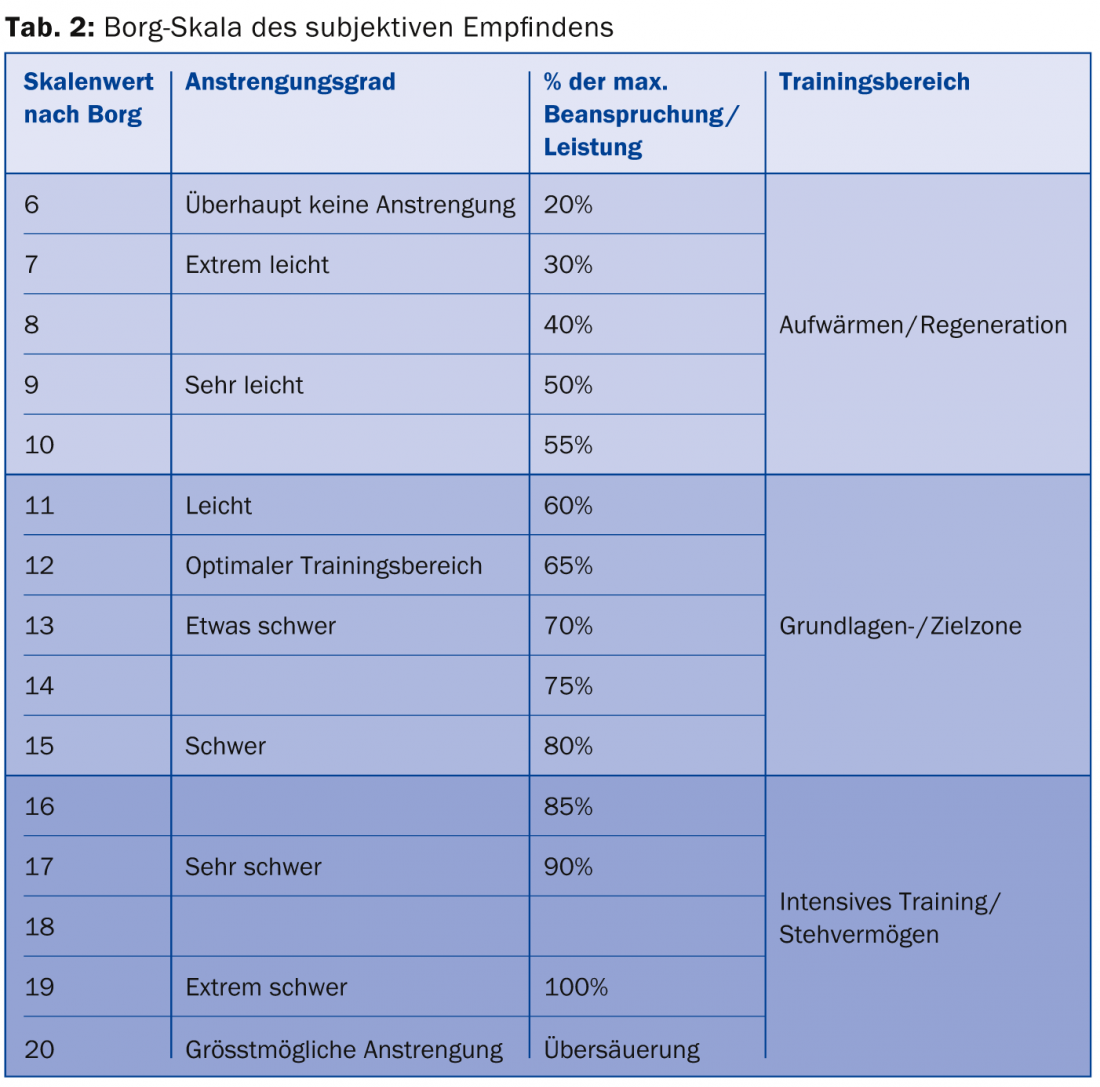
Activity intensity is often controlled by heart rate, and the correct number of heartbeats for the particular patient is best determined based on values obtained in the performance test. Personally, we advise against the countless “180 minus age” or “60% of 220 minus age” type formulas. The Borg scale (Table 2) is more imprecise, but can be used.
Integrate into pharmacological therapy
A very important point is to integrate this prescription of physical activities into the pharmacological therapy program, and to adjust it if necessary (insulin dose, beta blocker, etc.). Beta-blockers affect heart rate, which must be taken into account when managing exercise with heart rate.
Just as with the prescription of “classical” medical measures, it is essential to carefully monitor the effects and side effects of physical activity. At the start of treatment, these checks should take place at rather short notice (e.g. every 14 days). But as for the full development of the effect, more time is needed, four weeks at the minimum.
Technological gadgets to support?
In the age of electronic gadgets, we must definitely mention the countless wristbands and watches that register biological functions, as well as pedometers. Even if their effectiveness has not been definitively proven scientifically, they can play an interesting role, e.g. regarding motivation.
Of course, there are simpler measures to determine this training activity, which can be used on a case-by-case basis. One of them is the implementation of the movement pyramid, which shows how to keep active in a progressive way without complicated explanations (Fig. 1).
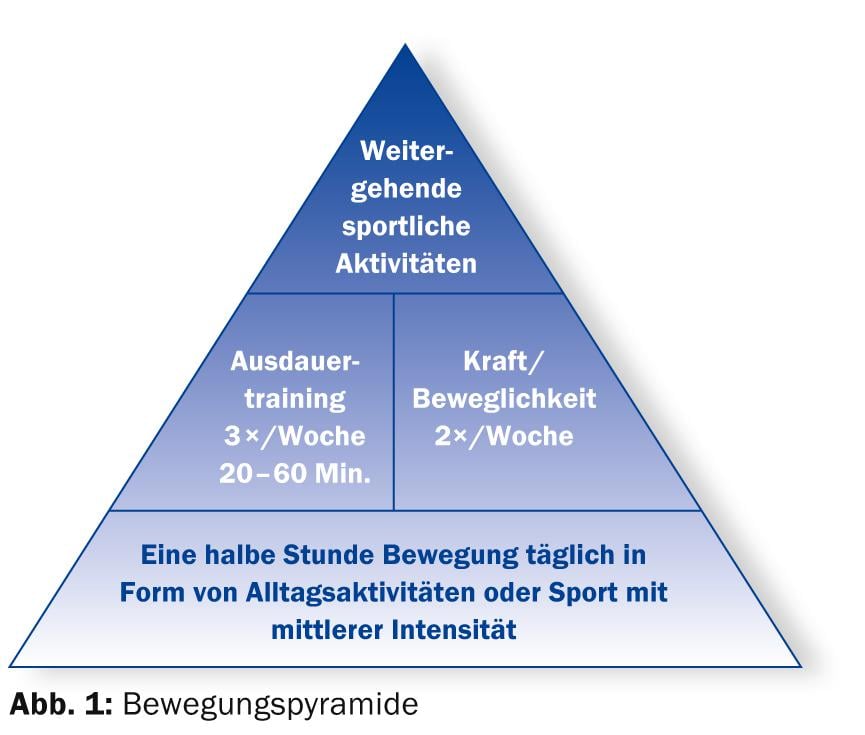
Undoubtedly, even such a “regulation” is better than nothing! Three times a week 20-60 min. Endurance training, plus strength and flexibility training twice a week should be the minimum increased prescription found on the doctor’s prescription in the future. This is a minimum, and actually only the best would be good enough in this field of medicine as well. Therefore, once again my warmest wish to all those responsible: In the future, this topic should be part of the training and continuing education. The College of Family Medicine already has such offerings (www.gesundheitscoaching-khm.ch).
HAUSARZT PRAXIS 2014; 9(6): 4-5









