Gender dysphoria (GD) is the discomfort regarding biological characteristics of birth sex and gender assignment, resulting in bio-psychosocial stress. Today, the diagnosis is considered confirmed when a professional has reached the reasoned opinion that the DSM-5 diagnostic criteria are met. In the presence of GD, a dual psychotherapeutic approach is preferable. The trans person decides for him/herself which bio-psychosocial measure he/she wants to take to reduce stress. Most trans people opt for hormonal gender reassignment first and then surgical gender reassignment.
It is Friday evening, his wife and the two children are already in bed. Mr. M. watches some more television and gets stuck on a documentary. There speaks a person who was born as a boy and tried to live the previous life also in this gender, failed in this attempt because of the other-gender experienced identity and will live her life as a woman in the future. Then he sees a man who is already successful in life, although he was raised as a girl until after graduating from canton school. He reports that his life has taken a positive turn since he no longer leads a “double life” and allows his masculinity. M. is agitated, he knows what these people are talking about in the program. M. is not a Lord, not a He. “Mr.” M. knows since youth that he is a woman. Body and soul do not go together. This report gives M. the courage to say to herself: Yes, I don’t want to have to hide anymore in the future. I want to make my body fit my identity. M. saw in the film that a person called herself “transsexual” and M. decides to call herself a trans woman from now on and to get help.
What has been the progress in recent years?
For Switzerland the common practice of “clarification and treatment of transsexualism” was last summarized in 1999 [1], therefore a reappraisal of the same is necessary and has already been redone elsewhere under the direction of the consultation for gender dysphoria of the University Hospital Zurich [2].
Among the clinical scientific advances of the past decade has been the development of a broader understanding of the “trans phenomenon” and experience. Formerly diagnosed as gender identity disorder (DSM-IV: “gender identity disorder”) or transsexualism (ICD-10), these terms were replaced by the term gender dysphoria (GD) (Table 1 ) in the Anglo-Saxon world with the publication of DSM-5 [3].
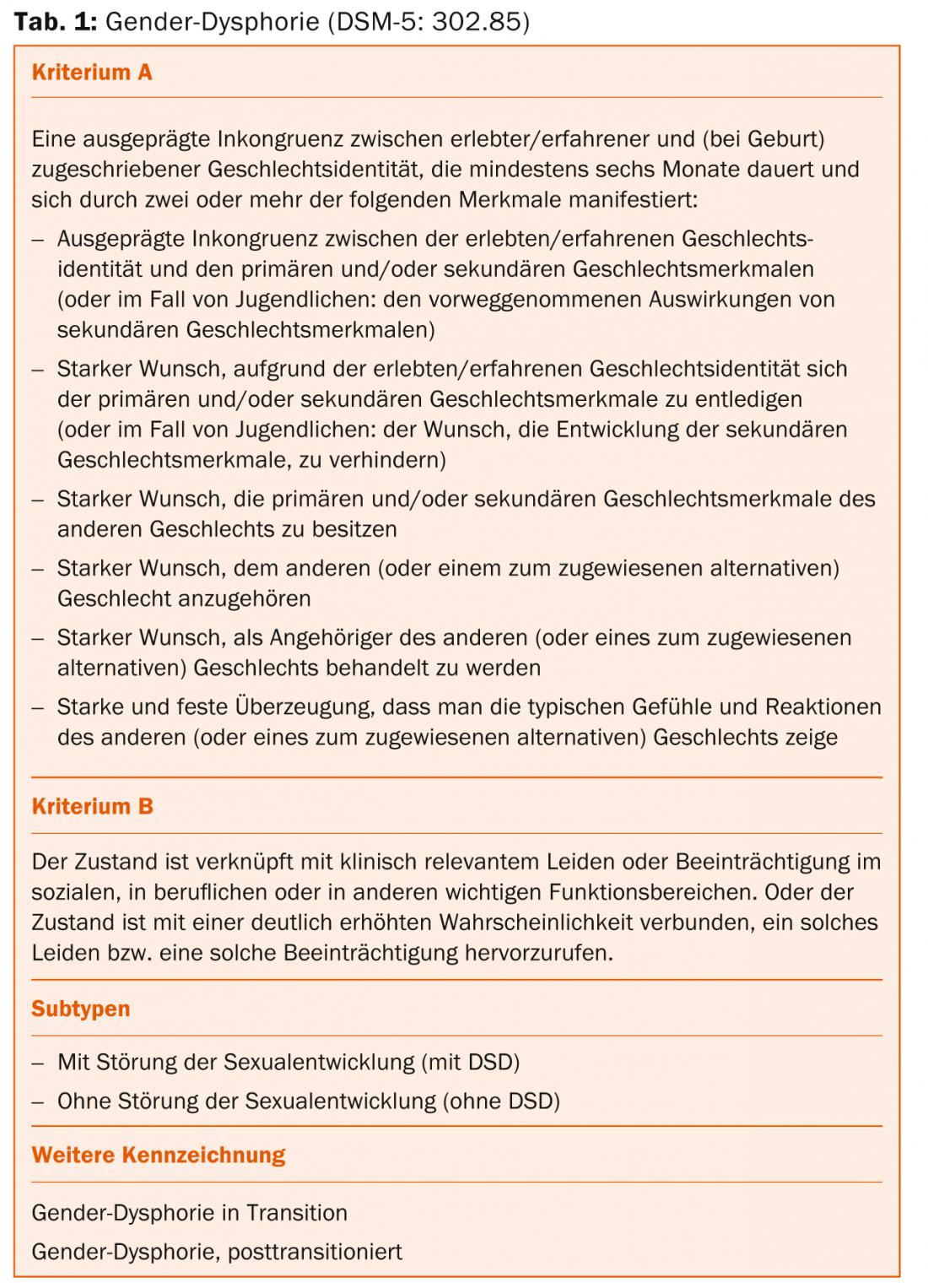
Gender Dysphoria
Formulated, GD is understood as discomfort regarding biological characteristics of birth sex and ascribed gender, which leads to bio-psychosocial stress. Considering that GD thus encompasses a much broader and no longer psychopathologically rigid gender identity spectrum according to earlier concepts, it can be assumed that the number of people who have such an experience is significantly larger than the old prevalences for transsexualism of about 2-5/100,000 [4]. Prevalence estimates in recent years assume a ratio of 1:1000 [5], but reliable figures are not (yet) available.
In clinical usage, one occasionally speaks of transidentity in addition to GD, in order to clarify the distinction from sexual disorders and the core problem, the incongruence of mental and physical experience. Individuals who report these experiences are referred to as trans women or trans men according to their experienced gender identity. Contrary to frequent assumptions by laypersons and also professionals, the gender ratio in these phenomena approaches 1:1 [4,5]. This means that the number of trans men and trans women in society is balanced.
M., now clearly a woman with a pronoun and a female first name, talks to her best friend about her experience the following week.
However, she reaps little sympathy. The boyfriend cannot accept that M. wants to be addressed as a woman in the future. Furthermore, he warns about the disadvantages of gender reassignment for M. and her children. Misunderstood, M. visits her family doctor, who refers her to a specialized psychiatric colleague after a detailed discussion.
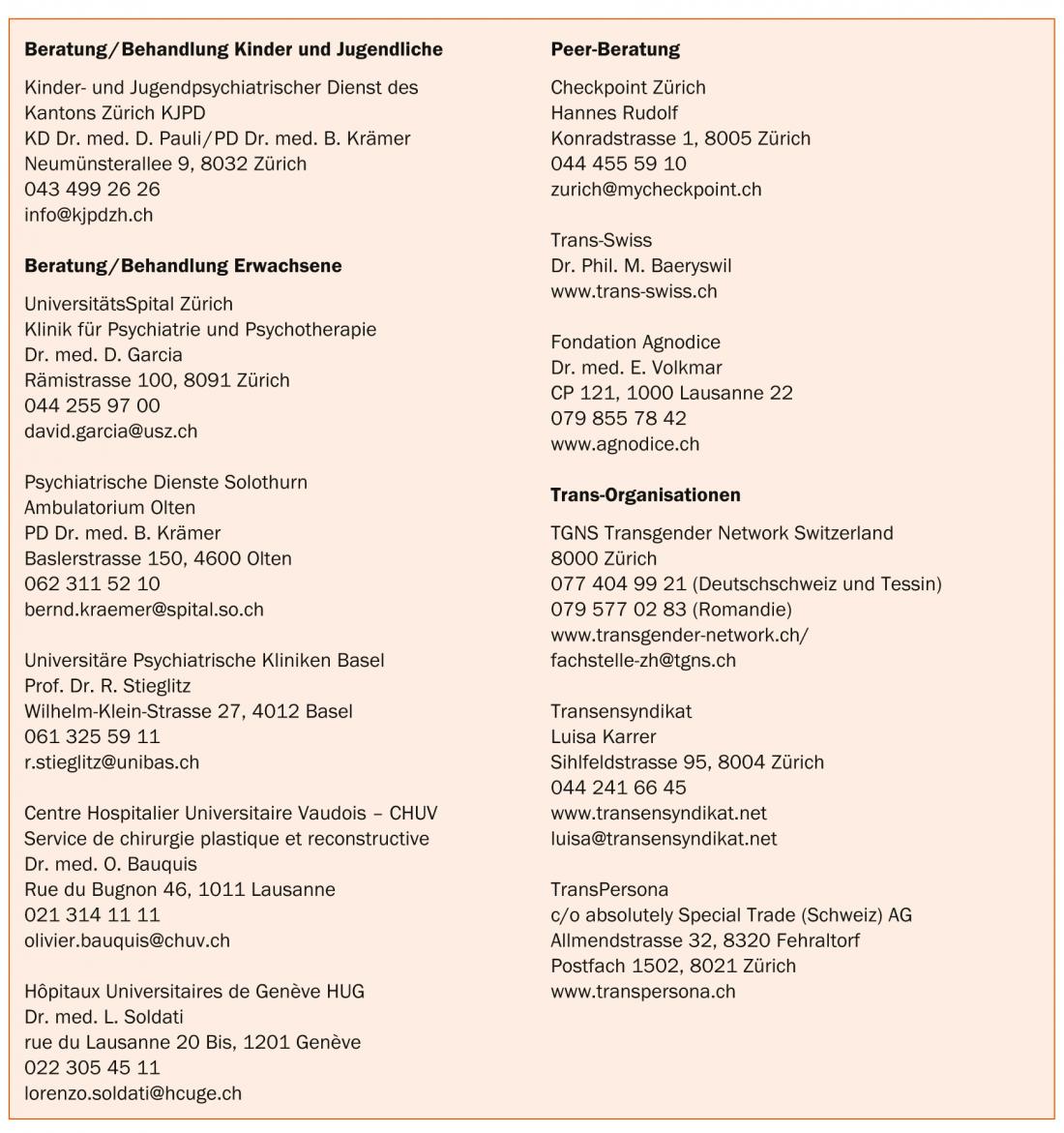
In Switzerland, there are only a few specialized centers for the accompaniment and treatment of people with GD. Some specialists in private practice also have the necessary expertise in this field. In the box a selection of addresses of special consultations, networks and self-help organizations is given. This selection serves as an orientation without claiming to be complete.
Restlessly, M. runs her hand through her hair, which she wears a little longer in the meantime. The fingernails are discreetly painted. Today is her first consultation with the psychiatrist at a specialty GD clinic. Her heart beats up to her throat when she enters the office. “I hope I don’t say anything wrong. Will he recognize my experience as a woman and believe me?” her thoughts run through her. For the first time, M. can now speak in detail about her experience and life story. Even as a child, she noticed that there was something “different” about her. She liked to play with girls, was hardly interested in football. The pubertal development of her body into a man was torture for her. It adapted to the expectations. “It will all work out,” she had thought, trying to get back to “normal” by starting a family. But in the meantime, she says, the feelings of feeling like a stranger in her own body have returned and become stronger and stronger.
Diagnostics
Currently, neither objective medical findings nor valid test psychological instruments exist for the diagnosis of GD. As an intrapsychic phenomenon whose existence cannot be stated independently of the person concerned, GD is thus a sensation that cannot be refuted. In this sense, the genderdysphoric experience represents a self-diagnosis. Most trans people have a healthy body by medical standards and often do not have clinically relevant psychiatric disorders. Nevertheless, the suffering resulting from the discrepancy between the anatomical conditions and the gender identity experience fulfills the criteria of a disorder of pathological value. Trans people seek help and try to minimize this state of experienced incongruence of body and experience [6].
After several sessions in which M. was able to talk openly about the dissatisfaction with her body and also about her past and her ideas regarding her (gender) role in the future, the treating specialist is able to confirm the GD diagnosis. On the one hand, M. is relieved to finally have security. On the other hand, she is very afraid to tell her wife and children about it. She is also worried about her job. M. is now determined to come out in all important areas of her life in her female gender identity and gender role and now needs a goal-oriented but careful accompaniment on her further way.
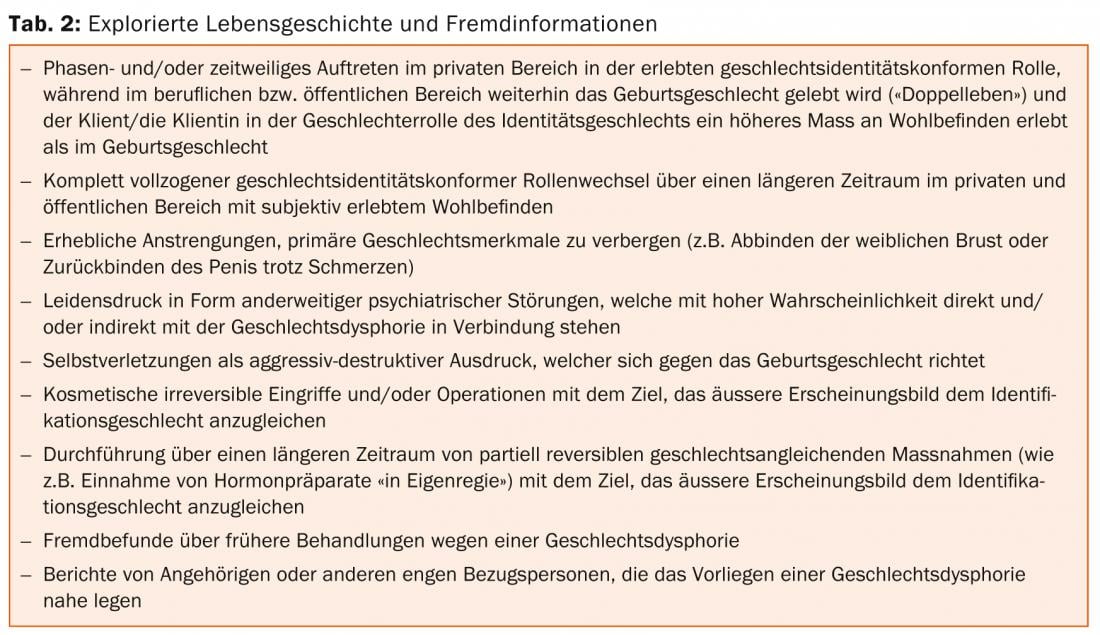
The diagnosis of GD can be considered confirmed when, after a thorough examination, a professional has come to the reasonable conclusion that the DSM-5 diagnostic criteria (Table 1) are met. At this point it is important to emphasize that the required time criterion in the diagnostic manual refers to the gender dysphoric experience and not to the psychiatric-psychotherapeutic treatment time. Therefore, depending on the discretion, the diagnostic process can be shortened. The criteria for this lie primarily in the explored life history as well as in extraneous information which, in the case of uncertainty, can plausibly substantiate the anamnestic information (Tab. 2).
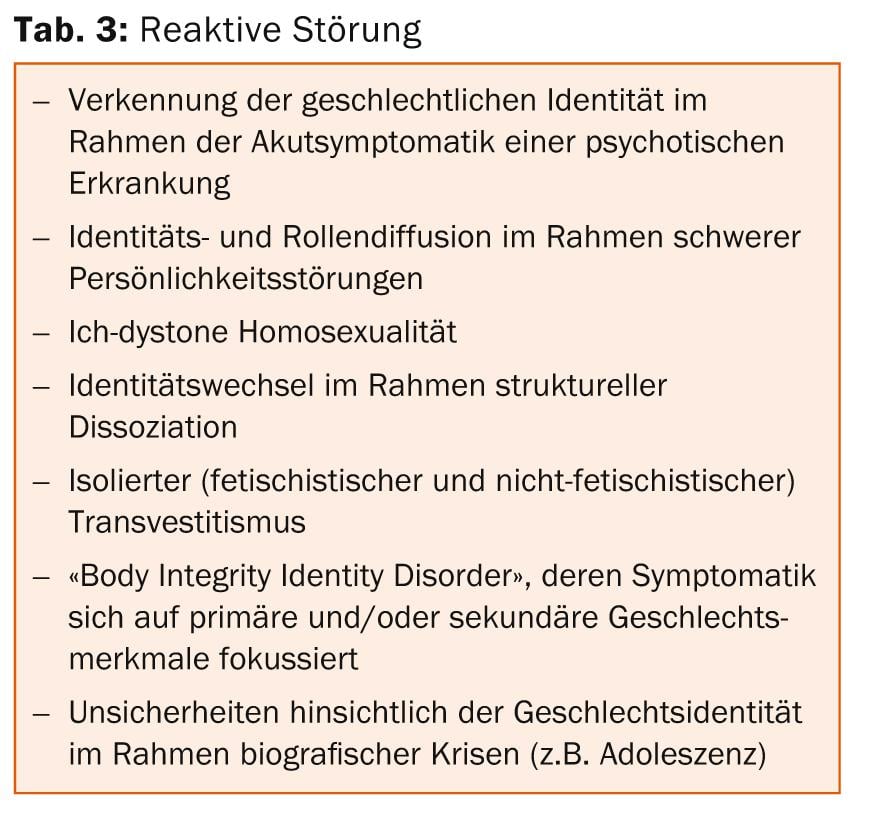
Differential diagnostic and advanced psychiatric considerations are important throughout the process. In the area of gender dysphoria, there is a great variety in subjective experience, appearance and course, personality structure, accompanying psychosocial circumstances, and sexual preference. Against the background of this heterogeneity, it is imperative to differentiate gender dysphoria from a reactive disorder (Tab. 3) in terms of differential diagnosis.
The psychiatric-psychological clarification and assessment then takes place in the sense of a procedural diagnosis. Once a GD has been identified, the focus should be on the persistence and continuity of the discomfort. Furthermore, the extent of physical, psychological and social impairment should be assessed and described. In this context, possible influencing factors as well as relevant psychodynamic correlations should be explored and named. The review of possible comorbid psychiatric disorders is a central part of this process, as is the assessment of resources.
Transition Plan
The desire for gender reassignment interventions is asked for by the professional, but is no longer considered diagnostically groundbreaking. Clearly, the trans person is in the best position to decide which bio-psychosocial measures they do and do not want to implement to reduce stress and suffering in GD. Here, a transition plan should be developed in cooperation between the client and the professional, which both sides can use as a guideline for the procedure. Providing information about the possibilities and limitations of gender reassignment surgery is useful at an early stage of the diagnostic process, but it does not replace the information provided by the specialists performing the procedure. Also, the transperson should be informed about current transition case law (especially regarding name and marital status changes).
In the presence of gender dysphoria, clinical experience suggests that a dual psychotherapeutic approach is preferable. A specialist experienced in the field of gender dysphoria is responsible for the diagnosis and the subsequent further support of the transition. With advantage, treatment of possible comorbid disorders is taken over by other psychiatric-psychotherapeutic center. Due to the major psychosocial changes and stresses of transition, outpatient psychotherapy is recommended even in the absence of psychiatric comorbidity. However, this is not a prerequisite for initiating further transition steps. In justified exceptional cases, transition support and treatment can also be carried out “in one hand”.
M. finds it very difficult to come out at work. But she is then surprised by the acceptance of the situation by her boss and colleagues. In the family, however, her outing leads to separation from her wife and children. M. suffers from the fact that they obviously still need time to accept the father as a woman. However, it is possible to maintain contact. For M., a complete coming out as a woman in all areas of life has now taken place. It is highly likely that Ms. M’s sense of belonging to the female gender will not change. The possibility of now being able to perform medical gender reassignment measures initially triggers nervousness in Ms. M..
Gender reassignment measures
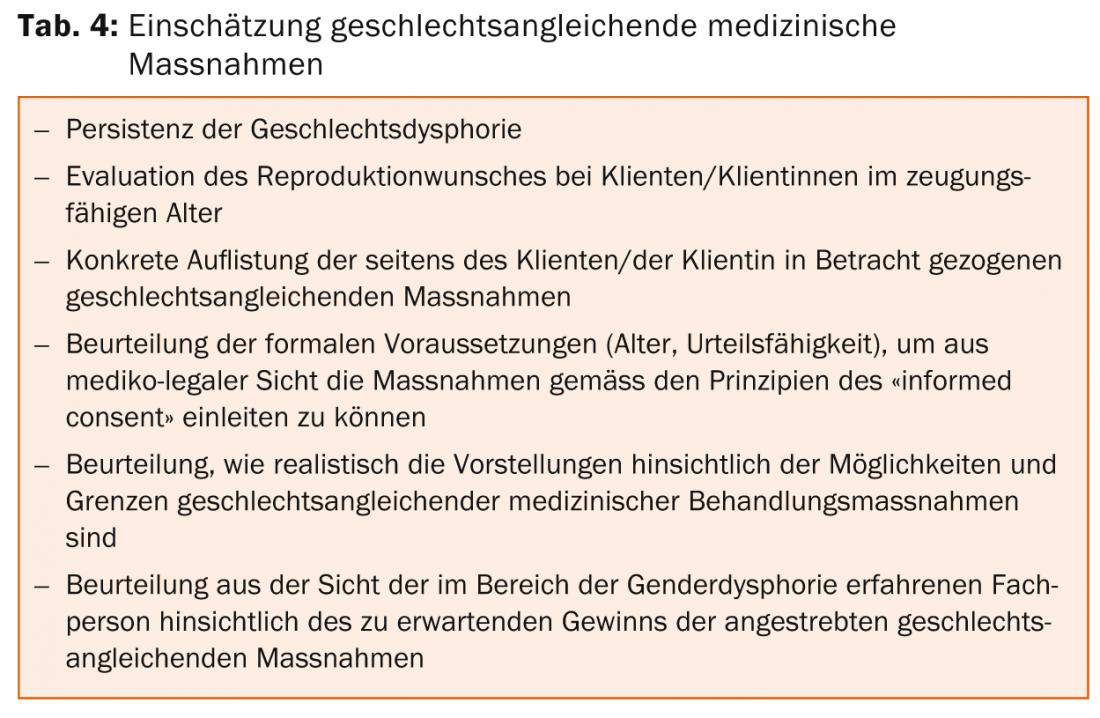
Careful, individualized, and differential diagnosis and follow-up, as outlined above, is required to make the recommendation for gender reassignment medical procedures. Therefore, in addition to the diagnostic process, an assessment should also be made on items in Table 4. Initiating gender reassignment medical procedures is a significant step in any transition.
Most trans people opt for hormonal gender reassignment first and then surgical gender reassignment. However, in some cases this order will have to be changed. Occasionally, and in accordance with the broad spectrum of the GD, it happens that clients do not want to or are not able to complete all steps – or not all within a short time. Hormone therapy as well as surgical measures are performed by specialists with proven expertise in GD. For surgical gender reassignment procedures, as with other surgical procedures, we set the minimum age of 18 years. Hormone treatment may be indicated as early as age 16. In general, there is a risk of a heart attack before surgery for at least two weeks. six months of continuous hormone therapy and a continuous daily experience in the experienced gender.
Diagnosis and treatment for children and adolescents up to age 18 requires the expertise of child and adolescent psychiatry and/or psychotherapy. It is carried out according to special criteria, which must be explained in a separate paper. The involvement of parents takes on a special significance here.
Today, M. lives as a woman according to her experienced gender. She has changed jobs and lives not far from her children in a small town. The contact with the ex-wife and the children is good, she has a new partnership with a woman. In the meantime, she was once with a man. “It wasn’t the right thing to do, though,” she says with a grin. Her hormone therapy has been established for a year, and M. is planning surgical gender reassignment steps at the region’s center hospital. M. would like to end the psychiatric support after the operation.
Literature:
- Hepp, U, Buddeberg C: Clarification and treatment of transsexualism. Schweiz Rundsch Med Prax 1999; 88(48): 1975-1979.
- Garcia Nuñez D, et al: From transsexuality to gender dysphoria – counseling and treatment recommendations in trans persons. Swiss Medical Forum, 2014 (In press).
- American Psychiatric Association, APA, DSM 5. 2013.
- Landen M, et al: Prevalence, incidence and sex ratio of transsexualism. Acta Psychiatr Scand 1996; 93(4): 221-223.
- Olyslager F, Conway L: Transseksualiteit komt vaker voor dan u denkt. Een nieuwe kijk op de prevalentie van transseksualiteit in Nederland en België. Tijdschrift voor Genderstudies 2008; 11(2): 39-51.
- Kraemer B, et al: Body image and transsexualism. Psychopathology 2008; 41(2): 96-100.
InFo NEUROLOGY & PSYCHIATRY 2014; 12(3): 26-31.









