
An expert panel finds considerable added benefit in the dual-blockade encorafenib combined with cetuximab in the treatment of metastatic colorectal cancer with BRAFV600E mutation after prior systemic therapy. This is the conclusion of a current benefit assessment.
The dual blockade consisting of the BRAF inhibitor encorafenib (BRAFTOVI®) [1] and the anti-EGFR antibody cetuximab has been approved by the European Commission since June 2020 for the treatment of patients with BRAFV600E-mutated metastatic colorectal cancer (mCRC) who have already received prior systemic therapy [1,2]. On December 17, 2020, the Federal Joint Committee (G-BA)* identified “evidence of substantial additional benefit” of dual blockade compared with the appropriate comparator therapy (irinotecan + cetuximab and FOLFIRI + cetuximab) [3,4]. According to the G-BA, there are clear advantages in the endpoint categories mortality and adverse events for therapy with the dual blockade compared to the appropriate comparator therapy. According to the G-BA, there is also an advantage for the dual blockade with regard to morbidity [4].
* The Federal Joint Committee (G-BA) consists of the four major self-governing organizations in Germany’s healthcare system (the National Association of Statutory Health Insurance Physicians, the National Association of Statutory Health Insurance Dentists, the German Hospital Federation and the National Association of Health Insurance Funds). It determines which medical services insured persons can claim. The G-BA’s assessment result forms the basis for negotiations with the GKV-Spitzenverband on the reimbursement amount.
Encorafenib combined with cetuximab: prolonging overall survival.
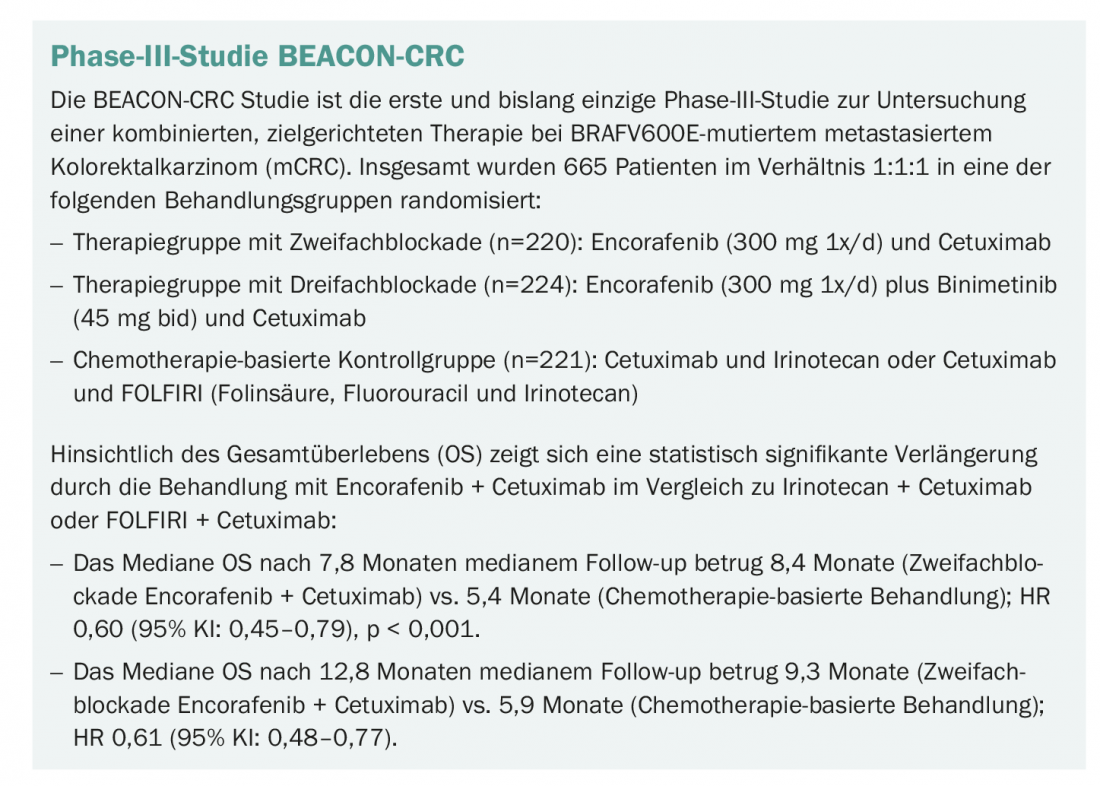
The results of the randomized, open-label, multicenter phase III BEACON-CRC trial were used for the benefit assessment (box) [3–6]. This study evaluated the combination of the BRAF inhibitor encorafenib (BRAFTOVI®) and the anti-EGFR antibody cetuximab with and without the MEK inhibitor binimetinib versus chemotherapy (FOLFIRI or irinotecan) plus cetuximab. Patients with metastatic BRAFV600E-mutated colorectal cancer who had disease progression after one or two prior systemic therapies were included. Primary efficacy endpoints were OS and ORR in the therapy group under triple blockade compared with the control group. The study was powered for the main secondary endpoint – OS in the therapy group with dual blockade versus the control group. In terms of overall survival (OS), data analysis of the trial showed a statistically significant prolongation with treatment with encorafenib + cetuximab compared with irinotecan + cetuximab or FOLFIRI + cetuximab (box). The extent of OS prolongation is assessed by the G-BA as a “significant improvement in therapeutic benefit”, taking into account the poor survival prognosis for patients with BRAF-mutated tumors and the advanced stage of disease and treatment [4]. In the endpoint category morbidity, according to the G-BA, there is a relevantly lower burden of diarrhea among patients under therapy with the dual blockade. With regard to side effects, the G-BA states “exclusively positive effects for encorafenib + cetuximab” [4]. In the endpoint category health-related quality of life, neither an advantage nor a disadvantage results from the dual blockade in the opinion of the G-BA. In its conclusion, the G-BA found “evidence of substantial added benefit for encorafenib + cetuximab over irinotecan + cetuximab or FOLFIRI + cetuximab” based on the trial data [3,4].
BEACON-CRC study retrospectively included in the evaluation.
The positive assessment of the G-BA revised the decision of an expert opinion of the Institute for Quality and Efficiency in Health Care (IQWiG) from September 2020, in which the relevant pivotal study BEACON-CRC was classified as not usable for the additional benefit assessment, since the addition of cetuximab to irinotecan or FOLFIRI in the control arm represented, according to IQWiG, an inappropriate deviation from the appropriate comparative therapy previously defined by the G-BA [7]. However, taking into account the joint opinion of the Arbeitsgemeinschaft Internistische Onkologie der (DKG), the Deutsche Gesellschaft für Hämatologie und Medizinische Onkologie (DGHO), and the Deutsche Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten e.V. (DGVS), the G-BA changed the appropriate comparative therapy by adding EGFR inhibitors (cetuximab, panitumumab) in combination with irinotecan-containing therapies [4,8]. Due to this subsequent change, the pivotal study BEACON-CRC could finally be used by the G-BA for the assessment of additional benefit. “With the ‘indication of substantial additional benefit’ for our mCRC indication, IQWiG’s initial negative assessment based on the failure to meet appropriate comparator therapy was completely revised by the G-BA,” explains Dr. Kai Neckermann, Business Unit Director Oncology (Germany-Austria-Switzerland) at Pierre Fabre. A decision by the G-BA contrary to IQWiG’s recommendation is remarkable and speaks for the high reliability of the data. “We are very pleased, as this adequately reflects the value of therapy to patients,” Neckermann added.
Based on the primary analysis of the BEACON-CRC trial, the European Commission granted approval in June 2020 for the dual blockade of encorafenib (BRAFTOVI®) plus cetuximab for the treatment of adult mCRC patients with BRAFV600E mutation after prior systemic therapy [1]. The study was conducted at more than 200 centers worldwide and was supported by ONO Pharmaceutical, Pierre Fabre, Array BioPharma/Pfizer and Merck.
Literature:
- Professional information BRAFTOVI®: Pierre Fabre Pharma GmbH, as of June 2020.
- European Medicines Agency: BRAFTOVI® (encorafenib) Summary of Product Characteristics, www.ema.europa.eu, last accessed January 2021.
- Federal Joint Committee, resolution of Dec. 17, 2020. Arzneimittel-Richtlinie/Anlage XII: Encorafenib (new indication: metastatic colorectal cancer with BRAF V600E mutation after prior systemic therapy; in combination with cetuximab), www.g-ba.de, last accessed January 2021.
- Federal Joint Committee, Supporting Reasons for the Decision of Dec. 17, 2020. Arzneimittel-Richtlinie/Anlage XII: Encorafenib (new indication: metastatic colorectal cancer with BRAF V600E mutation after prior systemic therapy; in combination with cetuximab), www.g-ba.de, last accessed January 2021.
- Kopetz S, et al: Encorafenib, binimetinib, and cetuximab in BRAFV600E-mutated colorectal cancer. N Engl J Med 2019; 381(17): 1632-1643.
- Kopetz S et al: J Clin Oncol 2020; 38(15_suppl): abstract #4001 and presentation.
- IQWiG reports – No. 976: Encorafenib (colorectal cancer) – benefit assessment according to § 35a SGB V; dossier evaluation V1.0 as of 29/09/2020. Available at: www.g-ba.de, last accessed January 2021.
- Statement on the benefit assessment according to §35a SGB V, encorafenib (new indication metastatic colorectal carcinoma), IQWiG Report No. 976; AIO, DGHO, DGVS, October 22, 2020, www.dgho.de/publikationen, last accessed January 2021.
- The Global Cancer Observatory, 2018. International Agency for Research on Cancer, World Health Organization, https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf, last accessed January 2021.
- Van Cutsem E, et al: Ann Oncol 2016; 27(8): 1386-1422.
- Modest DP, et al: Ann Oncol 2016; 27(9): 1746-1753.
- “Evidence of substantial additional benefit in BRAF-mutated mCRC: G-BA positively evaluates dual blockade consisting of encorafenib and cetuximab,” Pierre Fabre GmbH, 11/1/21.
InFo ONCOLOGY & HEMATOLOGY 2021; 9(1): 37-38.









