A heel spur is a thorn-shaped bone outgrowth on the heel bone (calcaneus). This is diagnosed by means of a lateral X-ray of the heel. Etiological factors include overuse due to calcification at the tendon insertion of the plantar tendon or Achilles tendon. The people most affected are those who are overweight, tall and very active.
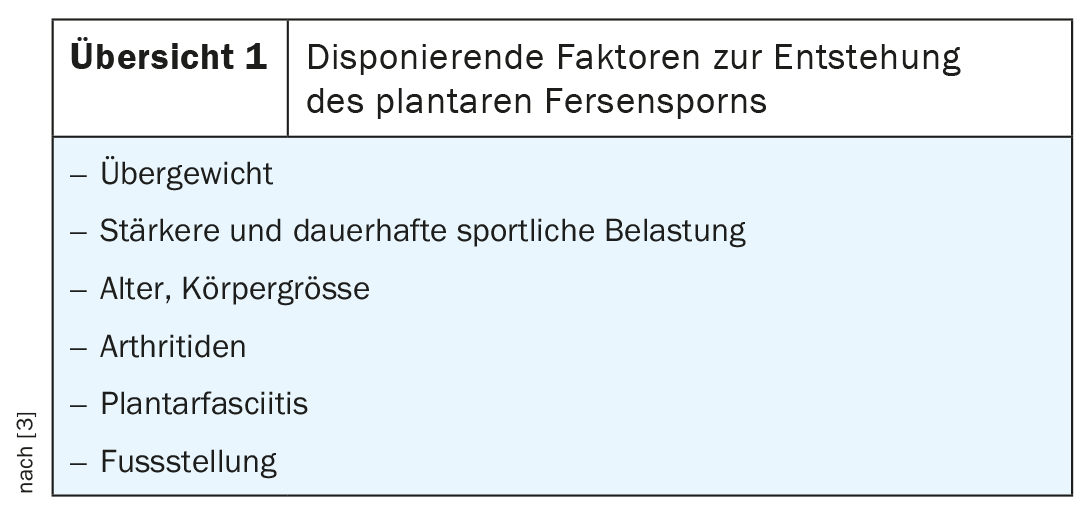
The ankle joint is a complex articulation formed by multiple bony and ligamentous structures. The mechanical load is considerable every day. The joint is therefore one of the main sites of manifestation of bony and ligamentous injuries, overuse damage and inflammation. Congenital malformations, e.g. osseous coalitions, occur. The heel spur is an expression of a long-lasting overload. Tall people and those who are overweight are more affected, due to the increased tensile forces of the tendons at the calcaneus, even those who are very active in sports. Various factors favor the development of heel spur, summarized in overview 1 [3].
The bone spur can occur plantar and dorsal, there is also an age dependence, while the sex distribution is approximately the same. In those over 70 years of age, the highest incidence of plantar spur is 41.8%; in relation to all individuals, plantar heel spur is 32.2% and dorsal spur is 13.1% [2]. The highest incidence of dorsal spur is found in the 7th decade of life. The proportion of asymptomatic calcaneal spurs is about 20% [1]. Also, the size of the spur has no correlation with the extent of symptomatology.
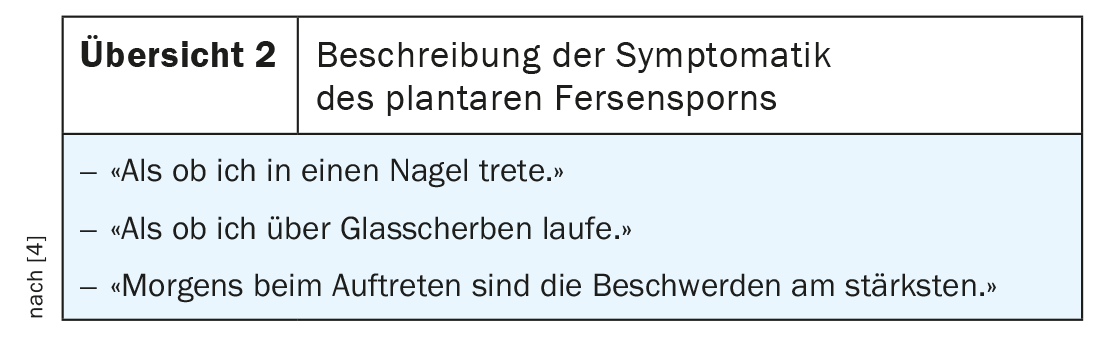
Patients with a symptomatic heel spur often use similar words to describe their complaints (overview 2) . The overuse leads to inflammation of the tendons, in this case the plantar fascia, at the base of the bone. Minute calcifications form, which become progressive with continued stress and lead to the formation of the spur. In addition to this productive fibroostitis, the rare rarefying form can also occur, which is recognizable with a circumscribed bony substance loss of the bone at the enthesis. Symptomatology can lead to unloading posture and incorrect loading [4]. Affected persons then primarily sit on the front part of the foot or put more weight on the outer edge of the foot, which leads to walking with a limp in a pointed foot position. Increasing pain in the heel at the side and in the lower leg may occur consecutively.
Radiographs in lateral projection can demonstrate productive fibroostitis and differentiate it from the rarefactive form. Contour blurring of the heel spur may indicate inflammatory activity. If no spur can be detected and other osseous changes can be ruled out, plantar fasciitis may be suspected as a differential diagnosis.
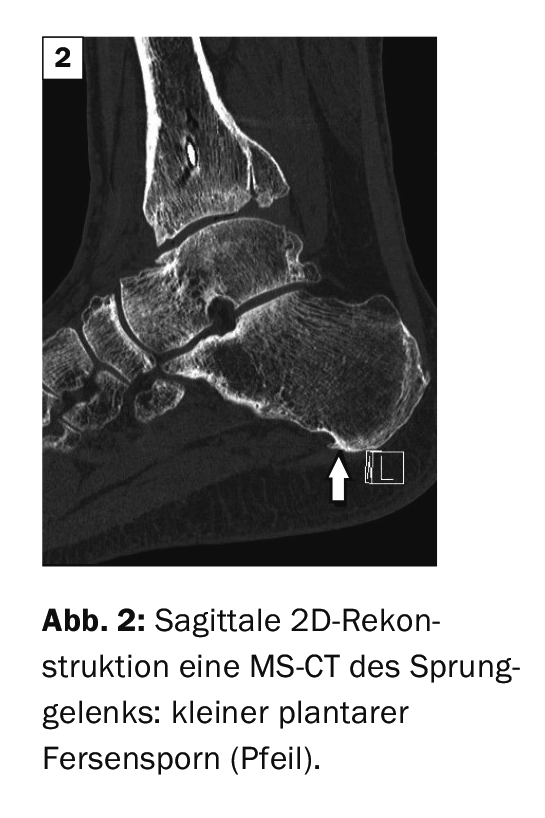
Computed tomographic examinations do not play a role in the primary imaging diagnosis of calcaneal spur. However, if a spur is present in the clarification of other issues, it can be visualized, especially in the sagittal reconstruction of the axial scans.
Magnetic resonance imaging is very good at diagnosing plantar fasciitis in particular, as well as the inflammatory activity of heel spurs. Simultaneous inflammatory changes (bursitis, tendinitis, peritendinitis, spongiosa edema) are often detectable in the surrounding area. The contrast-enhanced sequences make the extent and activity of the inflammation particularly clear.
Case studies
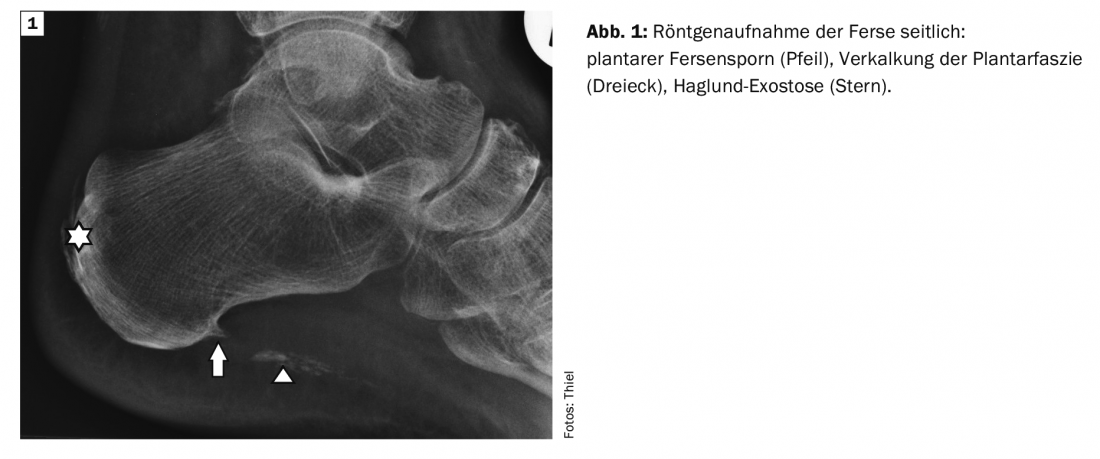
Case report 1 shows a lateral radiograph of the left ankle in a 70-year-old female patient with bilateral plantar pain symptoms on and after weight bearing a plantar and dorsal heel spur and extensive calcification in the course of the plantar fascia. The image of the right heel, which was not additionally documented here, revealed adequate changes (Fig.1). At Case 2 In a 48-year-old man, a small plantar and dorsal calcaneal spur was detected on MS-CT with sagittal reconstruction in addition to advanced arthrosis of the ankle joint for postoperative follow-up after a complex distal tibial fracture. (Fig. 2) recognizable as an incidental finding, asymptomatic in each case.
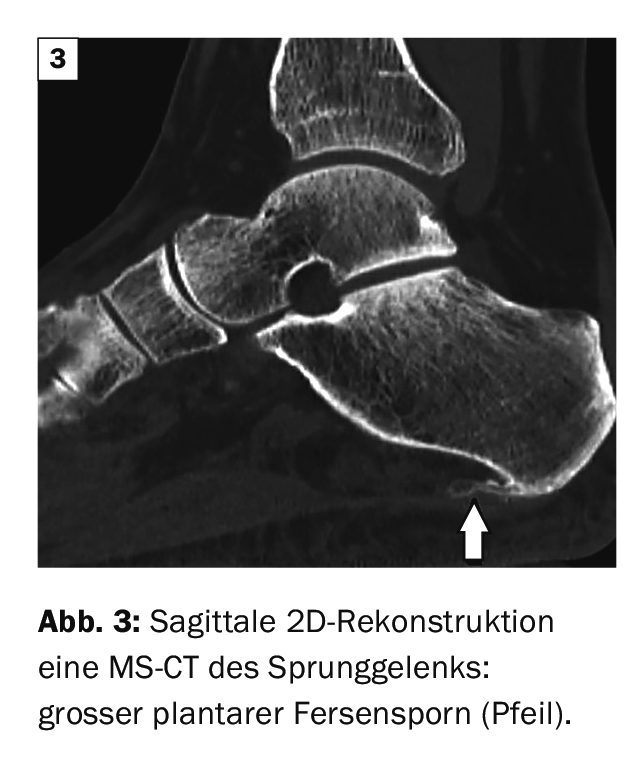
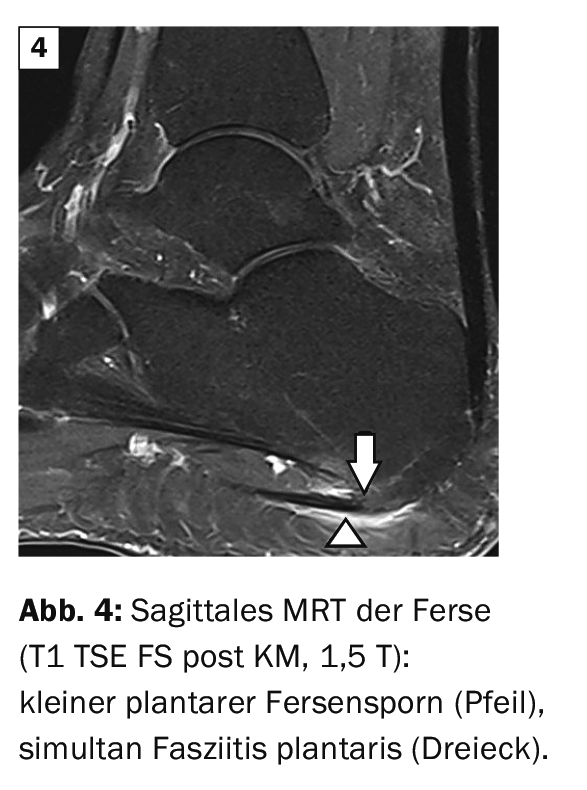
Case report 3 demonstrates a powerful plantar calcaneal spur in the sagittal 2D reconstruction of an MS-CT (Fig. 3) . The 55-year-old patient was suspected to have an insidious fracture of the calcaneus with progressive plantar pain symptoms. Case 4 shows the simultaneous appearance of plantar calcaneal spur and fasciitis plantaris on contrast-enhanced MRI of the heel region (Fig. 4). of a 67-year-old woman with significant plantar pain.
Literature:
- Alatassi R, Alajlan A, Almalki T: Bizarre calcaneal spur: A case report. Int J Surg Case Rep 2018; 49: 37-39.
- Beytemür O, Öncü M: The age dependent change in the incidence of calcaneal spur. Acta Orthop Traumatol Turc 2018; 52(5): 367-371.
- Kirkpatrick J, Yassaie O, Mirjalili SA: The plantar calcaneal spur: a review of anatomy, histology, etiology and key associations. J Anat 2017; 230(6): 743-751.
- Orthopaedic Joint Clinic: www.gelenk-klinik.de (last accessed 04/22/2021).
HAUSARZT PRAXIS 2021; 16(5): 35-36









