
Complex Physical Decongestion – manual lymphatic drainage combined with consistent compression – is the gold standard in the treatment of lymphedema. Overview of the classification of lymphedema and its stages as well as diagnostics and conservative therapeutic approach.
Lymphedema is a chronic disease of the interstitium resulting from primary or secondary damage to the lymphatic drainage system. Under physiological conditions, there is a balance between the fluid filtered through the blood vessel wall into the interstitium and not reabsorbed and its removal from the interstitium via the lymphatic system [1]. Here, intravascular colloidosmotic pressure is responsible for the reabsorption of interstitial fluid into the capillary bed, i.e., the ability of proteins to bind water. Because some proteins also cross over into the interstitium, they counteract intravascular KOD, and not all filtered water can be reabsorbed. These proteins and the fluid bound to them, as well as other interstitial substances requiring lymphatic drainage (bacteria, viruses, cell detritus, leukocytes, macrophages, immunoglobulins, etc.) must be drained and removed via the lymphatic system. Recent studies indicate that the lymphatic fluid volume appears to be larger than previously thought [2].
Consequently, edema occurs whenever filtration is greater than KOD and lymphatic drainage. Lymphedema forms as soon as the lymphatic drainage is structurally or functionally no longer guaranteed. The lymphoid proteins and fluid in the interstitium accumulate, and tissue alteration occurs during the course, although the exact mechanisms are not known. Thus, lymphedema develops into a chronic and progressive disease. The risk of erysipelas is increased, which in turn affects the lymphatic vessels [1].
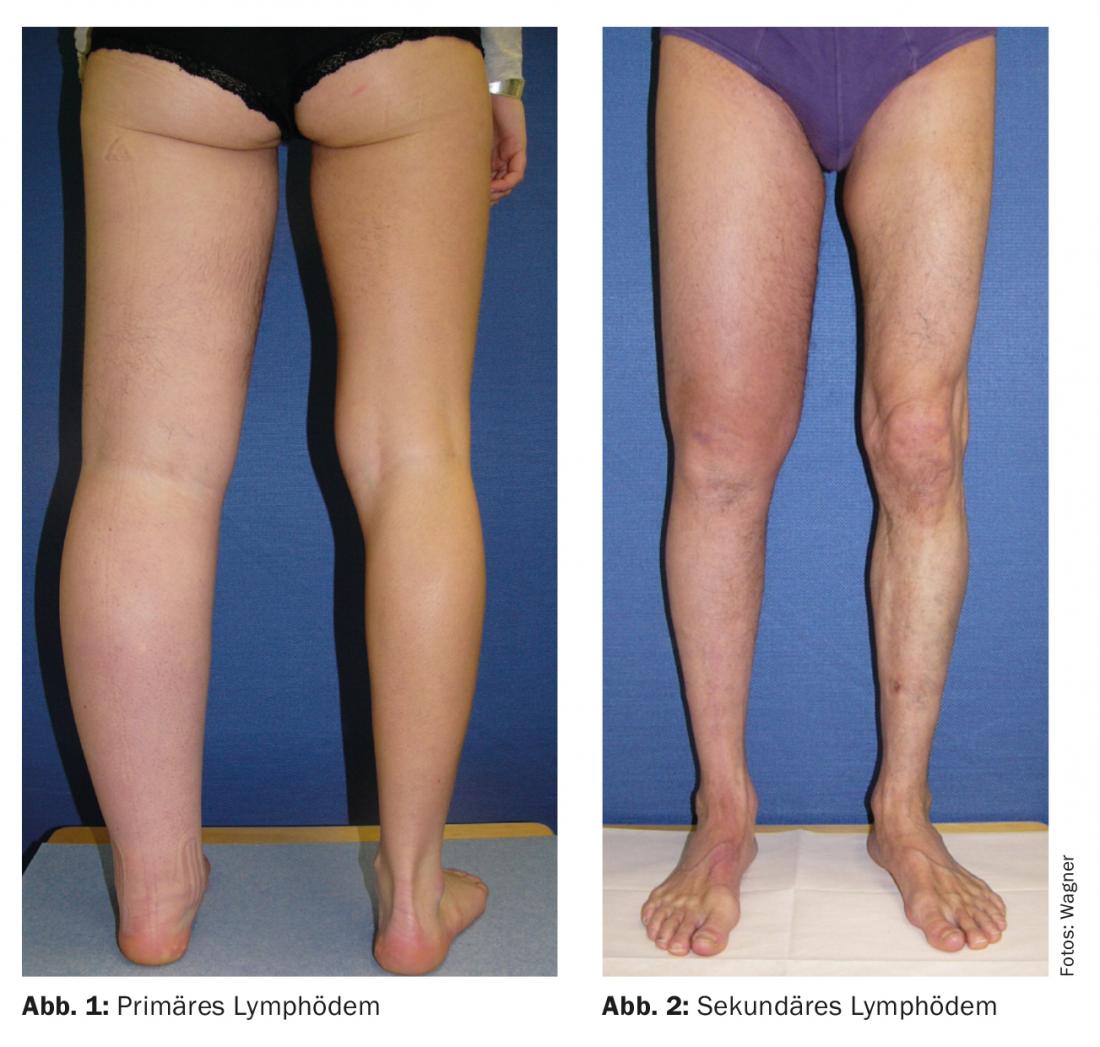
The primary lymphedema
Only about 1% of all lymphedema is of primary etiology, with primary lymphedema (Fig. 1) occurring mostly sporadically and less often hereditary or symptom-associated [3]. The cause is a hypo- or hyperplastic/dysplastic layout of the lymphatic vascular system, lymph node fibrosis or akinesia. In most cases, mixed forms are present [4]. Primary lymphedema is more commonly localized to the lower extremities and is usually unilateral. The first clinical signs appear in the periphery (toes, fingers) and spread proximally over time. Epidemiologically, primary lymphedema is poorly studied. The incidence of primary lymphedema at birth is estimated to be approximately 1:6000 [5], and the prevalence in those under 20 years of age is approximately 1:87,000 [6]. Initial manifestation in boys often occurs in the first twelve months of life, and in girls around puberty. However, initial manifestation can occur at any age. Women are about five times more likely to be affected [7–9].
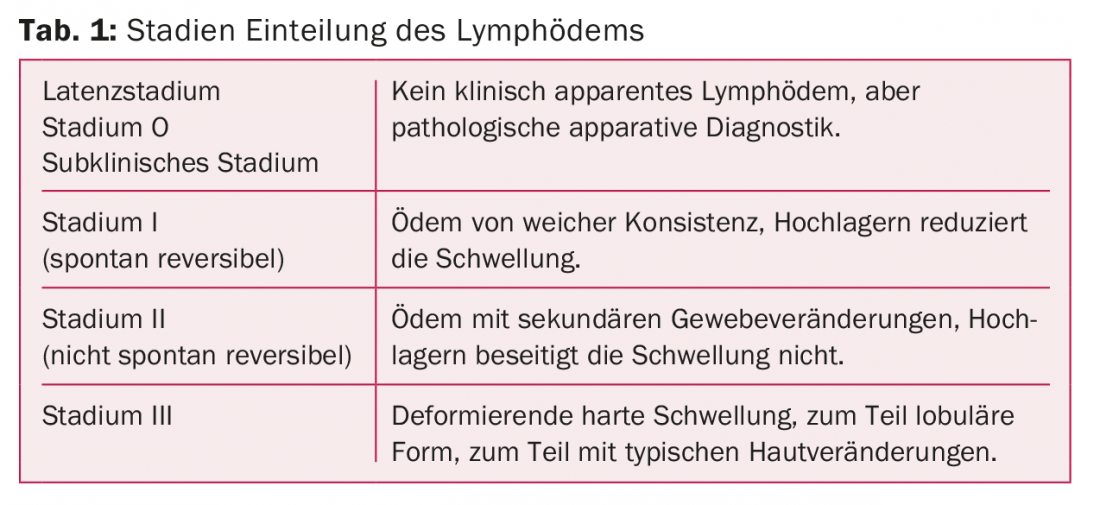
The secondary lymphedema
The cause of secondary lymphedema (Fig. 2) is an acquired interruption of lymphatic drainage. This may be the result of “benign” lymphatic injury (trauma, surgery, chronic infections) or tumor-associated (“malignant”). Clinically, secondary lymphedema manifests from the site of interruption peripherally.
Worldwide, the most common secondary cause is filariasis, a nematode that lodges in the vascular system, leading to obliteration of the lymphatic capillaries via chronic inflammation. In industrialized countries, tumor therapy is the main cause of secondary lymphedema. With axillary lymph node excision, the incidence is approximately 20% [7] After sentinel lymph node excision, an incidence of up to 5% is still listed [10], with increased breast lymphedema observed. In surgeries involving abdominal, pelvic, or inguinal lymph node removal, an average lymphedema incidence of approximately 16-20% has been described [11–13], even up to 50% depending on the radical nature of the surgery [14]. It is certain that the number of removed lymph nodes as well as the localization play a role. Pre-existing obesity and perioperative infections increase the rate of lymphedema. Radiation therapy is also described as a risk factor. Not secured is chemotherapy.
Lymphedema is divided into four stages according to Földi [15] and ISL (International Society of Lymphology) [16] (Table 1).
Diagnostics
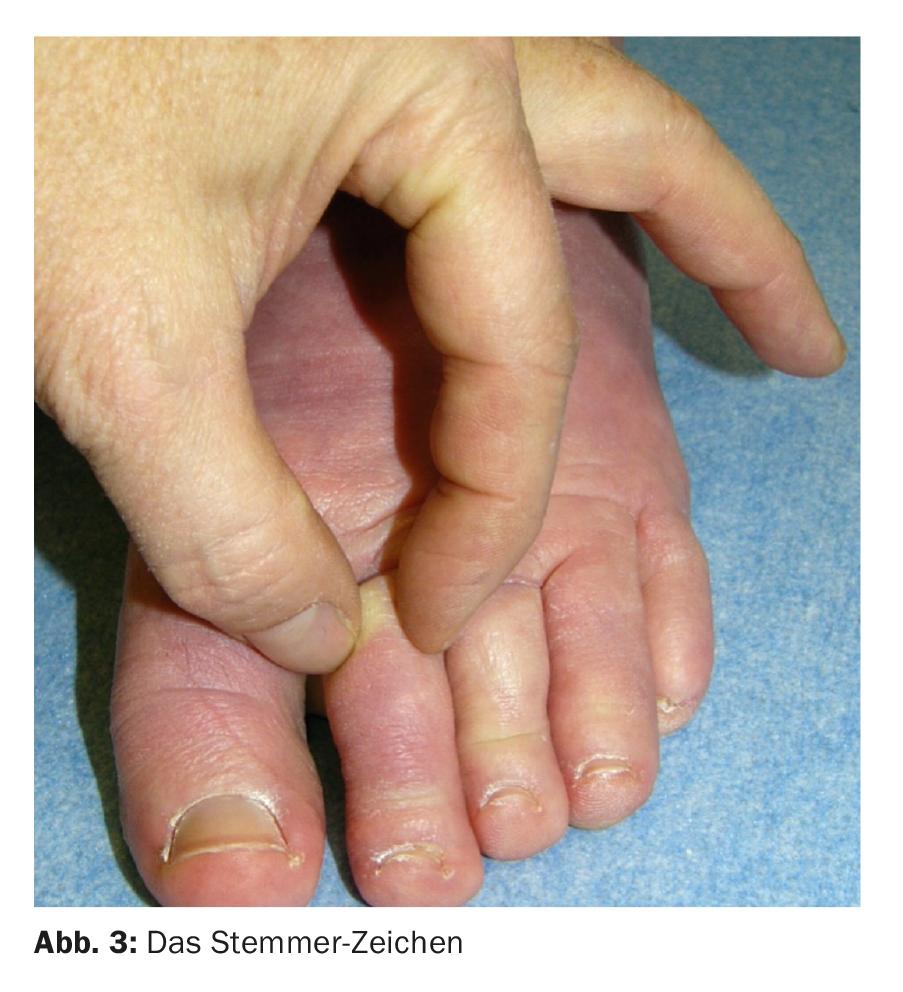
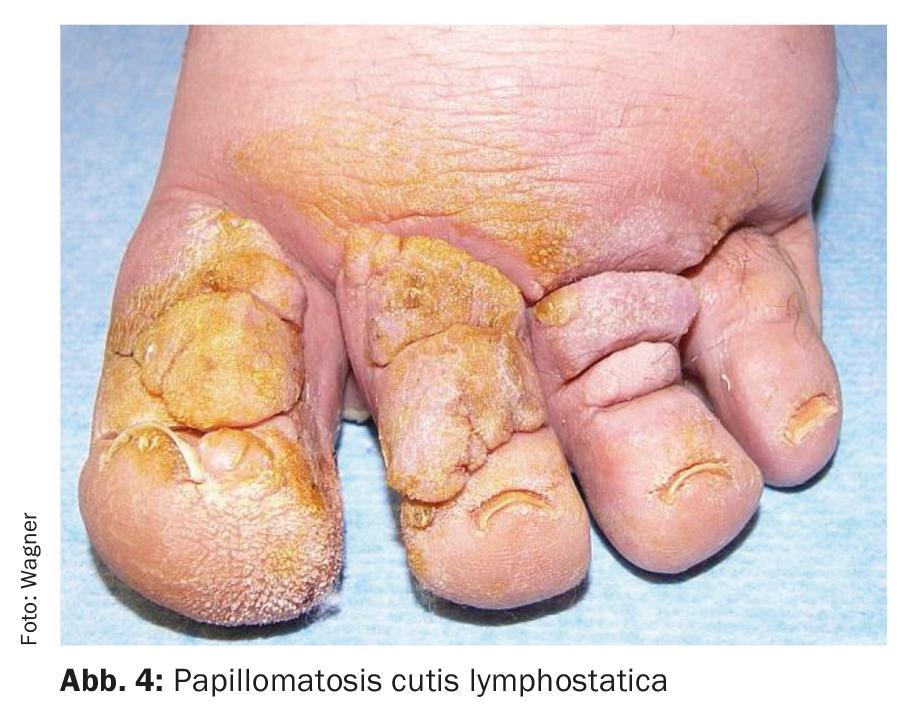
Basic diagnostics, i.e. history, inspection and palpation, are usually sufficient to establish the diagnosis, provided that lymphedema is even considered as a differential diagnosis. Of course, it is important to exclude other edema-inducing clinical pictures [17]. This is especially true for the exclusion of tumor-induced secondary lymphedema at diagnosis. Anamnestically, the patient describes a swelling that is initially regressible and usually not realized for a long time, but then increasingly persists. Often there is also a triggering event such as a sprain or mosquito bite with swelling that does not subside. This is usually unilateral, if bilateral typically asymmetric. Especially in primary edema, the toes and fingers are almost always affected during the course and the Stemmer’s sign is positive (non-removable skin fold on the second toe or finger dorsum (Fig. 3). In addition, the fine skin folds over the toes become scarified, and coarser skin folds begin to form at the base of the toes. Fibrosis may be palpated. The tissue is soft at first, but as it progresses it becomes increasingly difficult to press in because of fibrosis, and secondary skin changes such as papillomatosis cutis lymphostatica (Fig. 4) may develop.
Instrumental diagnostics are rarely necessary. Fluorescence microlymphography is established in Switzerland, and functional scintigraphy in Germany. Indocyanine green lymphography has been established in recent years for preoperative planning and postoperative control, but not for diagnostic purposes. Ultrasound, MR, direct and indirect lymphography can be helpful for specific questions, but are not used for primary diagnosis.
The conservative therapeutic approach
Assuming that we always have edema when filtration is greater than colloid osmotic pressure and lymphatic drainage combined, each of these factors can in principle be targeted (Fig. 5). In the case of lymphedema, compression therapy and manual lymphatic drainage are specifically used here. Diuretics are contraindicated, especially in the younger patient, because they promote fibrotic tissue remodeling in the long term. They may be necessary selectively at the beginning of a decongestion phase to prevent heart failure. Infusions with human albumin are reserved for intensive care medicine when specifically indicated. Manual lymphatic drainage stimulates the lymphatic vessels from central to peripheral, creating a suction effect, which drains the interstitial space. The lymphatic drainage grips are designed in such a way as to avoid a massage effect with consecutive hyperemia of the tissues and enhancement of filtration.
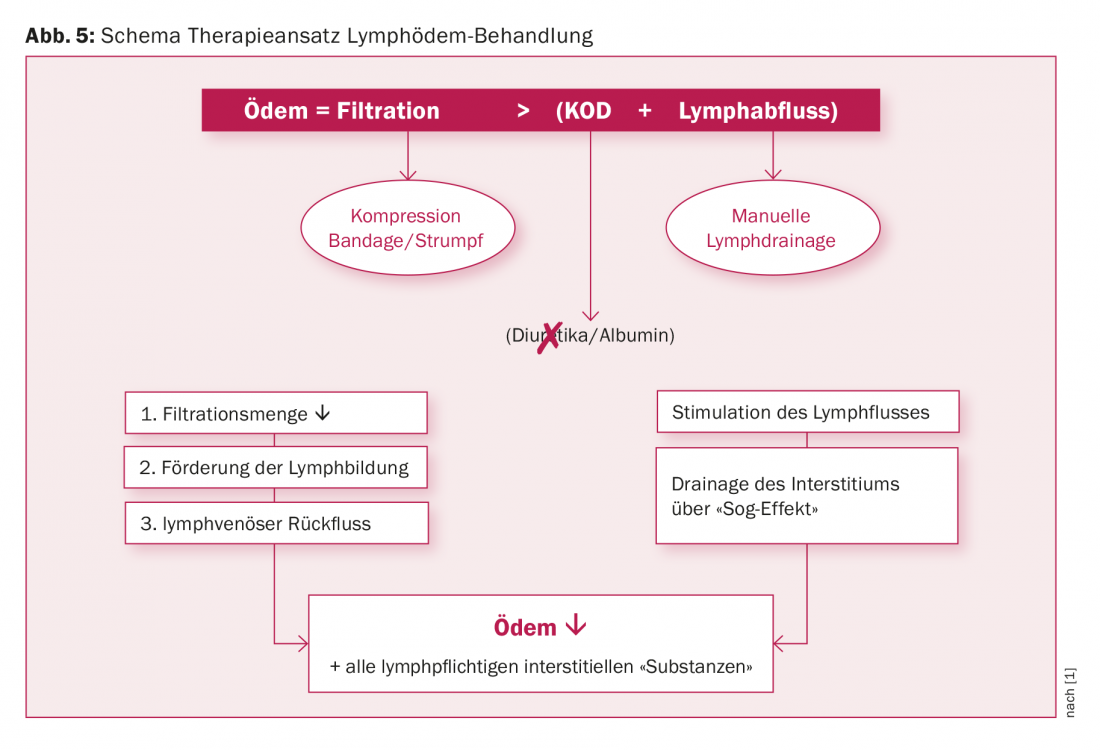
As the most important conservative measure, compression from the outside counteracts the filtration pressure, so that the filtration volume decreases in a pressure-dependent manner and thus also the lymphatic volume remaining in the interstitium. However, compression also shifts the interstitial fluid toward the draining lymphatic capillaries and supports lymphatic drainage.
The complex physical decongestive therapy
The combination of manual lymphatic drainage with compression therapy is called complex physical decongestion. A distinction is made between the decongestion phase and the maintenance phase. The decongestion phase involves edema reduction and softening of fibrotic tissue. During this intensive phase, treatment is ideally daily (or several times a week) with application of a short-stretch compression bandage, which requires a lot of skill and experience. The decongestion phase can often be performed on an outpatient basis. If the clinic is very advanced, or if intensive patient education is necessary, inpatient treatment at a specialized clinic is recommended. Once the goal has been reached, the treatment moves into the maintenance phase, in which treatment is adapted to the clinic, which is often necessary on a weekly basis. Regular treatment is beneficial to keep the concentration of lymphoid proteins accumulating in the interstitium as low as possible. However, consistent compression therapy with a compression stocking is always obligatory in this phase as well. The compression stocking in the patient with lymphedema should be of the “flat knit” type. Flat knit compression stockings typically have a seam. Physically, they are more short-legged than standard circular knit socks, thus exhibiting increased stiffness and working pressure, and less fatigue over the course of the day. Flat knit compression stockings are usually appropriate in orthopedic stores and it is recommended to prescribe them with MiGel number 17.10…. The optimal compression stocking fitting is individual and must be worked out. Sometimes it is better to combine two “class II” compression stockings and put them on top of each other than just one compression class IV. On the one hand, the compression pressures add up, on the other hand, especially the stiffness of the knitted fabric increases, which best counteracts swelling. Prescribed compression stockings should always be checked by a doctor. This shows the patient the importance of this therapy and, in addition, a good fit increases wearer discipline.
The patient affected by lymphedema is a very important player in the therapy. Without his compliance, a lasting result is hardly achievable. This requires that the patient be educated, about the clinical picture, skin care, and the need for consistent compression therapy. Depending on the clinical situation and possibility, this may include teaching self-bandaging as well as simple self-drainage grips. This training is very time-consuming and costly. In addition to the specific therapy, the usually existing muscular imbalance must be addressed physiotherapeutically and the patient should be shown decongestion exercises in dry and also in water. Aquajogging or swimming in water below 30 degrees is an excellent remedy because, on the one hand, compression is exerted and, on the other hand, a kind of lymphatic drainage effect occurs due to the movement in the water. All these measures are time-consuming. The necessary therapy discipline can usually only be achieved in a well-functioning network around the patient. This includes the patient’s attending physician, therapist, stocking provider, family, employer, and others in the patient’s community.
Lymphedema and sport
All studies that have investigated sporting activity in lymphedema patients have always started from the question of whether sport could do harm. None of the studies demonstrated this. Individual studies showed a tendency toward volume depletion. A significant volume decrease was found only with Nordic walking in patients with arm lymphedema [18]. Sports under the compression is more beneficial than without. However, exercising without compression does not appear to be persistently detrimental [19,20]. From the studies and recommendations, it can be concluded that there are actually no athletic limitations, but that there are individual limitations. In principle, any sporting activity is beneficial because it usually helps to increase the quality of life [21].
Complementary therapy measures
Many patients with lymphedema require additional support from clinical psychology to promote acceptance of the disease, which again affects compliance. The fact that it is a chronic disease that requires daily attention can be very stressful. Also, arm lymphedema is difficult to hide in public or the choice of clothing is limited in leg lymphedema. Entering into a relationship and including sexuality also requires a lot of understanding from the partner.
All the therapeutic measures listed so far bring about an improvement in the clinic, in some cases considerable, but they do not lead to a cure. They improve quality of life by controlling symptoms and edema as well as preventing complications (erysipelas, fibrosis, ulceration to immobilization). The goal of comprehensive treatment must be to maintain the ability to work and the highest possible quality of life. This is not always easy, as the affected patient often has to spend a lot of time on the therapies. The desire for additional therapeutic options is therefore understandable.
Differential diagnosis lipedema
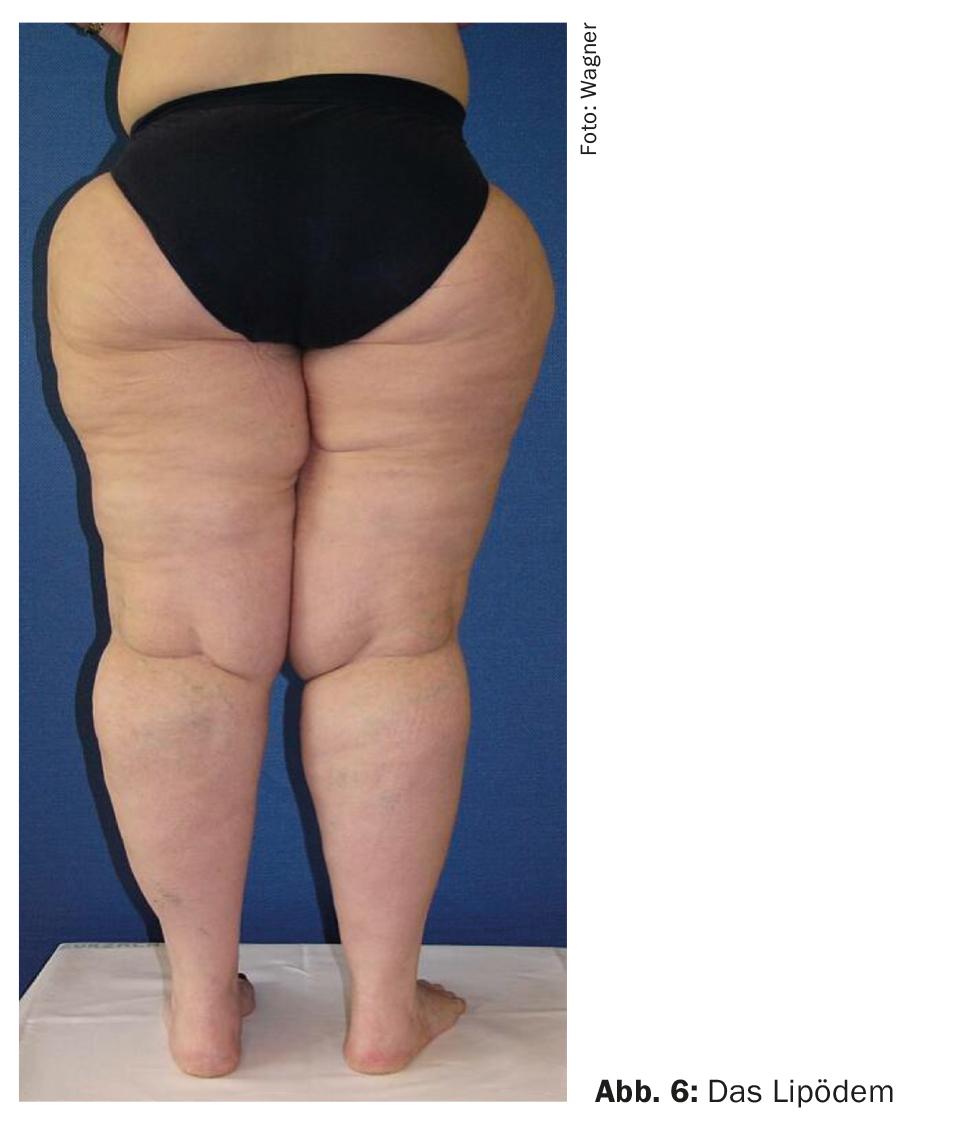
A frequently observed differential diagnosis to lymphedema is female patients with lipedema (Fig. 6). This is a subcutaneous fat cell hypertrophy and hyperplasia mostly affecting the lower extremities, with an orthostatic tendency to edema, which over time leads to daily, sometimes disabling pain. In the course, secondary lymphedema may develop, but stasis dermatitis or ulceration may also be observed. Typically, a disproportion is found between the lower body and upper body with a slender waist. The clinical picture of lipedema is not to be equated with obesity. But body weight gain is considered a risk factor and leads to progression, which usually responds only frustratingly when weight is reduced by dietary measures. That is why weight consistency is very important. Because of this risk factor, many patients with lipedema tend to be obese. Despite this, you can often see a slim waist. Conservative therapy includes the same elements of CPD as for lymphedema, in addition to nutritional counseling and promotion of physical activity [1,22].
Take-Home Messages
- Lymphedema is a chronic and so far not curatively treatable disease with a great impact on the quality of life.
- Diagnosis and correct initiation of therapy are often delayed.
- The gold standard of treatment to date has been Complex Physical Decongestion (CPD), which is manual lymphatic drainage combined with consistent compression.
- Good compliance can only be achieved through time-intensive education of the patient with assumption of personal responsibility in dealing with the condition.
Literature:
- GDL Guideline Lymphedema: S2k Guideline Diagnostics and Therapy of Lymphedema AWMF Reg. No. 058-001 www.awmf.org/uploads/tx_szleitlinien/058-001l_S2k_Diagnostik_und_Therapie_der_Lymphoedeme_2017-05.pdf
- Levick JR, Michel CC: Microvascular fluid exchange and the revised Starling principle. Cardiovasc Res 2010; 87(2): 198-210.
- Vignes S.: Lymphedema from diagnosis to treatment. Rev Med Intern 2017; 38(2): 97-105.
- Kinmonth JB: Fibrosis in lymphnodes in primary lymphedema. Ann R Coll Surg Engl 1980; 62: 344-354.
- Dale RF: The inheritance of primary lamphedema. J Med Genetic 1985; 22(4): 274-278.
- Smeltzer DM, et al: Primary lymphedema in children and adolescents: a follow up study and review. Pediatrics 1985; 76(2): 206-218.
- Moffatt CJ, et al: Lymphoedema: an underestimated health problem. QJM 2003; 96(10): 731-738.
- Neuhüttler S, Brenner E: Contribution to the epidemiology of lymphedema. Phlebology 2003; 35: 181-187.
- Brunner U: Perimed 1985: 39-47.
- Di Sipio, et al: Incidence of unilateral arm lymphedema after breast cancer: a systematic literature review and metaanalysis. The lancet oncology 2013; 14(6): 500-515.
- Cormier JN: Lymphedema beyond breast cancer: a systematic review and meta-analysis of cancer-related secondary lymphedema Cancer. 2010; 116(22): 5138-5149.
- Todo Y: Close relationship between removal of circumflex iliac nodes to distal external iliac nodes and postoperative lower-extremity lymphedema in uterine corpus malignant tumors. Gynecol Oncol 2015; 139(1): 160-164.
- Yamazaki H: Relationship between removal of circumflex iliac nodes distal to the external iliac nodes and postoperative lower-extremity lymphedema in uterine cervical cancer. Gynecol Oncol 2015; 139(2): 295-299.
- Ryan M: Aetiology and prevalence of lower limb lymphoedema following treatment for gynaecological cancer. Aust N Z J Obstet Gynaecol 2003; 43(2): 148-151.
- Földi E, et al: On the diagnosis and therapy of lymphedema. Dtsch Ärztebl 1998; 95: A-740-747.
- Consensus document Lymphology 2016; 49: 170-184.
- Stöberl C: Clinical differential diagnosis of leg swelling – a guide for practice. Z Vascular Med 2011; 8(1): 11-18.
- Jönsson C: The effect of pole walking on arm lymphedema and cardiovascular fitness in women treated for breast cancer. A pilot and feasibility study. Physiother Theory Pract 2014; 30(4): 236-242.
- Singh B: Effects of compression on lymphedema during resistance exercise in women with breast cancer related lymphedema: a randomized crossover trial. Lymphology 2015; 48(2): 80-92.
- Johansson K: Low intensity resistance exercise for BC Patients with arm lymphedema with or without compression sleeve. Lymphology 2005; 38(4): 167-180.
- Brown JC: Physical activity, daily walking, and lower limb lymphedema associate with physical function among uterine cancer survivors. Support Care Cancer 2014; 22(11); 3017-3025.
- S1 Guideline Lipedema AWMF Register Number 037-012 2016; www.awmf.org/uploads/tx_szleitlinien/037-012l_S1_Lipoedem_2016-01.pdf
CARDIOVASC 2017; 16(5): 6-10









