Patients with severe mitral regurgitation (MI) and high surgical risk are often treated conservatively, despite high morbidity and mortality from the underlying condition. Since 2009, a new percutaneous procedure has been available in Switzerland to treat such patients.
This technique allows mitral valve repair via femoral transvenous access and transseptal puncture. This procedure is performed under anesthesia on the beating heart (without a heart-lung machine) under fluoroscopic and echocardiographic control. In this procedure, a steerable catheter is used to staple the anterior and posterior mitral valve leaflets together with one (or more) clips. Most patients do not require intensive care after the procedure and can leave the hospital within a few days. More than 80% of patients show a significant improvement in symptoms as well as performance. This therapy is used only in patients at high surgical risk for conventional mitral valve surgery.
Introduction
Mitral regurgitation (MI) is the most common valvular disease in general and – after aortic stenosis – the second most common in hospitalized patients [1]. The prevalence of moderate MI is about 2.0% and severe MI is 0.2%, and it is increasing with age. The course of the disease is often gradual and symptoms usually appear only in advanced stages. Treatment of severe MI has been the domain of cardiac surgery. Surgical mitral valve reconstruction (MKR) is now the therapy of choice for the correction of MI of various etiologies because it is superior to mitral valve replacement in terms of perioperative morbidity and mortality and long-term outcomes. However, many patients are diagnosed late, at a time when the surgical risk for MKR is high [2]. In recent years, various new percutaneous treatment methods have been developed, which could become a real alternative to surgical treatment primarily for this group of patients.
The MitraClip system allows the two mitral valve leaflets to be clipped together at specific points, thus reducing the backflow of blood through the mitral valve. The clip is made of an MRI-compatible metallic alloy (Fig. 1) . To date, this technique has been used in more than 6000 patients worldwide.
Patient selection
The indication for mitral valve repair is made after extensive invasive and echocardiographic evaluation. The decision whether surgical rehabilitation or MitraClip intervention should be preferred is made on a case-by-case basis in a multidisciplinary conference. We believe this discussion forum is essential to define the optimal procedure for each patient.
The feasibility of the procedure is defined by specific echocardiographic criteria. Echocardiographic evaluation using 3D transesophageal echocardiography (TEE) has proven useful in this regard.
Technology
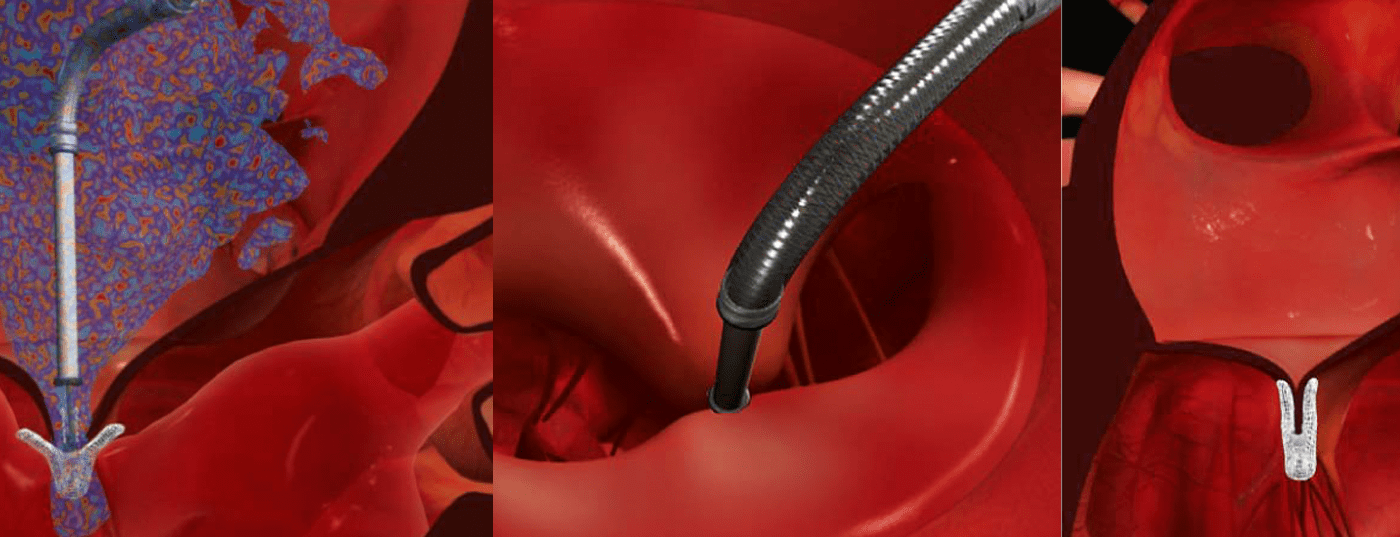
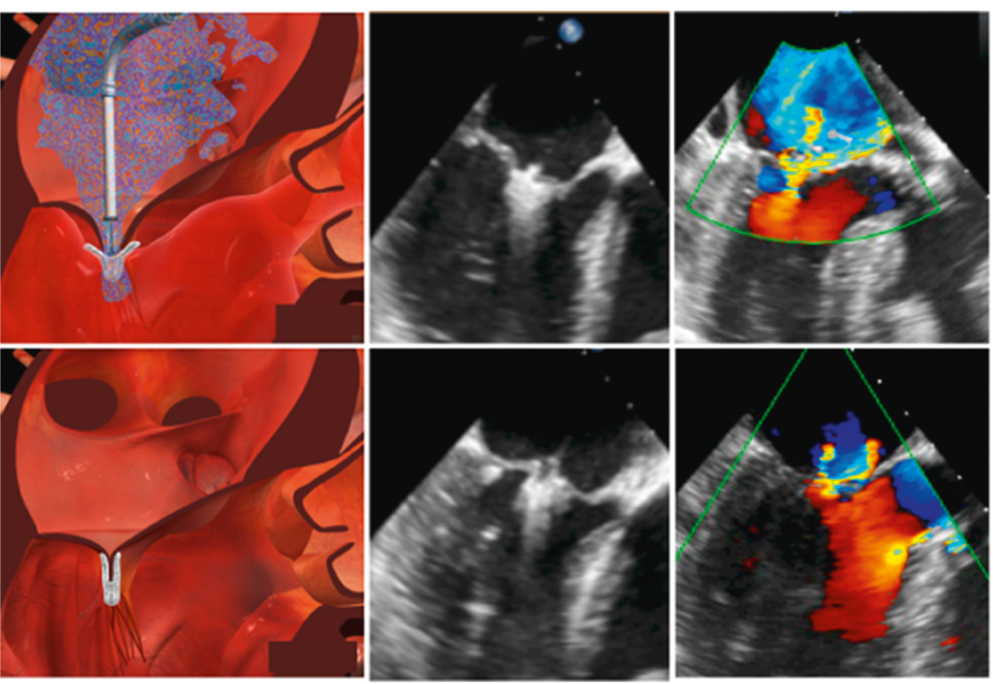
Intervention is performed in the cardiac catheterization laboratory or hybrid operating room. To allow continuous monitoring of the procedure using TEE, patients are intubated endotracheally. After puncture of the femoral vein, a steerable guiding catheter is advanced into the left atrium after transeptal puncture (Fig. 2). The guiding catheter is used to advance the carrier catheter system (clip mounted on the tip), which is also steerable, into the left ventricle through the mitral valve. As the open clip is slowly retracted, the flap sails are caught by the clip wings. When the clip is closed, the opposing mitral leaflets are fixed to each other. If the result is insufficient, the clip can be opened again, retracted and repositioned. If the result is satisfactory, the clip is detached from the catheter and left in place on the mitral valve in the heart. If necessary, several clips can be used.
Results
The first nonrandomized human trials have shown that percutaneous MKR reduces the severity of MI and improves patients’ exercise capacity and subjective well-being [3–5]. In 2011, 2-year data from the EVEREST II trial were published [6]. This randomized, controlled multicenter trial compared MitraClip technology with established surgical therapy in 279 patients with severe mitral regurgitation at moderately increased surgical risk. Although classic mitral valve surgery showed better results in terms of mitral regurgitation reduction, clip therapy was associated with better control of heart failure symptoms.
Smaller studies specifically investigated the benefit of MitraClip in patients with terminal heart failure and severe mitral regurgitation [7, 8]. In the PERMIT-CARE registry of terminally heart failure patients with severe symptoms (NYHA III/IV), the complication rate was low (30-day mortality 4.2%). 73% of patients already had an improved NYHA heart failure class at discharge, and the proportion continued to increase during follow-up. After six months, there was a decrease in left ventricular volumes and an increase in ejection fraction. Hemodynamics already improve during treatment [9]. Immediately after clip implantation, there is a significant increase in cardiac output and a decrease in pulmonary circulation pressures [9].
Treatment of mitral regurgitation using MitraClip in patients with impaired LV function has been considered in both the new ESC guidelines for the treatment of valvular heart disease and heart failure [10, 11].
Discussion
The presented technique is a novel percutaneous transvenous reconstruction technique for insufficient mitral valves. The application requires a confident use of interventional and echocardiographic techniques as well as a good anatomical knowledge of the mitral valve. As with all technically demanding procedures, a learning curve that should not be underestimated is observed, which is reflected both in the duration of the examination and in the primary result. MitraClip should therefore only be performed at centers with proven expertise in the treatment of heart failure and in surgical MKR and represents a new option for selected patients.
CONCLUSION FOR PRACTICE
- Mitral regurgitation is the most common valvular disease in general and – after aortic stenosis – the second most common in hospitalized patients.
- Surgical mitral valve reconstruction is therapy of choice for correction of mitral regurgitation of various etiologies.
- Percutaneous catheter-based treatment (using the MitraClip system) is an alternative to mitral valve surgery for patients with increased surgical risk, such as advanced age or heart failure.
- The decision whether surgical rehabilitation or MitraClip intervention should be preferred is made on a case-by-case basis in a multidisciplinary conference.
Prof. Dr. med. Roberto Corti
Literature:
- Enriquez-Sarano M, et al: Circulation 1995;91:1022-1028.
- Mirabel M, et al: Eur Heart J 2007;28:1358-1365.
- Feldman T, et al: J Am Coll Cardiol 2005;46:2134-2140.
- Pedrazzini G, et al: Cardiovascular Medicine 2010;13:122-129.
- Feldman T, et al: J Am Coll Cardiol 2009;54:686-694.
- Feldman T, et al: N Engl J Med 2011;364:1395-1406.
- Auricchio A, et al: J Am Coll Cardiol 2011;58:2183-2189.
- Franzen O, et al: Eur J Heart Fail 2011;13:569-576.
- Gaemperli O, et al: Heart 2012;98:126-132.
- Vahanian A, et al: Eur Heart J 2012.
- McMurray JJ, et al: Eur Heart J 2012;33:1787-1847.









