Prostate cancer is the most common cancer in men. Not all prostate cancers are the same (keyword risk stratification). Not every prostate carcinoma needs to be treated (keyword overtherapy). Various curative therapeutic options are available for the treatment of localized prostate carcinoma, depending on the risk profile.
In Switzerland, approximately 6100 men are diagnosed with prostate cancer each year. This makes prostate cancer the most common cancer of all. In most cases, the tumor is initially localized or organ-confined. In this case, the treating urologist has a variety of therapeutic options at his disposal. These range from active surveillance (“active surveillance”) to radical prostatectomy.
Before a decision for or against a form of therapy is made, the general condition, life expectancy, and tumor characteristics (risk stratification) should be assessed in each patient. Life expectancy plays a larger role than biological age in considering treatment modalities. With advanced patient age or reduced life expectancy, the patient’s comorbidities reduce the risk of dying from prostate cancer: Thus, patients die with prostate cancer but not from prostate cancer.
Risk stratification
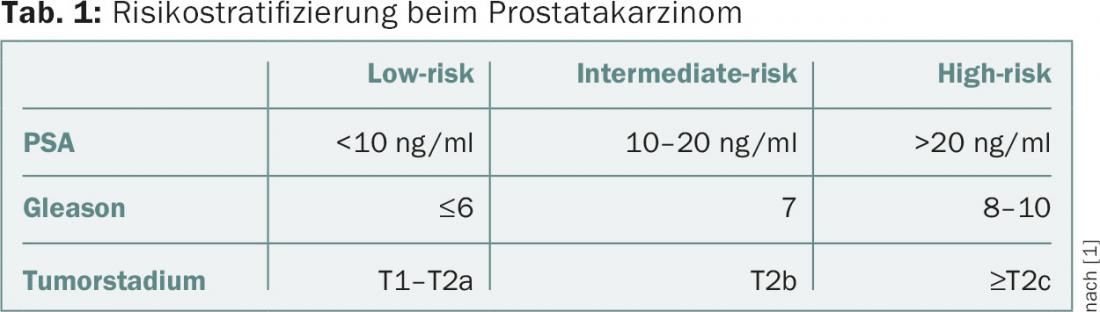
Risk stratification in prostate cancer is based on PSA level, Gleason biopsy score, and clinical stage. A common classification is according to D’Amico et al. [1]. Here, patients with localized prostate cancer are divided into three risk groups (Table 1).
Active Surveillance
The imbalance between incidence and mortality in localized prostate cancer suggests that some patients do not benefit from treatment (overtreatment). Men who do not seek immediate treatment may opt for Active Surveillance (AS) in the presence of a low-risk tumor [2]. Here, the local status and the PSA value are monitored and rebiopsies are performed according to a schedule. AS has two goals: First, to provide timely curative therapy to men with localized prostate cancer, not immediately, but in the event of progression. Second, to reduce the risks of treatment-induced complications (e.g., erectile dysfunction, incontinence) in men with low-risk carcinomas.
With good patient selection, the results are promising. The overall survival of patients in the long-term course is the same as in patients who received curative therapy directly. Approximately 25% of patients under AS will undergo curative therapy during the observation period. Arguments against the concept of AS include the sometimes high psychological burden on patients and a possible worsening of prognosis if therapy is delayed. For example, data exist indicating that patients who waited more than 180 days for therapy after diagnosis of prostate cancer had a 2.7-fold higher postoperative recurrence risk than patients who had radical prostatectomy in the first three months [3].
AS has undoubted value in the treatment of localized prostate carcinoma, but reliable predictors for confident prognosis estimation are currently lacking. Therefore, patients must be informed and educated about the respective advantages and disadvantages of AS.
Low-dose-rate brachytherapy
In low-dose-rate (LDR) brachytherapy, radioactive metal pins (seeds) are inserted into the prostate via the perineum using hollow needles under ultrasound guidance. The seeds remain in the prostate gland where they deliver the required radioactive dose. The procedure is performed under anesthesia and takes about two and a half to three hours, including all preparations, with an inpatient stay of usually only one night after the surgery.
Of great importance for brachytherapy is the selection of patients. Due to heterogeneous data, LDR brachytherapy is only a treatment option for patients with low-risk carcinoma (i.e., patients who also qualify for AS), a prostate size <50 cm3, and no relevant micturition symptoms (IPSS ≤12). Disease-free survival at five years is 71-93%, and 65-85% at ten years [4]. To date, no randomized trial has compared brachytherapy with any other curative therapy for localized prostate cancer.
External radiotherapy
External percutaneous radiotherapy (“external beam radiation therapy”, EBRT) is an alternative therapy for organ-confined prostate cancer. In retrospective comparisons, EBRT shows comparable oncologic outcomes to radical prostatectomy in well-differentiated tumors; radical prostatectomy has advantages in poorly differentiated tumors. EBRT is performed as individual image-guided irradiation (CT, MRI, PET-CT) using photons with optimal utilization of the target organ while sparing the surrounding organs at risk as much as possible. The duration of EBRT is several weeks (e.g., 78 Gy total dose with single doses of 2 Gy = 39 fractions = eight weeks of therapy).
Depending on the risk group according to D’Amico et al. patients with EBRT receive either neoadjuvant, concomitant, or adjuvant androgen deprivation therapy (ADT). Therefore, due to the hormone-dependent nature of prostate cancer, the results of EBRT are difficult to compare with the results of other curative therapeutic modalities. If recurrence occurs after primary EBRT, it is in principle treatable and curable by radical salvage prostatectomy, but the procedure is associated with a significantly increased risk of serious complications (incontinence in 56%, erectile dysfunction in 81%) [5]. It remains unclear whether and at what frequency second cancers occur after EBRT.
Radical prostatectomy
Radical prostatectomy (RP) involves removal of the entire prostate gland, including the seminal vesicles and the ampullae of the vas deferens. At treatment centers, the procedure is nowadays preferably performed in a minimally invasive robot-assisted procedure (RARP) using the da Vinci system. Recent studies report lower perioperative morbidity as well as better postoperative erectile function when using the da Vinci system compared to the open technique [6,7]. In contrast, initial long-term observations with a follow-up of ten years indicate equivalent oncologic effectiveness of robotic-assisted and open surgery [8].
Depending on the tumor characteristics and the patient’s sexual function, RP is either nerve-sparing (to preserve erectile function) or non-nerve-sparing. Simultaneous pelvic lymphadenectomy is performed with RP depending on the risk profile. Of the various curative methods for the treatment of localized prostate cancer, RP is the only one for which there is an evidence level I regarding tumor control. Another potential advantage of RP compared to EBRT is that in case of recurrence after RP, a substantial proportion of patients can be cured by additive radiation (so-called salvage radiotherapy) with acceptable morbidity (incontinence in 13%, erectile dysfunction in 61%) [5].
Other treatments
In addition to the established treatment modalities already described, a variety of other therapies exist. These include cryotherapy, high-intensity focused ultrasound (HIFU), high-dose interstitial prostate brachytherapy, and combination therapies (e.g., EBRT and interstitial prostate brachytherapy). A scientific evaluation of these procedures is still pending and therefore does not allow any clear recommendations.
Conclusion
Men with a newly diagnosed, locally limited prostate carcinoma and a high life expectancy can now be offered all established methods (EBRT, RP, LDR prostate brachytherapy or AS) depending on the risk profile. Choosing the optimal procedure for the individual patient is challenging and requires close cooperation between all disciplines involved. This can best be achieved within the framework of an interdisciplinary tumor board.
Literature:
- D’Amico AV, et al: Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998; 280(11): 969-974.
- Klotz L: Active surveillance: patient selection. Curr Opin Urol 2013; 23(3): 239-244.
- Lellig K, et al: [Active surveillance of low risk prostate cancer]. Urologist A 2014; 53(7): 1031-1039.
- Mottet N, et al: Guidelines on prostate cancer. European Association of Urology. Guidelines on prostate cancer. European Association of Urology 2015.
- van der Poel HG, et al: Sequential treatment for recurrent localized prostate cancer. Journal of Surgical Oncology 2008; 97(5): 377-382.
- Ficarra V, et al: Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol 2012; 62(3): 405-417.
- Haglind E, et al: Urinary Incontinence and Erectile Dysfunction After Robotic Versus Open Radical Prostatectomy: A Prospective, Controlled, Nonrandomised Trial. Eur Urol 2015; 68(2): 216-225.
- Diaz M, et al: Oncologic outcomes at 10 years following robotic radical prostatectomy. Eur Urol 2015; 67(6): 1168-1176.
InFo ONCOLOGY & HEMATOLOGY 2015; 3(11-12): 8-10.