
More volunteer donors and reduced-intensity conditioning now make allogeneic stem cell transplantation accessible to a larger patient population. In turn, autologous stem cell transplantation also stops autoimmune diseases via “rebooting” the immune system.
Allogeneic bone marrow transplantation turned 60 years old last year. At that time (1957), E. Donnall Thomas and colleagues obtained bone marrow cells from the ribs of adult or fetal cadavers, filtered, suspended in culture medium, frozen at -80°C, and later infused into irradiated patients. Passive growth of donor cells could be demonstrated in a proportion of patients, but all patients died within the first 100 days after transplantation. Although much has changed since then, allogeneic stem cell transplantation (allo-SCT, via transfer of bone marrow, mobilized peripheral blood, or umbilical cord blood) remains a complex, intensive, and complicated treatment today. In view of new targeted substances and immunotherapies, some experts postulate that allo-SCT has passed its zenith and will no longer be needed to cure many malignant diseases of the blood and lymphatic system in just a few years. The real numbers speak against it – still the trend of annually increasing numbers of allogeneic as well as autologous stem cell transplantations continues [1]. In this article, selected examples will be used to illustrate the developments in stem cell transplantation in recent years and to venture an outlook for the future.
Donor selection and availability
The first allogeneic bone marrow transplants took place before the discovery of human leukocyte antigens (HLA). As late as the 1960s, knowledge was essentially limited to observations that blood or leukocytes of certain patients reacted with each other and that “sensitization of the immune system” was possible. In the 1970s, R. Zinkernagel and P. Doherty discovered the basic principle of T cell activation by antigen presentation and HLA restriction. It was not until the late 1980s that the protein structure of the HLA was visualized. Today, two HLA classes are known, each with 7678 class I and 2268 class II alleles. Today, allo-SCT is performed taking into account the HLA characteristics, since it is known that so-called “mismatches” in the HLA are the strongest cause of a reverse rejection reaction (graft-versus-host disease, GVHD). In addition, it is also known – but not yet implemented in the clinic – that the expression level of certain disparate HLA allele variants may be associated with the severity of GVHD [2], and that certain disparate allele variants may simultaneously influence the likelihood of disease recurrence [3]. Consideration of such permissive “mismatches” (for GVHD or graft-versus-leukemia effects, GVL) in donor selection is quite conceivable in the future, given increasing numbers of registered donors. Currently, over 32 million stem cell donors are registered worldwide (123,471 in Switzerland as of Aug. 12, 2018 and >8 million in Germany, www.wmda.info), which means that despite decreasing family size and number of siblings, an HLA-identical unrelated donor can be found for over 70% of patients of Caucasian descent. However, for other ethnic groups, this probability is much lower [4], and individuals of mixed ethnic descent usually have low chances of successfully finding an outside donor.
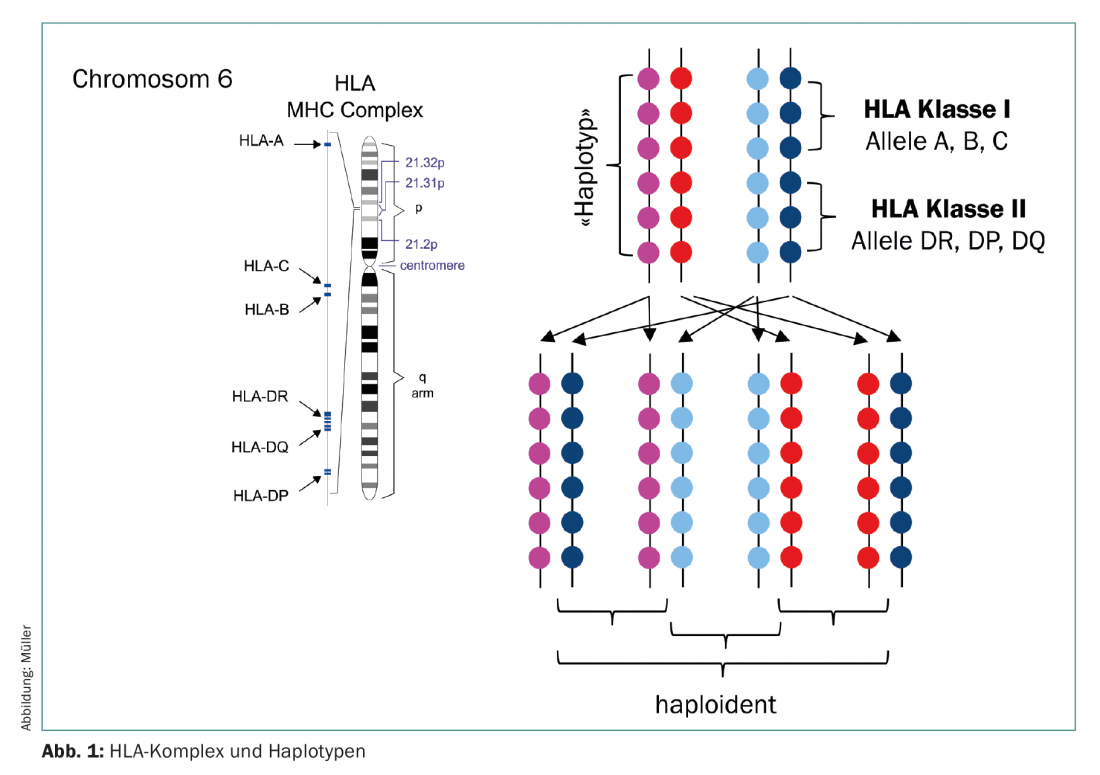
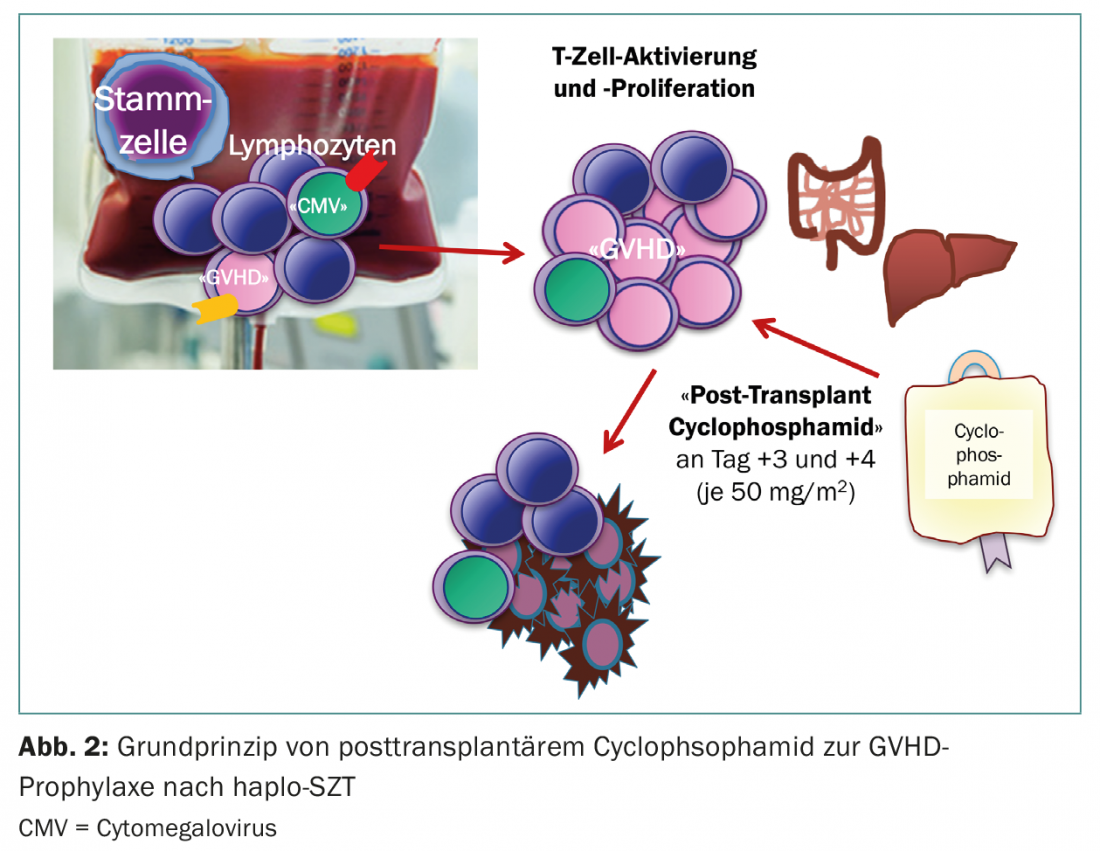
An alternative stem cell source is haploidentical (semi-matched) donors (Fig. 1) . Until a few years ago, haploidentical transplants were used with the same reluctance as umbilical cords, since both were associated with a high risk of severe complications. However, since about 2012, haplo-SZT has been gaining strong popularity as a new therapeutic maneuver has entered the clinic. The group of E. Fuchs and L. Luznik developed a conditioning regimen in which unmanipulated bone marrow from haploidentical donors with full T-cell content is infused into patients without concomitant immunosuppression. It is well known that in the first days after transplantation there is a massive proliferation and expansion of lymphocytes due to lymphopenia in the recipient (homeostatic expansion). Here, mainly activated lymphocytes proliferate, i.e. the cells that have found their target antigen on the recipient tissues and would consequently lead to acute GVHD. In this assumption, high-dose cyclophosphamide is administered on days 3 and 4 after haplo-SZT, which in turn kills lymphocytes undergoing division. Resting lymphocytes, on the other hand, are spared, as are the stem cells themselves, so that hematopoietic regeneration is unrestricted (Fig. 2) [5,6]. The success of this regimen is now proven, both in studies and in clinical practice [7,8]. With parents and children certain, and siblings 50 percent likely to be haploidentical, a donor can now be identified for nearly all patients – even for patients whose ethnicity is not adequately represented in the registry, or in countries where a costly outside donation cannot be financed.
Conditioning, side effects and mortality
There is less news in the area of conditioning and its complications. With the realization that allogeneic transplantation is an immunotherapy, and that it is not so much the conditioning chemotherapy but rather the alloreactivity of the T cells directed against the malignant cells that can achieve long-term immunological control of the underlying malignancy, the intensity of the preparatory chemotherapy was reduced (“reduced-intensity conditioning”, RIC), which significantly reduced its toxicity and mortality. As a result, allogeneic transplantation is now accessible to older patients and those with comorbidities. This is clearly reflected in the transplantation figures, since myeloid neoplasms in particular are diseases of older age. RIC conditioning has gained a permanent place in the clinic over the past 10-15 years and now accounts for about half of allogeneic SCT. The question of whether more recurrences occur after RIC than after myeloablative conditioning (MAC) has not yet been resolved for all disease entities and remains the subject of ongoing debate.
Widely used component of reduced as well as myeloablative conditioning regimens is now anti-thymocyte globulin (ATG), which serves as in vivo T-cell depletion of GVHD prophylaxis. Several studies have shown that ATG can reduce the rate of not only acute but also chronic GVHD. However, experiences regarding the probability of recurrence after SCT are contrary, which is why ATG is used more cautiously in the USA than in Europe.
Less chronic (but not acute) GVHD is associated with the use of bone marrow (BM) rather than mobilized peripheral blood as a stem cell source [9], which has been attributed to the lower T cell content of bone marrow. However, due to the significantly higher expense for donor and collection center, it currently seems unlikely that the number of KM transplants at the expense of peripheral blood stem cell transplants will gain importance in the near future.
In established GVHD, two “new” promising compounds are currently in clinical trials – first, the JAK1/2 inhibitor ruxolitinib, which can also inhibit T cell activity via STAT signaling pathways [10], and second, ibrutinib has been approved in the US for the treatment of chronic GVHD. Ibrutinib is an irreversible inhibitor (“small-molecule”) of Bruton tyrosine kinase and interleukin 2-inducible kinase (ITK). The latter kinase is significantly involved in the activation of T cells and thus in the development of alloreactivity and GVHD [11].
New cell therapy strategies against recurrences.
Overall survival after allo-SCT has improved significantly over the past two to three decades. Therapy-associated mortality has dropped significantly due to improved antimicrobial agents (mainly antifungal and antiviral). However, despite all progress, the recurrence rate after allo-SCT has not improved, ultimately leading to death in more than 25% of patients [12]. Approaches to prevent posttransplant recurrences in the future include the following considerations: The effect of allo-SCT and its superiority over high-dose chemotherapy with autologous stem cell retransfusion (auto-SCT) are based on the GVL effect. This can be long-lasting and protect against disease recurrence, but requires a certain amount of time to “establish”. Especially in aggressive leukemias, disease activity often recurs very early after allo-SCT, even before a GVL effect can occur. For this reason, strategies are being explored to provide prophylactic drug therapy continuation early after allo-SCT, e.g. with hypomethylating agents, and to combine these with donor lymphocytes, if necessary, in order to control the disease until sufficient GVL effect has set in.
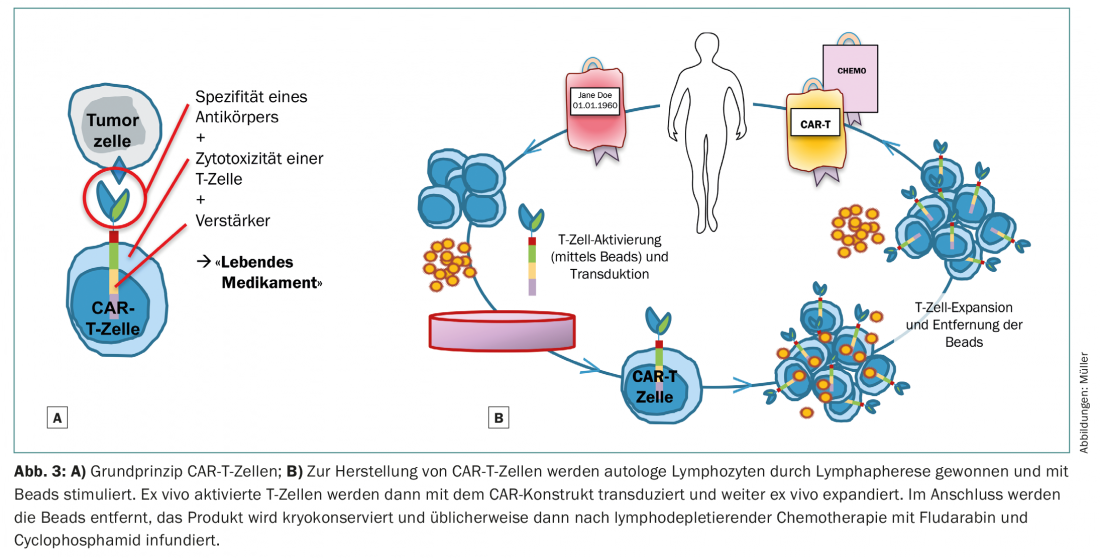
An alternative strategy to cure neoplasms immunologically or by T cell activity is the genetic manipulation of T cells into so-called chimeric antigen receptor T cells (CAR-T) (Fig. 3). For CD19-positive lymphoproliferative neoplasms, commercial CAR-T cells are already clinically available – soon also in Switzerland. Such modified CAR-T cells recognize their target antigen with the sensitivity of an antibody, independent of the MHC, and act with potentiated efficiency of a T cell [13,14]. In contrast to conventional cell transfers of fresh or in vitro expanded T cells, even small numbers of these genetically modified CAR-T cells are capable of massive immune responses. The disadvantage is that CAR-T cells can only be developed against known and “exclusive” tumor antigens or that unavoidable collateral damage to healthy cells must be tolerable. In the case of CD19-targeted CAR-T cells for aggressive lymphoma and acute B-lymphoblastic leukemia, healthy B cells are inevitably eliminated as well. The consequence is hypogammaglobulinemia, which can be substituted clinically pragmatically. The situation is more complex in the case of acute myeloid leukemia, for example. The leukemic stem cell is phenotypically not clearly distinguishable from the healthy blood stem cell. Immunotherapy directed against the leukemic stem cell thus requires modified, innovative CAR-T cells that are either safely short-lived (yet strong and selective enough to exert their effector function) or can be specifically eliminated again. Severe collateral damage to the healthy hematopoietic stem cell with prolonged aplasia is to be expected, so that such therapies may only be clinically feasible with the follow-up concept of SCT.
That CAR-T cell therapies will replace allo-SCT completely in the near future is not yet within reach. However, for a few entities such as aggressive B-cell lymphomas and possibly myelomas, it seems conceivable that CAR-T cell therapies could be superior to both autologous and allogeneic SCT.
Autolog – new on old paths
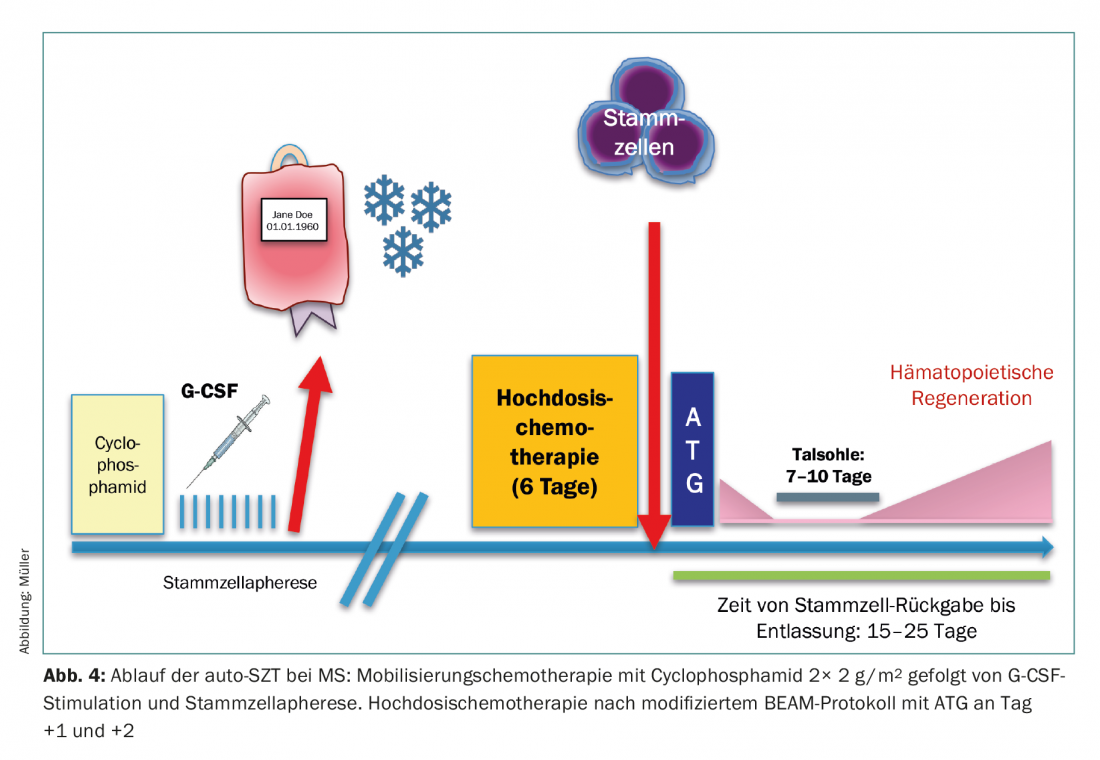
The use of auto-SCT is currently being expanded at the University Hospital Zurich in the form of a registry study for patients with multiple sclerosis (MS). Stem cell mobilization is achieved by the highly lymphodepleting cyclophosphamide, thus minimizing lymphocyte contamination of the apheresate. Following high-dose chemotherapy, further in vivo T cell depletion is performed post-transplant using ATG (days 1 and 2) to eliminate residual T cells. After complete eradication of hematopoietic and lymphatic system, the “restart” occurs starting from the hematopoietic stem cell (Fig.4). Biological data on the efficacy of this principle are available in the form of many well-founded observations in preclinical models, but also in phase II clinical trials, which have been able to show that this therapeutic maneuver can bring the progression of MS to a complete halt in many cases [15,16].
Will classical stem cell transplantation become a redundant form of treatment in the near future? Certainly not at present – but it is to be hoped that the field will move in the direction of innovative, tailored cell therapies that have fewer or better controllable, shorter-lasting side effects and attack tumor cells more efficiently instead of healthy tissue.
Take-Home Messages
- Despite new targeted substances and immunotherapies, the numbers of stem cell transplants performed each year continue to rise steadily.
- Increasing numbers of registered volunteer donors and reduced-intensity conditioning regimens now allow access to allogeneic stem cell transplantation for a significantly larger patient population.
- Recurrences after allogeneic stem cell transplantation remain the leading cause of death and require new strategies for recurrence prophylaxis and enhancement of graft-versus-leukemia effects.
- Chimeric antigen receptor T cells are the most advanced form of cell therapy, but are currently in clinical use for only a few disease entities.
- Autologous stem cell transplants are not only used in the treatment of malignant hematologic diseases, but
- can also stop the course of autoimmune diseases by restarting the immune system.
Literature:
- Passweg JR, et al: Is the use of unrelated donor transplantation leveling off in Europe? The 2016 European Society for Blood and Marrow Transplant activity survey report. Bone Marrow Transplant 2018. DOI: 10.1038/s41409-018-0153-1 [Epub ahead of print].
- Petersdorf EW, et al: High HLA-DP expression and graft-versus-host disease. N Engl J Med 2015; 373(7): 599-609.
- Venstrom JM, et al: HLA-C-dependent prevention of leukemia relapse by donor activating KIR2DS1. N Engl J Med 2012; 367(9): 805-816.
- Gragert L, et al: HLA match likelihoods for hematopoietic stem-cell grafts in the U.S. registry. N Engl J Med 2014; 371(4): 339-348.
- Robinson TM, et al: Haploidentical bone marrow and stem cell transplantation: experience with post-transplant cyclophosphamide. Semin Hematol 2016; 53(2): 90-97.
- Luznik L, O’Donnell PV, Fuchs EJ: Post-transplant cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation. Semin Oncol 2012; 39(6): 683-693.
- McCurdy SR, et al: Comparable composite endpoints after HLA-matched and HLA-haploidentical transplantation with post-transplant cyclophosphamide. Haematologica 2017; 102(2): 391-400.
- Kasamon YL, et al: Prospective study of nonmyeloablative, HLA-mismatched unrelated BMT with high-dose posttransplant cyclophosphamide. Blood Adv 2017; 1(4): 288-292.
- Anasetti C, et al: Peripheral-blood stem cells versus bone marrow from unrelated donors. N Engl J Med 2012; 367(16): 1487-1496.
- Zeiser R, et al: Ruxolitinib in corticosteroid-refractory graft-versus-host disease after allogeneic stem cell transplantation: a multicenter survey. Leukemia 2015; 29(10): 2062-2068.
- Miklos D, et al: Ibrutinib for chronic graft-versus-host disease after failure of prior therapy. Blood 2017; 130(21): 2243-2250.
- Appelbaum FR: Improved outcomes with allogeneic hematopoietic cell transplantation. Best Pract Res Clin Haematol 2012; 25(4): 465-471.
- Dai H, et al: Chimeric Antigen Receptors Modified T-Cells for Cancer Therapy. J Natl Cancer Inst 2016; 108(7).
- Curran KJ, Pegram HJ, Brentjens RJ: Chimeric antigen receptors for T cell immunotherapy: current understanding and future directions. J Gene Med 2012; 14(6): 405-415.
- Muraro PA, et al: Long-term Outcomes After Autologous Hematopoietic Stem Cell Transplantation for Multiple Sclerosis. JAMA Neurol 2017; 74(4): 459-469.
- Mancardi GL, et al: Autologous hematopoietic stem cell transplantation in multiple sclerosis: a phase II trial. Neurology 2015; 84(10): 981-988.
InFo ONCOLOGY & HEMATOLOGY 2018; 6(5): 26-30.









