
In order to assess the appropriate use of folic acid as a supplement or its fortification in foods, it is necessary to know the biological importance, the supply of the population and the health, i.e. preventive, benefits of this vitamin. These aspects will be highlighted in the following article.
According to today’s definition, folic acid is the synthetic form of the vitamin known as folate. The name derives from the lat. “folium” (=leaf), as it was first isolated from spinach. Naturally occurring folate compounds (= folates) are found in animal and plant foods. Especially leafy vegetables have a high content. Good sources of folate are spinach, lettuce, broccoli, white cabbage, beans, tomatoes, oranges, liver, and cereals [1].
The synthetically produced folic acid used for dietary supplementation and in pharmaceuticals contains only a glutamic acid residue (PGA). It is the most stable form with the highest oxidation state of all folate-active compounds [1]. It is almost completely absorbed as a pure substance on an empty stomach.
Folates in solution are sensitive to light, oxygen and heat and break down into various degradation products. Therefore, considerable storage and preparation losses are to be expected [2]. Folic acid, on the other hand, is the stable form that is little affected by external influences. Due to the different composition and absorption of natural folates and synthetic folic acid, the term folate equivalent was introduced for practical intake calculation: 1 folate equivalent (FE) = 1 µg dietary folate = 0.5 µg synthetic folic acid = 0.6 µg folic acid added to food (fortification).
In the human organism, tetrahydrofolate (THF), the active folate compound, occurs as 5-methyl-THF, 5,10-methylene-THF, 5,10-methenyl-THF, and 5-formyl-THF. In serum/plasma, 5-methyl-THF monoglutamate is mainly present, and polyglutamyl-THF is present intracellularly [3]. This shows that dietary folates are subject to various, rather complex transport and metabolic processes and regulations in the organism and their effects are therefore not yet clarified in all details [4].
Biological function
Folates enable the transfer of CH3(C1) or methyl groups in various metabolic reactions and thus play a key role in cell division and cell renewal [3]. Folate deficiency manifests itself mainly in cell systems with high division rate, i.e. blood cells and mucosal cells. Therefore, the first signs of deficiency are anemia with blood cell changes and mucosal inflammation (glossitis).
Needs, supply and recommendations
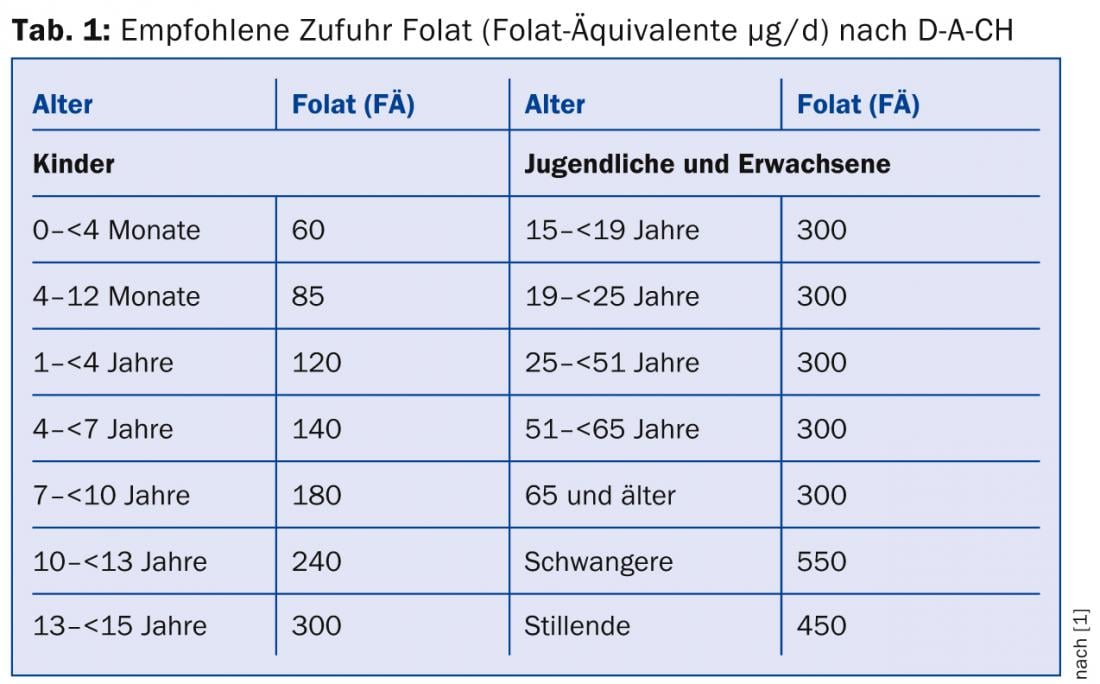
The minimum amount of folate necessary for the maturation of blood cell precursors and thus for the prevention of anemia is 50(-100) µg/d. In the Swiss Nutrition Ordinance, the legal value for the folic acid/folacin daily requirement is given as 200 µg, which corresponds to about 400 µg FÄ according to the D-A-CH reference values of 2000. At that time, this value was determined because with this daily dose the homocysteine value (at that time an important factor for cardiovascular risk) could be stabilized in the upper normal range (10-12 µmol/L). Today, however, less importance is attached to homocysteine, so that the new D-A-CH recommendation as of August 2013 for adults is 300 µg FÄ [1]. The age-dependent recommendations in force today can be seen in Table 1.
The new recommendations are based on literature data from recent years and, above all, studies in Germany and Austria on the folate supply of the population and their folate status, i.e. the determinations of folic acid in serum/plasma and erythrocytes [1]. In Switzerland, we do not know of any such general surveys of dietary folate intake and folate status except in a few small groups. In our country, folate consumption is calculated based on the total consumption of various foods and their folate content and is reported as 284 and 295 µg/d per person in the fifth (2001/02) and sixth (2007/08) Swiss Nutrition Reports [6, 7]. In many cases, an undersupply of folate is emphasized [2, 5].
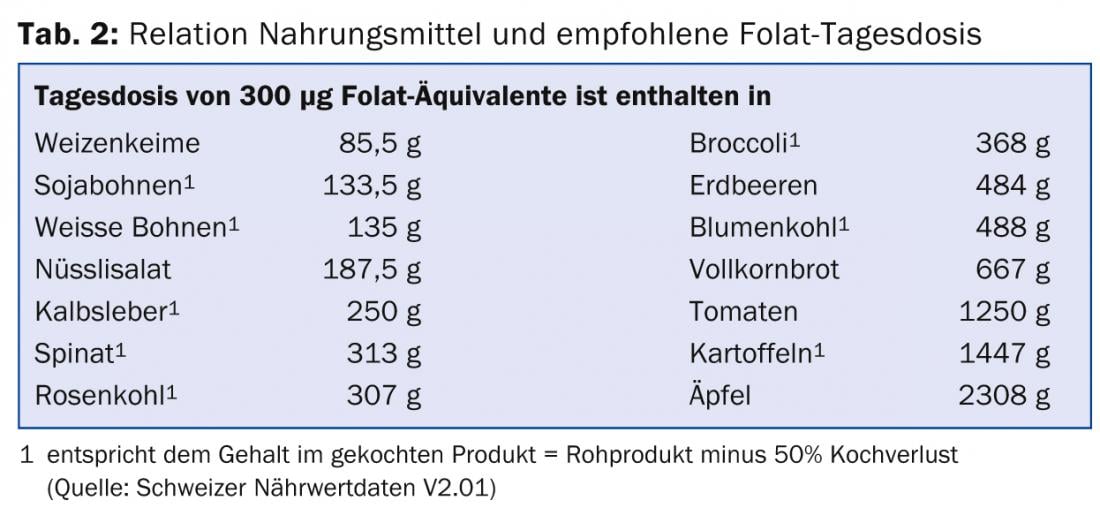
It has also been calculated that it is difficult to meet the daily requirement of folate with a healthy diet, especially when the requirement is increased, as in pregnancy or lactation [1]. Several factors can increase the need for FS, such as smoking, chronic alcohol consumption, and medications such as FS antagonists, antiepileptic drugs (e.g., phenytoin) [5]. Table 2 shows how much of individual foods must be taken to meet the requirement of 300 µg FS [5].
The surveys in Germany and Austria showed daily FÄ intakes in the range of 190-255 µg/d, and yet normal to highly normal serum/plasma and erythrocyte folate levels were measured in adults, and even higher in adolescents. Based on these facts, the new D-A-CH reference values for adults were lowered to 300 µg FÄ/d [1].
Health aspects of folic acid
Folate/folic acid has numerous preventive effects. These resulted primarily from epidemiologic studies that evaluated specific endpoints in comparison with the level of folate intake. Comparative studies of disease prevalences before and after fortification of flour with folic acid (now mandatory in 75 countries worldwide) also contributed [8]. In the EU and Switzerland, the following health claims are permitted for FS-enriched foods that meet the minimum requirements (>15% of the daily requirement per 100 g, 100 ml or serving), approved: Folate contributes “to the growth of maternal tissues during pregnancy” , “to normal amino acid synthesis”, “to normal hematopoiesis”, “to normal homocysteine metabolism”, “to normal mental function”, “to normal immune system function”, “to reduction of fatigue and tiredness” and “has a function in cell division” [9]. In Switzerland, the additional claim: “Folate is needed for the development of the neural tube of the unborn child.” is permitted.
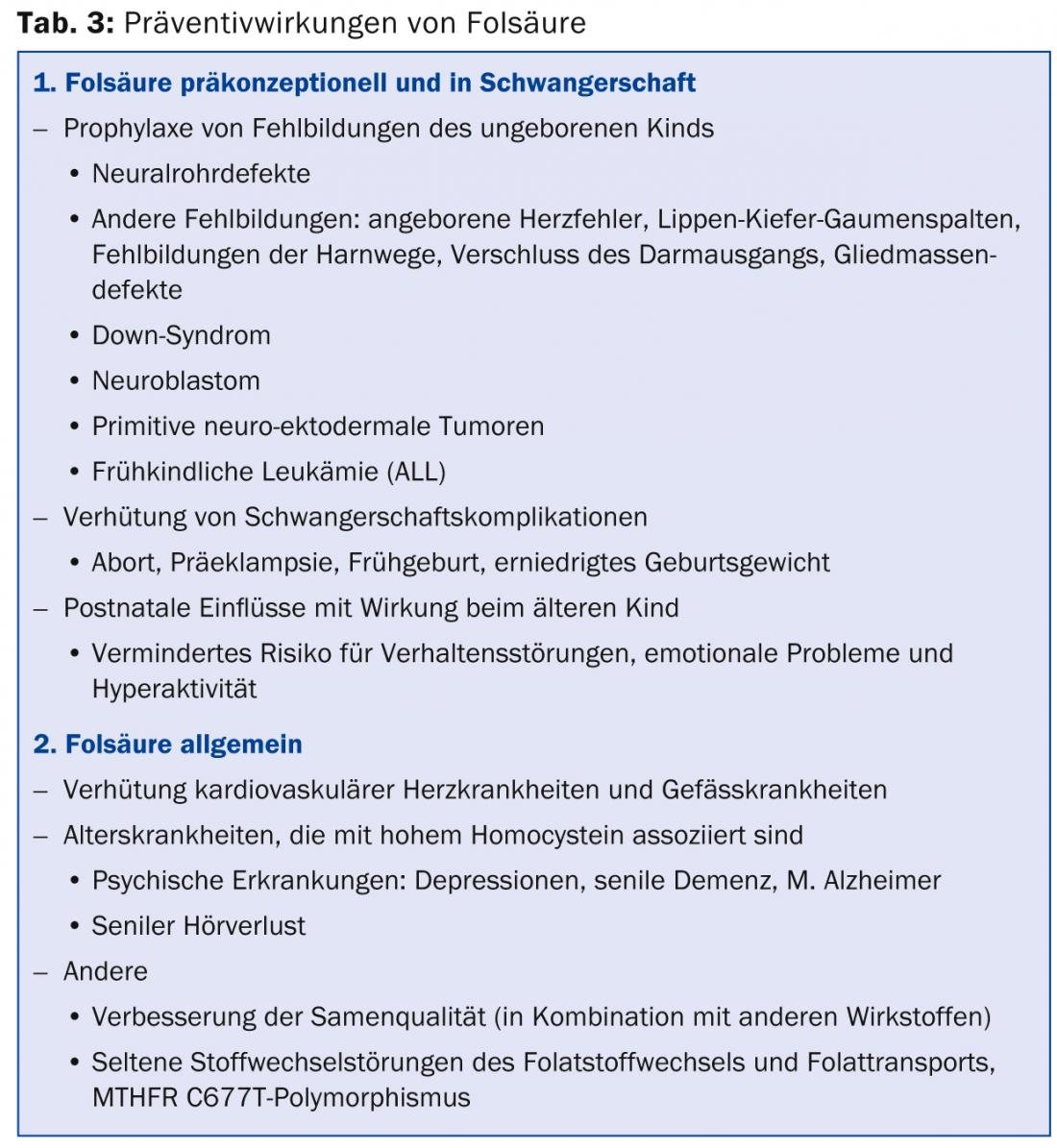
Table 3 summarizes the preventive effects of folic acid, following Tönz [10].
Folic acid preconception and during pregnancy
In the prophylaxis of malformations of the unborn child, the neural tube defects (NRD) are in the foreground. NRDs are early embryonic developmental disorders that occur between days 18 and 28 after conception. If closure of the neural tube does not occur during this time, vertebral arches (and skullcap) also remain open without skin covering (open back = spina bifida, myelomeningocele). Despite early treatment, children usually remain motor and sensory paralyzed. In the cranial defect, anencephaly occurs, which is usually lethal. The incidence of NRD is variable, ranging from 5-6‰ to 0.8‰. In Switzerland, it is slightly less than 1‰ [10, 11].
In several intervention studies, folic acid supplementation early in pregnancy reduced the relative risk of NRD by 40-100%. Today, 75 countries worldwide fortify flour with folic acid, achieving an average reduction in NRD of 47% [8].
In the Hungary study, in which the intervention was performed with a multivitamin containing folic acid (800 µg), it was noticed that other malformations (cleft lip and palate, congenital heart defect, urinary tract malformations, intestinal outlet obstruction, and limb defects) were also reduced by half, as mentioned in Table 3 [2, 10]. However, it is difficult to provide unequivocal evidence that the malformations are preventable by folic acid alone when a multivitamin is taken. But the causality of the association folic acid and embryonic malformations is confirmed by the observation that folic acid antagonists taken during early pregnancy lead to the same malformation patterns (four to seven times higher risk than in control group) as can be prevented by supplements of folic acid alone or as a multivitamin [10].
In cleft lip and palate, only orofacial clefts respond to FS (reduction of 40-60%), but not isolated cleft palate (different embryogenesis). In congenital heart defects, success has been seen primarily in conotruncal malformations (tetralogy of Fallot) and septal defects. This is because septation of the great vessels (aorta/pulmonary artery) and creation of the septum primum occur from neural crest tissue, suggesting a dependence on FS [4, 10]. The formation of the urinary tract occurs somewhat later in embryogenesis than that of the neural tube and heart, which is why the intake of folic acid is important until the end of the third month of pregnancy. The reduction rate here is quite high (up to 80%), although embryologically there is no connection with the neural plate. Limb defects are rather rare, but could be reduced by FS by about 35% [4, 10].
Elevated homocysteine levels have been found in mothers of children with Down syndrome. Similarly, women with certain gene variants in FS metabolism (e.g., MTHFR C677T) have a slightly increased risk of giving birth to a child with Down syndrome. In children with Down syndrome, congenital heart defects are 40 times more common and early childhood leukemias are 20 times more common than in children with a normal set of chromosomes [10]. These findings suggest a relationship with folic acid. Hypomethylation of DNA in the centromeric region promotes non-disjunction, which can lead to trisomy 21 [2]. However, this effect has not yet been statistically proven. The reason is that chromosomal non-disjunction occurs in two-thirds of cases in meiosis 1, i.e. towards the end of the maternal fetal period, so that success can only be expected in about 30-35 years [10].
The use of folic acid has shown in recent years that individual early childhood malignancies have also become less frequent. Malignant neuroblastoma arising from the sympathetic or adrenal medulla and primitive neuroectodermal tumors of the brain both arise from embryonic nervous tissue. Since flour enrichment in America, the incidence of neuroblastoma has decreased from 1.57/10,000 to 0.62 and neuroectodermal tumors have been reduced by half [10]. It was first observed in Australia in 2001 that children of mothers who received folic acid during pregnancy were 60% less likely to develop acute lymphoblastic leukemia. In children with Down syndrome, the leukemia rate was reduced by 27% [10].
Folic acid deficiency can also lead to pregnancy complications. Several studies indicate the association of low folic acid status with abortions, preeclampsia, abruptio placentae as well as fetal growth retardation. Such placenta-related complications have also been observed with the use of folic acid antagonists. Folic acid is thought to regulate trophoblast invasion [4]. Recent strudies show that FS can prevent 60% of abortions [12] and reduce the risk of preterm birth by 16% [13]. According to a Dutch study, infants of mothers who did not take folic acid supplements in the first trimester of pregnancy had a 44% higher risk of behavioral problems, and a second study also found a higher risk of emotional problems [4]. Low maternal plasma folic acid levels in early pregnancy were associated with increased rates of hyperactivity, inattention, and group behavior problems in children in an English study (observation period approaching 9 years) [4].
Folic acid in general
Whereas low serum folate with elevated homocysteine used to be quite prominent as a risk factor for cardiovascular disease, larger clinical intervention trials with B vitamins (including folate) showed no positive results for secondary prevention of cardiovascular disease, except for a reduction in stroke. However, there is a significant increase in the risk of coronary heart disease, cerebrovascular disease, and also peripheral occlusive disease at higher homocysteine levels [14]. However, the reduction of homocysteine did not yield any preventive effects. Homocysteine is thus a marker for cardiovascular disease, but not the cause. Routine screening for homocysteine and treatment of elevated homocysteine levels with folic acid for prevention can therefore not be recommended [14].
The influence of folic acid on the prevention of cancer is controversial. On the one hand, folic acid can stabilize DNA and thus prevent or limit tumorogenic transformations, but on the other hand, in an already existing early stage of a cancer, it can promote its proliferation and growth. Several epidemiological studies have primarily shown an inverse, or preventive, association between folate status and risk of colorectal, pancreatic, breast, prostate, and other malignancies [15].
As a result of the enrichment of flour with FS, a temporary increase in colorectal tumors and prostate Ca was seen in America and Canada. This has led to critical questions about flour fortification with FS. Intervention studies for cardiovascular disease with relatively high folic acid doses (average 2.5 mg/d) also found isolated evidence for increased tumor growth. However, a recent meta-analysis failed to show an association between folic acid supplementation and the incidence of colon, prostate, lung, breast, and other organ-specific cancers during the first five years of observation [16]. Flour fortification with FS and the recommended daily dose of FÄ are much lower than used in these studies. In the context of epigenetic modification of DNA by methyl groups, many unanswered questions remain about how FS can influence disease prevention, both positively and negatively [16].
Some diseases of aging are associated with elevated homocysteine, which may argue for their prevention with folates. Thus, epidemiological studies have pointed out the relationship between folate supply and cognitive impairments in old age such as senile dementia, Alzheimer’s disease, and depressive disorders [2, 10]. The risk for these diseases is twice as high with high homocysteine as with low homocysteine. In an American study, a daily FS supplement resulted in a 50 percent reduction in risk. In another study, 800 µg FS/d significantly improved cognitive functions (memory and speed of information processing). Age-related hearing loss was also favorably affected in this study. There was a significant association with low folate levels in melancholic depression [2].
Recent work also suggests links of methyl (C1) metabolism with spermiogenesis and male infertility [17]. Studies in young men have shown that sperm quality has deteriorated in recent years. According to an American study, an undersupply of folate has a negative influence on sperm count and chromosome fragility. With targeted FS therapy in combination with zinc, these changes could be reduced by up to 30% [18]. In a comparative study, a Viennese research group treated 132 subfertile men for three months with two capsules of a mixture of folic acid, zinc, L-carnitine, L-arginine, vitamin E, glutathione, selenium, and coenzyme Q 10 (sold as PROFERTIL in Austria) and compared them with a group of 73 subfertile men without treatment. Results were measured by standardized sperm analysis, sperm density, ejaculate volume, sperm motility, and morphology. Findings improved by 23-83%, and during a six-month observation period, 34 pregnancies were reported in the treatment group versus 11 in the control group [19].
In the area of folate/folic acid metabolism and transport, rare disorders are known to result in folate deficiency or insufficient formation of 5-methyltetrahydrofolate (5-MTHF) and its transport into or within cells. FS cannot have a preventive effect for these disorders because they occur early. They show the full picture of extreme deficiency of FS, but are treatable with appropriate folate preparations such as folinic acid (leucovorin, citrovorum factor or formyl-THF) or metafolin (5-methylTHF) [20]. Hereditary folic acid malabsorption is well known and can lead to megaloblastic anemia, failure to thrive, immunodeficiency, neurological symptoms, and intellectual disability. Cerebral folic acid transport deficiency (FOLR1 deficiency) affects the folate receptor, results in decreased folate in CSF (serum level normal), begins in early childhood with progressive movement disorder, epilepsy, and hypomyelination. Dihydrofolate reductase deficiency (DHFR gene) may result in normal serum folate but not 5-MTHF and thus decreased CSF folate and the neurological symptoms already described above with megaloblastic anemia and pancytopenia [20].
Methylenetetrahydrofolate reductase deficiency (MTHFR deficiency) also results in a severe early childhood clinical picture. This gene is known to have a polymorphism (MTHFR-C677T) that is associated with increased folate requirements and leads to mild elevation of homocysteine [20]. It is also a risk factor for NRD. Therefore, in the prevention of NRD in pregnancy, the preparation Femibion is also recommended, which, in addition to folic acid, contains metafolin (the active form = 5-methyltetrahydrofolate, bypasses the polymorphism). Although this product is manufactured in Switzerland, it is only available abroad for the time being.
Dangers of fortification with folic acid or supplements
Although high doses of FS (≥15 mg/day) showed no direct toxic effects [15], concerns have been expressed in the context of food fortification with FS. A high intake of FS masks vitamin B12 deficiency anemia because FS corrects the typical blood changes and thus also – because of the missed diagnosis – reinforces the neurological picture of B12 deficiency. Therefore, the upper limit (“upper level”) of daily intake was set at 1000 µg (1 mg), below which this effect does not exist. Other unproven concerns include promotion of cancer (see above) and also possible epigenetic changes. At a dose of >200 µg FS, unmetabolized (free) FS may be found in the blood, the significance of which is still unclear. In any case, no definite negative health consequences have been found so far [15].
Conclusions
The effects of folic acid and its success in preventing numerous diseases make it clear that an optimal intake of this vitamin should be ensured. Unfortunately, numerous surveys at home and abroad show that FS provision is inadequate in part of the population [2 ,5]. Therefore, it is not surprising if some people, about 30-40%, take supplements with FS [21, 22].
The simplest and cheapest way to improve FS supply to the population is to fortify baking flour with FS. This would serve the entire population, especially the socially less advantaged populations who are most at risk for folate deficiency. Fortification with FS and vitamin B12 was proposed in 2002 by a group of experts from the Swiss Federal Nutrition Commission [11], but was rejected as a coercive measure by consumer organizations, among others. It is also not possible at present for legal reasons. Perhaps a renewed parliamentary interpellation can change this for the future [23].
CONCLUSION FOR PRACTICE
- Consumption of a balanced diet rich in folate through plenty of fresh vegetables and fruits as well as whole grain products
- Possible supplementation of this healthy diet with special FS-enriched foods (nutritional supplementation).
- In certain situations, additional intake of supplements (200-400 µg FS), to maintain optimal supply.
- For women who can or want to become pregnant, daily supplementation of 400-600 µg FS (preferably in the form of a multivitamin) is min. essential four weeks before the start of pregnancy and in the first twelve weeks of pregnancy to prevent neural tube defects and other malformations.
Literature:
- D-A-CH: German Nutrition Society, Austrian Nutrition Society, Swiss Nutrition Society. Reference values for nutrient intake: folate . Umschau/Braus-Verlag Frankfurt. 1st ed, 5th rev. ed. 2013; 127-152.
- Koletzko B, Pietrzik K: for the Working Group Folic Acid and Health: health significance of folic acid intake. Ernährungs-Umschau 2004, 51: 264-271.
- Moser U, Eichholzer M: Folic acid – an overview of the state of knowledge. SZE 2012; 10: 6-8.
- Bärlocher K: Folic acid periconceptional and in pregnancy. SZE 2012; 10: 9-14.
- Eichholzer M, et. al.: Folic acid is indispensable for normal child development. Bern: Federal Office of Public Health (FOPH), 2008.
- Eichholzer M, et al. (eds): Fifth Swiss Nutrition Report. Bern: Federal Office of Public Health 2005; 32.
- Keller U, et al: Sixth Swiss Nutrition Report. Bern: Federal Office of Public Health 2012; 90-91.
- Handforth B: 17 years of Fortifying with Folic Acid. Presentation on 23.Sept. 2013, personal communication.
- EU Regulation 432/2012 of May 16, 2013 on health claims for folate.
- Tönz O: Folic acid- a broad-spectrum prophylactic. Ars Medici 2008; 8: 25-30.
- Baerlocher K, et al: Measures for the prophylaxis of neural tube defects and the improvement of folic acid supply in Switzerland. Report of the Working Group “Folic Acid Prophylaxis” of the Federal Nutrition Commission, Federal Office of Public Health Bern 2002.
- Byrne J: Periconceptional folic acid prevents miscarriage in Irish families with neural tube defects. Ir J Med Sci 2011; 18: 59-62.
- Catov JM, et al: Perconceptional mutivitaminuse and risk of preterm or small for gestational-age births in the Danish <nastional Birth Cohort. Am J Clin Nutr 2011; 94: 906-912.
- Riesen WF: Homocysteine – cardiovascular and cerebrovascular risk factor or risk marker? SZE 2012; 10: 15-18.
- Crider KS, et al: Folic Acid Food Fortification – Its History, Effect, Concerns, and Future Directions. Nutrients 2011; 3(3): 370-384.
- Vollset SE, et al: Effects od folic acid supplentation on overall and site-specific cancer incidence during randomized trials: meta-analyses of data on 50 000 individuals. Lancet 2013; 381: 1029-1036.
- Singh K, Jaiswal D: One-carbon metabolism, spermatogenesis, and male infertility, Reproductive Sciences 2013; 20: 622-630.
- Malberg K, et al: The association of folate, zinc and antioxidant intake with sperm aneuploidy in healthy non – smoking men. Hum Reprod 2008; Doi: 10.1093/humrep/deno 36
- Imhof M, et al: Micronutrient Suplementation increases Sperm Quality in the sub-fertile Male. E-SPEN, the European e-Journal of Clinical Nutrition an Metabolism, doi:10.1016/j.e lnm 2011.11.002
- Zschokke J, Hofmann GF: Vademecum Metabolicum. Diagnosis and therapy of hereditary metabolic diseases. 4 edition, Schattauer Verlag 2012; 157/58.
- Beer-Borst S, et al.: The importance of functional foods in the diet of the adult population of Geneva – a review. In: Eichholzer M, et al.(eds.): Fünfter Schweizerischer Ernährungsbercht. Bern; Federal Office of Public Health 2005; 751-766.
- Max Rubner Institute, Federal Research Institute of Nutrition and Food: Often too well supplied by dietary supplements. www.mri.bund.de.
- Maury Pasquier L, personal communication via SFO.
HAUSARZT PRAXIS 2014; 9(1): 28-34









