Type 2 diabetes mellitus is a common disease in elderly patients with increasing prevalence. In addition to aspects typical of diabetes, specific geriatric syndromes such as dementia or increased risk of falls are often present. The main principles of diabetes therapy to be considered in elderly patients are: Avoidance of hypoglycemia; individual determination of HbA.1ctarget range; selection of antidiabetic drugs according to the expected blood glucose-lowering effect, side effect profile and adjustment of the drug dose in renal insufficiency; “start low and go slow!”. Insulin therapy is often started too late, but can improve quality of life to a decisive extent and has an anabolic effect.
Type 2 diabetes mellitus is a common disease in the elderly. With increasing age, the risk of developing diabetes increases – in conjunction with risk factors that are also increasing, such as obesity, malnutrition and lack of exercise. Longer life expectancy will lead to a further increase in diabetes sufferers in this age segment in the coming decades. Up to 15% of people over the age of 60 already have diabetes mellitus.
In addition to controlling the metabolic state, avoiding hypoglycemia, and treating secondary complications, treatment must also take into account the geriatric syndromes that are often present, such as dementia, risk of falls, incontinence, and depression. It should be noted that most diabetes intervention studies focus primarily on younger patients. According to a recent compilation, just 0.6% of these studies specifically examined older patient populations, almost one-third excluded patients older than 65 years, and almost all did not include individuals older than 75 years [1]. In addition, long-term data are not yet available for most of the newer preparations. This puts the influence of evidence-based guidelines into perspective [2,3], but also emphasizes the importance of the individualized approach to therapy. This article is therefore intended to provide an up-to-date and practice-oriented overview of treatment in this diverse group of patients frequently encountered in clinical practice.
Changes in carbohydrate metabolism in old age
With age, functional beta cell mass decreases, associated with a decrease in glucose-stimulated insulin secretion and a decreased beta cell response to endogenous incretins (GLP-1 and GIP). In addition, the already existing insulin resistance usually worsens. This is caused by an increase in (visceral) fat mass due to reduced physical activity and a decrease in insulin sensitivity due to medication (e.g. glucocorticoids). Muscle tissue, which along with liver and adipose tissue is one of the three main target organs in carbohydrate metabolism, is increasingly becoming the focus of age-related changes in patients with diabetes. The excessive, multifactorial decrease in muscle mass or strength (sarcopenia) in the elderly plays a central role in the complex homeostasis between insulin action and glucose metabolism and represents another cause of increasing insulin resistance in the elderly [4].
Special aspects in elderly patients with diabetes mellitus
A variety of geriatric syndromes are clustered in elderly patients with diabetes mellitus and have a negative impact on metabolic control, functional status, quality of life, and mortality. For example, cognitive impairment and dementia-related syndromes significantly worsen diabetes self-management, increase the risk of hypoglycemia, and thus make good metabolic control more difficult. Depression is significantly more common in elderly diabetics, but is often not recognized or adequately treated, and has an impact on diabetes control, in addition to effects on cognitive abilities.
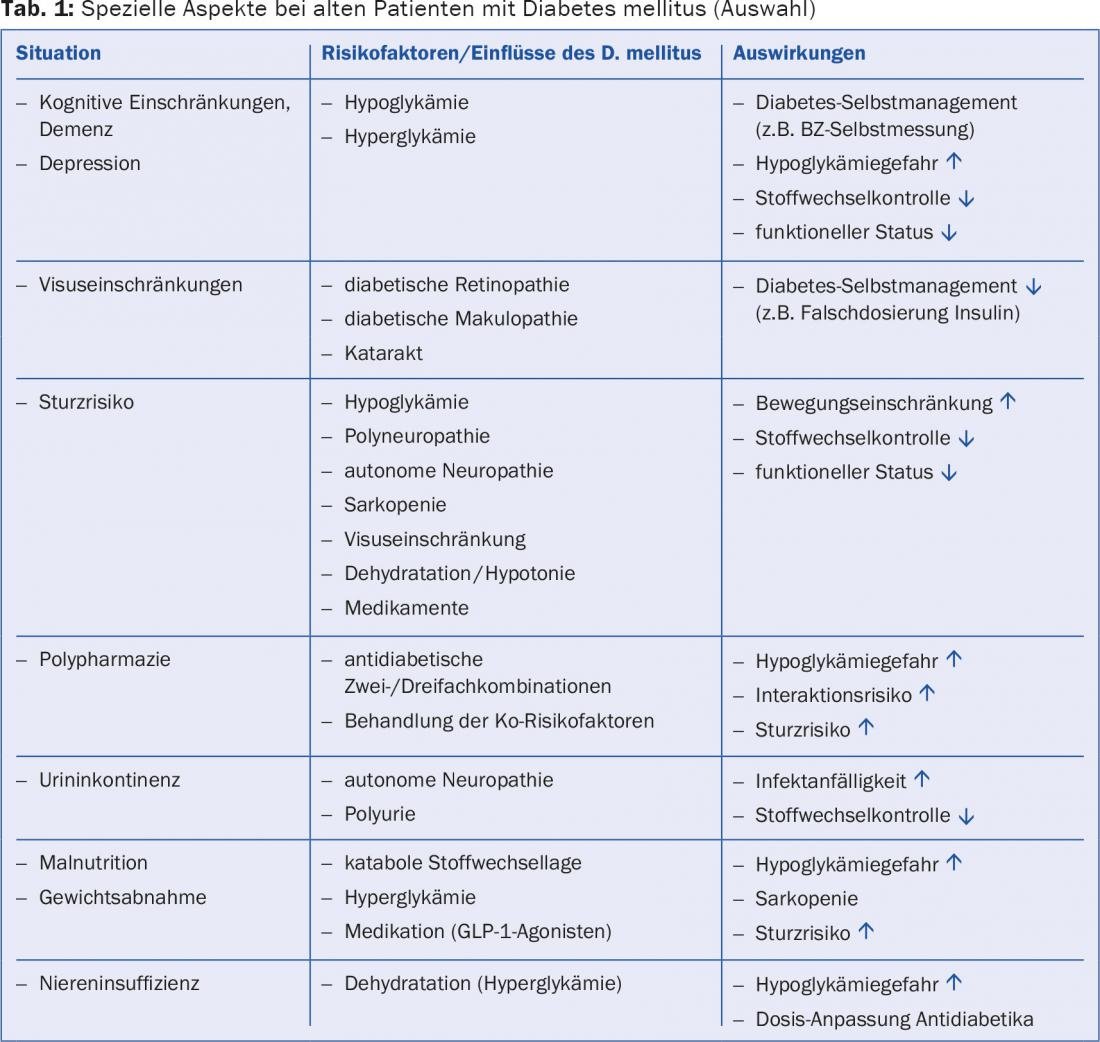
In addition to specific geriatric aspects, great attention must be paid to age- or comorbidity-related limitations in renal, hepatic, and cardiac function. This is particularly important in the selection and dosing of antidiabetic drugs and with regard to interactions with other drugs, since pharmacodynamic and pharmacokinetic parameters also change as a result. It should also be noted that the creatinine value, but also the GFR estimated with a formula (eGFR) per se, may inaccurately represent renal function in elderly patients and thus the degree of renal function impairment is often underestimated. Table 1 provides an overview of the special aspects of managing elderly patients with diabetes mellitus.
Treatment
The four main principles in the management of diabetes mellitus in elderly patients are:
- Avoiding hypoglycemia
- individual determination of the HbA1c target range
- Selection of antidiabetic drugs according to expected blood glucose-lowering effect, side effect profile, and adjustment of drug dose in renal insufficiency.
- Start low and go slow!
Avoiding hypoglycemia (Fig. 1): The risk of hypoglycemia increases with increasing duration of diabetes. Often, elderly patients are insufficiently aware of adrenergic hypoglycemic symptoms. Neuroglycopenic symptoms are not infrequently interpreted as symptoms of dementia or cerebral circulatory disorder, thus significantly underestimating the true prevalence of hypoglycemia in everyday life in these patients. Recurrent severe hypoglycemia is an important risk factor for dementia [5]. They lead to falls, increase the risk of fractures, and cause increased hospitalizations [6]. Any hypoglycemia activates the sympathoadrenal system and thus can trigger arrhythmias and increase blood pressure, which increases cardiovascular morbidity and mortality. Hypoglycemia can be reduced, on the one hand, by avoiding the appropriate risk factors that predispose the patient to hypoglycemia and, on the other hand, by choosing the appropriate therapeutic agents. The increasing number of new antidiabetic drugs (incretin-based therapeutics and SGLT-2 inhibitors) is a valuable addition, as these drugs do not have an intrinsic hypoglycemic risk.

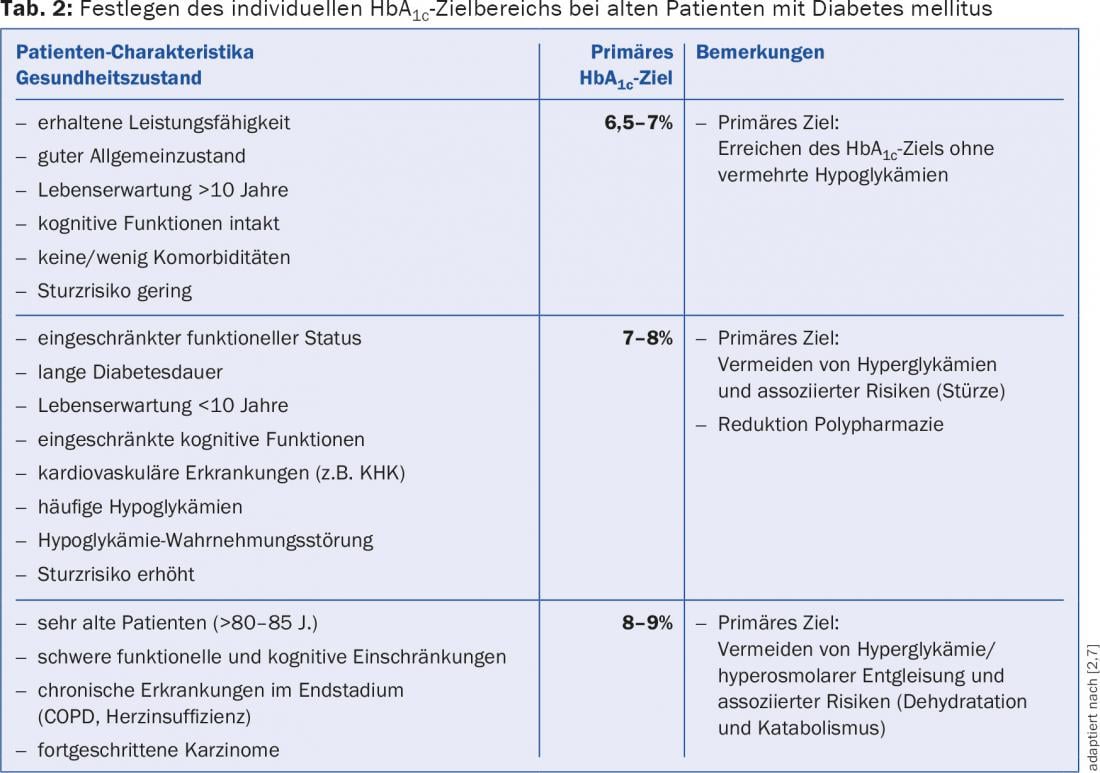
Establish the individual HbA1c target range (tab. 2): The goal of comprehensive diabetes therapy is to prevent or reduce microvascular and macrovascular secondary complications through adequate metabolic control and treatment of co-risk factors. In addition to hypoglycemia, persistent hyperglycemic states (i.e., levels above 15-20 mmol/l) must be prevented, as they lead to dehydration and negative caloric balance due to glucosuria – in addition to unfavorable effects on cerebral function and visual acuity – and worsen malnutrition. Target values are set based on a wide variety of factors (life expectancy, hypoglycemia risk, patient resources, etc.) as in younger patients and on current recommendations [7] (Table 2).
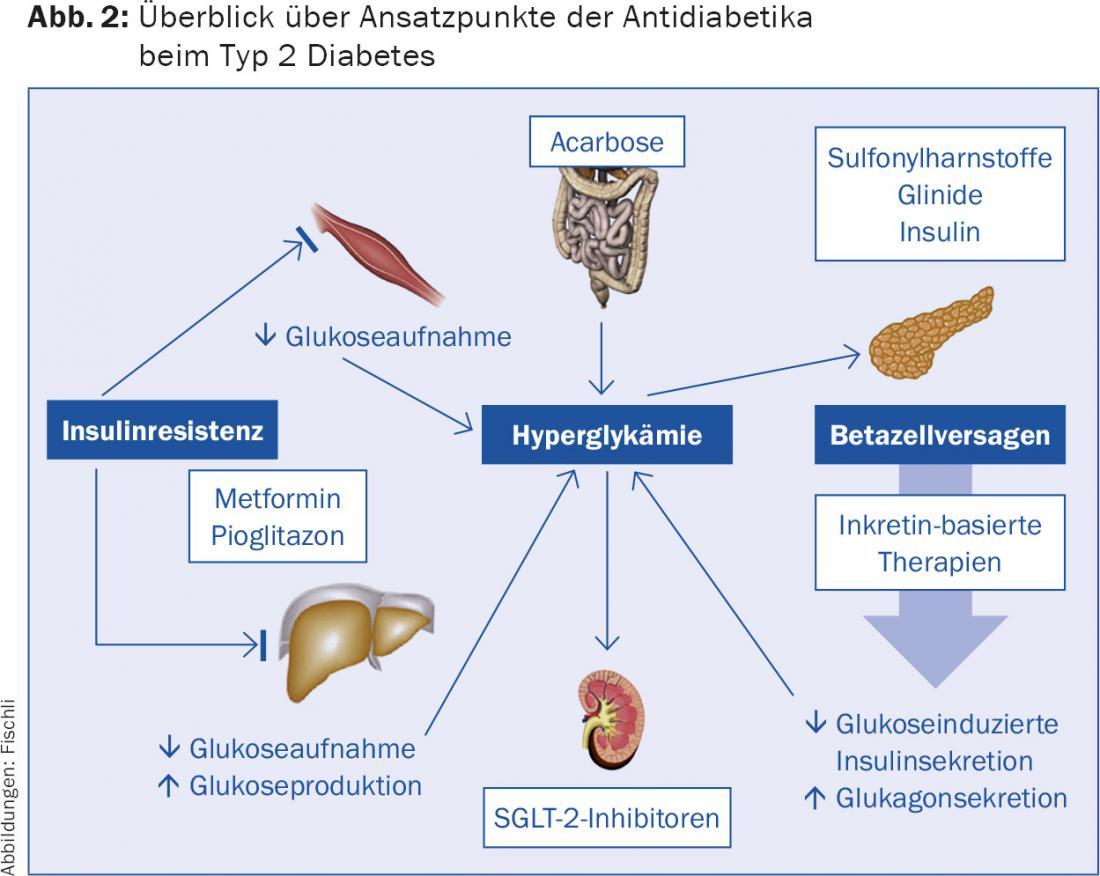
Selection of antidiabetic drugs according to the expected blood glucose-lowering effect and side effect profile (Fig. 2, Tab. 3) : After the target range [7,8] suitable for the patient has been defined, the corresponding therapeutic regimens are determined. The expected blood glucose-lowering effect as well as the side effect profiles must be taken into account. Any renal function impairment with decrease in GFR below 60 ml/min requires critical re-evaluation of antidiabetic therapy [9]. If necessary, the dose must be adjusted or the medication stopped (Tab. 3).
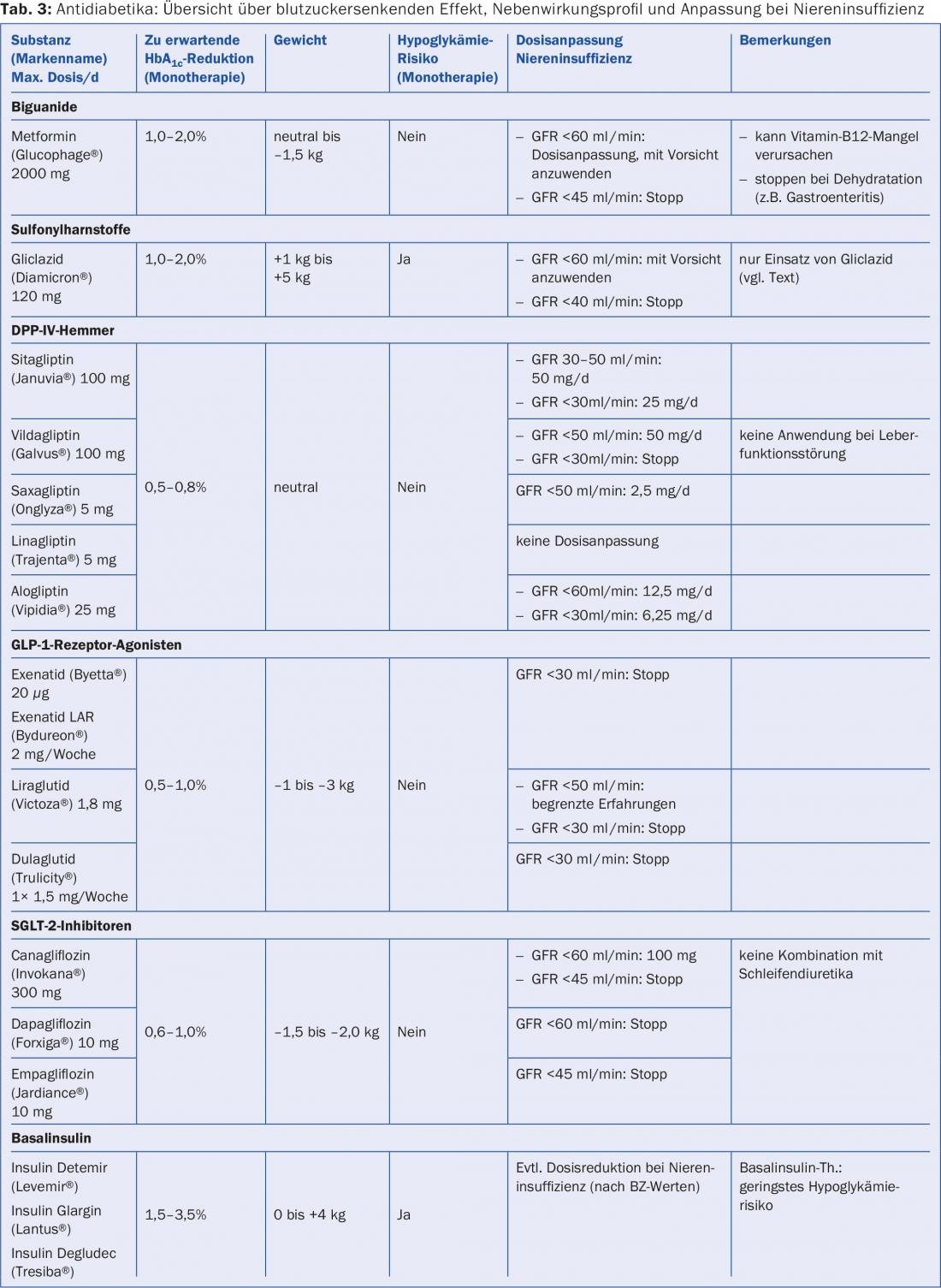
Overview of the most commonly used therapeutics
Metformin: Metformin still forms the first choice in drug therapy for type 2 diabetes mellitus. In elderly patients with a GFR below 60 ml/min, metformin should generally no longer be used. The risk of lactic acidosis is increased especially in the presence of other diseases (severe heart failure, liver failure, severe COPD). Instruct patients that metformin must be mandatorily paused in conditions of dehydration and risk of rapid development of prerenal renal failure (e.g., high fever, gastroenteritis) and before application of radiographic contrast media. Note that metformin reduces intestinal vitamin B12 absorption and may lead to vitamin B12 deficiency, which can worsen polyneuropathy or cognitive function.
Sulfonylureas: Sulfonylureas carry a risk of hypoglycemia and are a particular problem in patients with malnutrition and irregular food intake (dementia syndromes!). Of the preparations available in Switzerland, primarily only gliclazide (e.g. Diamicron®) should be used, since this substance has the lowest hypoglycemic potential and – in contrast to glibenclamide and glimepiride – is degraded hepatically to inactive metabolites. Gliclazide should be stopped at a GFR below 40 ml/min.
Gliptins: Due to their good tolerability, low side effect potential (weight neutral), peroral administration, and lack of intrinsic risk for hypoglycemia, gliptins are a good therapeutic option in elderly patients. It should be noted that the dose – except for linagliptin (Trajenta®) – must be adjusted in the case of renal insufficiency (Tab. 3) . However, the blood glucose-lowering effect is lower compared with sulfonylureas or GLP-1 analogues.
GLP-1 receptor agonists: liraglutide (Victoza®) and exenatide (Byetta®/Bydureon®) must be injected subcutaneously and are associated with gastrointestinal side effects in 10-20%, especially in the initial phase. They lead to weight loss and are therefore unsuitable in patients with malnutrition. In overweight, insulin-resistant diabetics, they are a viable option and can be combined with insulin (liraglutide, exenatide, or the combination of insulin degludec and liraglutide Xultophy®). GLP-1 receptor agonists are stopped at GFR below 30 ml/min.
SGLT-2 inhibitors: These new compounds inhibit renal tubular glucose reabsorption and act independently of residual beta cell function and insulin resistance. This makes it – in addition to the lack of hypoglycemic risk and weight-reducing effect – a valid therapy option also for older diabetics with long-standing diabetes. The SGLT-2 inhibitors can be combined with insulin. Note the increased risk of urogenital infections (especially in women) and the risk of volume depletion (orthostatic hypotension) when the agents are combined with loop diuretics. The effect is limited with increasing renal insufficiency, which is why preparations are stopped at a certain degree of renal function impairment (Tab. 3).
Insulin: Insulin therapy is often started too late, but it offers numerous benefits and can significantly improve quality of life in elderly diabetics [10]. Insulin remains the antidiabetic agent with the greatest therapeutic potency and can effectively correct symptoms of hyperglycemia such as fatigue, osmotic diuresis, dehydration, and visual acuity changes. Insulin has virtually no interaction potential and has an anabolic effect, which is of decisive advantage in malnourished, sarcopenic patients. Renal insufficiency slows the breakdown of insulin, so the dose must be reduced. Hypoglycemia can be significantly reduced by selecting the appropriate regimen and slow dose titration. Basal insulin therapy, which is usually combined with oral antidiabetic agents, has the lowest hypoglycemic potential. Central to this is the education of patients or the identification of cognitive dysfunctions that make insulin self-administration impossible or endanger the patient due to incorrect management or insulin misadministration.
Literature:
- Lakey, WC, et al: Are current clinical trials in diabetes addressing important issues in diabetes care? Diabetologia 2013; 56(6): 1226-1235.
- Kirkman MS, et al: Diabetes in older adults. Diabetes Care 2012; 35(12): 2650-2664.
- Sinclair AJ, et al: European Diabetes Working Party for Older People 2011 clinical guidelines for type 2 diabetes mellitus. Executive summary. Diabetes Metab 2011; 37(Suppl 3): S27-S38.
- Kalyani RR, Egan JM: Diabetes and altered glucose metabolism with aging. Endocrinol Metab Clin North Am 2013; 42(2): 333-347.
- Yaffe K, et al: Association between hypoglycemia and dementia in a biracial cohort of older adults with diabetes mellitus. JAMA Intern Med 2013; 173(14): 1300-1306.
- Yau RK, et al: Diabetes and risk of hospitalized fall injury among older adults. Diabetes Care 2013; 36(12): 3985-3991.
- Inzucchi SE, et al: Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012; 35(6): 1364-1379.
- Girlich C, Hoffmann U, Bollheimer C: Treatment of type 2 diabetes in elderly patients. Internist (Berl) 2014; 55(7): 762-768.
- Zanchi A, Lehmann R, Philippe J: Antidiabetic drugs and kidney disease–recommendations of the Swiss Society for Endocrinology and Diabetology. Swiss Med Wkly 2012; 142: w13629.
- Reza M, et al: Insulin improves well-being for selected elderly type 2 diabetic subjects. Diabetes Res Clin Pract 2002; 55(3): 201-207.
- Meneghini LF, et al: Weight beneficial treatments for type 2 diabetes. J Clin Endocrinol Metab 2011; 96(11): 3337-3353.
- Vasilakou D, et al: Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med 2013; 159(4): 262-274.
HAUSARZT PRAXIS 2015; 10(10): 20-26