With PCI, mortality in acute coronary syndrome has been impressively reduced. An overview of current technical developments (stents), key treatment guidelines, and adjunctive therapies. Includes overview interventional vs surgical treatment options.
Percutaneous transluminal coronary balloon angioplasty (PTCA) was introduced into clinical practice 40 years ago by Andreas Grüntzig and was the cornerstone for the rapid further development of interventional cardiology. Since then, this discipline has continuously expanded the range of indications due to numerous technological and pharmacological advances. In particular, the introduction of stents and their evolution from uncoated bare-metal stents (BMS) to first-generation drug-eluting stents (DES) to newer-generation DES has led to percutaneous coronary intervention (PCI) with excellent results in both acute coronary syndrome (ACS) and stable coronary artery disease (CAD). Adjunctive drug therapy is essential not only to prevent the rare stent thrombosis but also to favorably affect the underlying atherosclerosis.
Utility of PCI in acute coronary syndrome and stable coronary artery disease.
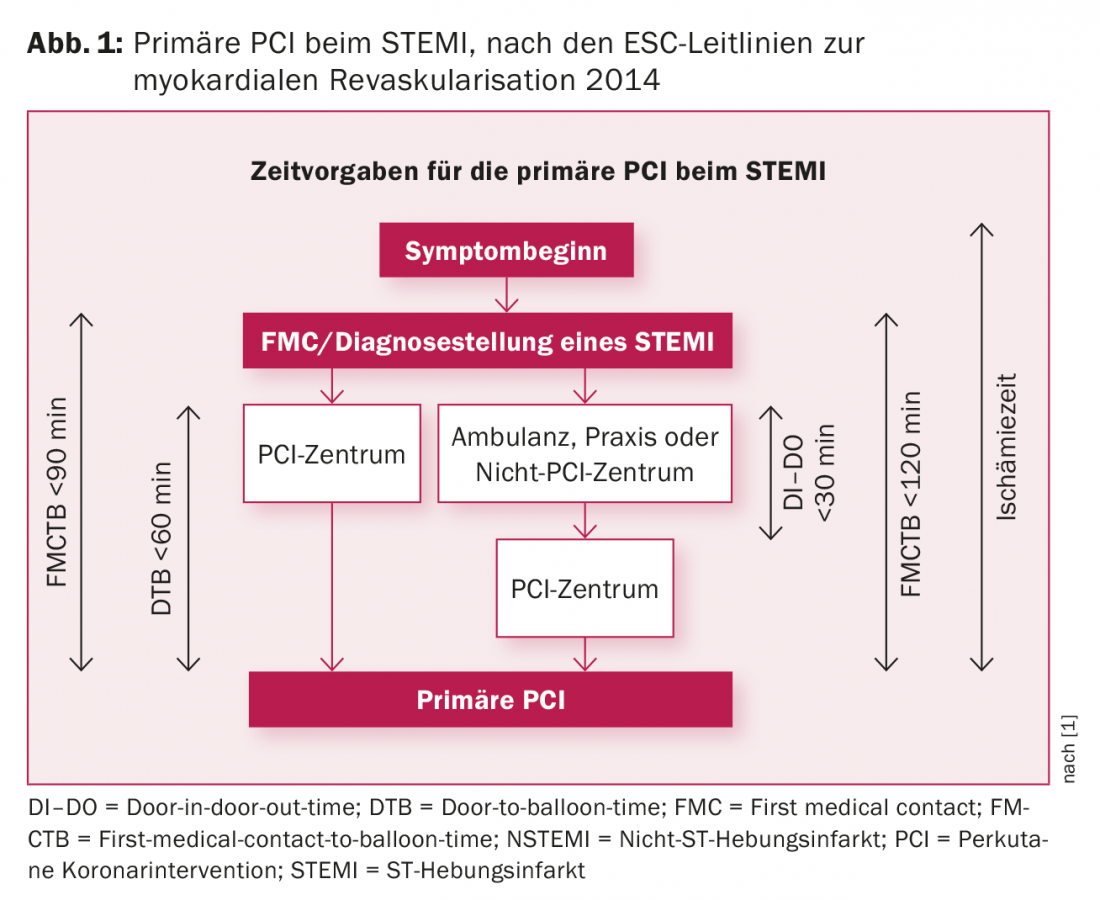
Percutaneous coronary intervention is the cornerstone in the treatment of acute coronary syndrome with prognostic significance. Due to the nationwide rapid availability of emergency PCI, virtually every ST elevation myocardial infarction (STEMI) can be revascularized within the recommended 60-90 minutes (Fig. 1) [1]. Compared with thrombolysis, primary PCI reduces infarct size, rates of re-infarction and re-occlusion of vessels and intracranial hemorrhage, and improves survival. With a door-to-balloon time (admission to a PCI-capable hospital until reopening of the vessel) of less than 60 minutes, the average mortality of a STEMI today is 3%, whereas in the era of thrombolysis, mortality was twice as high. In cardiogenic shock secondary to acute myocardial infarction, immediate revascularization improves survival compared with intensive care alone from 37% to 50% during the first six months.
For patients with stable coronary artery disease who suffer from angina despite anti-ischemic therapy, myocardial revascularization is indicated as symptomatic therapy, and there is evidence that with new-generation DES, PCI may also improve prognosis [2].
Stent type
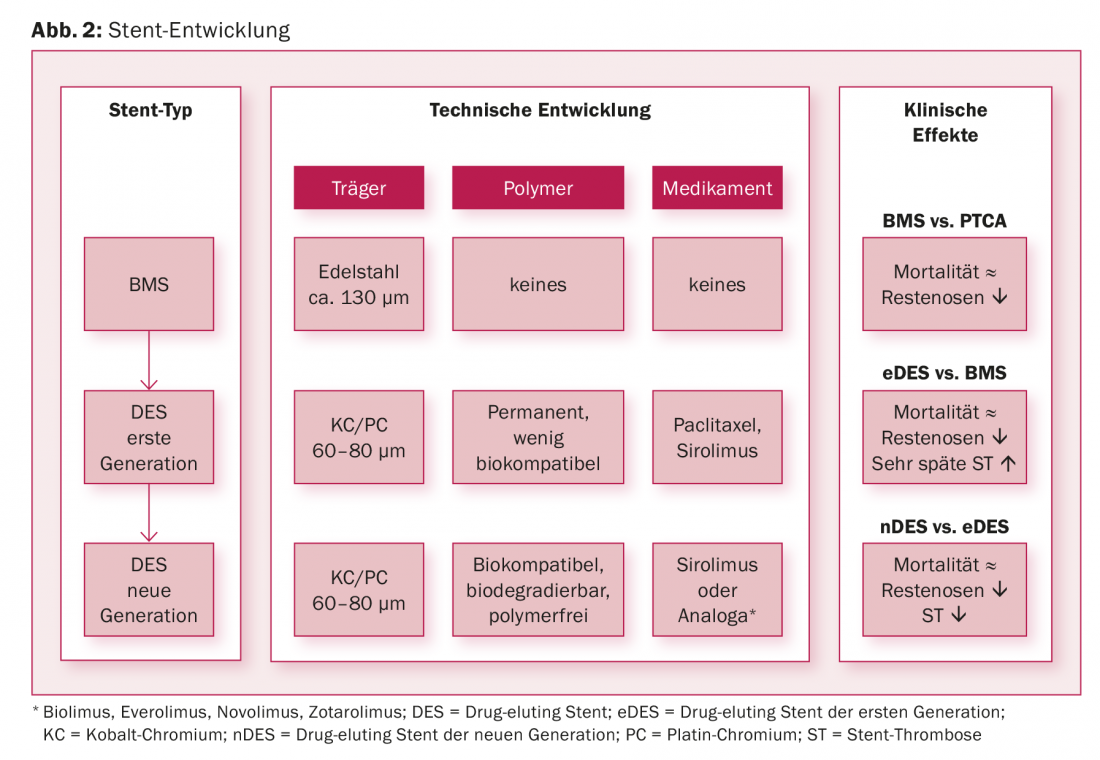
Important limitations of balloon angioplasty were the occurrence of dissections, impending vessel occlusions, and restenosis. The development of BMS has effectively treated acute vascular occlusions by covering the dissecting membrane, effectively eliminating the need for emergency bypass surgery. It is true that BMS also had a favorable effect on restenosis rate because the metal grids prevent elastic recoil of dilated vessels. Nevertheless, restenosis (instent restenosis) remained common under BMS. This led to the development of drug-eluting stents, which contain a polymer-supported antiproliferative drug in very small doses in addition to the metal scaffold. This is released into the arterial wall over several weeks to months after stent implantation, effectively suppressing neointimal hyperplasia. In fact, first-generation DES reduced the restenosis rate and thereby also reduced the need for repeat revascularization by more than half, but at the price of an increased risk of stent thrombosis much later (>1 year after implantation). The further development of DES involved the scaffold as well as the polymer and the drug. First, the new generation DES have thinner cobalt or platinum-chromium scaffolds, making them less thrombogenic and more rapidly endothelialized. Furthermore, they consist of thinner, more biocompatible or biodegradable polymers or even manage without polymers. In addition, the amount of the required immunosuppressive sirolimus or its more potent analogues could be reduced (Fig. 2). Thus, under DES of the new generation, stent thrombosis rates are still 0.5-1%, restenosis rates are <5%, and mortality from acute coronary syndrome has been reduced to 2-3% in the long term [3,4]. Thus, the new-generation drug-eluting stents represent the gold standard in percutaneous coronary intervention and occupy a Class IA indication in the guidelines [1]. Efforts to further improve DES or new approaches such as bioresorbable scaffolds will find it difficult to achieve further clinically relevant improvements due to the already excellent results of new DES.
Bioresorbable scaffolds
The basic idea of bioabsorbable vascular scaffolds (BVS) is that they consist of a polymer- or magnesium alloy-based scaffold, which, depending on the product, is completely resorbed by the body within 6-36 months, in contrast to the metallic stents that remain permanently as foreign bodies in the coronary arteries. 3-6 months after implantation, but may nevertheless seal the lesions by their mechanical properties, prevent elastic recoil of the vessels, and also be coated with antiproliferative drugs to prevent neointimal hyperplasia. However, unlike the metal alloys commonly used for stents, the materials used have reduced radial strength and expansion limits despite thicker struts, making implantation more difficult. While pilot studies yielded promising results, they were inferior to newer-generation DES in terms of restenosis and stent thrombosis in the first randomized controlled trials. Currently, scaffolds with thinner struts, other material properties, and the use of special implantation techniques are under investigation [5].
The approach: radial vs. femoral
Although femoral access is technically simpler (larger and easier to puncture artery, more catheter stability due to fewer curves from the puncture site to the coronary branches), it has a greater risk of bleeding compared with access via the easier-to-compress radial artery. The MATRIX trial, which randomized radial vs. femoral access in patients with acute coronary syndrome, showed that this increased rate of relevant bleeding complications with femoral puncture was associated with increased mortality (2.2% vs. 1.6%, p=0.045) [6]. From the patient’s perspective, the radial approach also has the advantage of shortening the immobilization period after PCI.
“Complex” coronary artery disease and the main stem: interventional vs. surgical
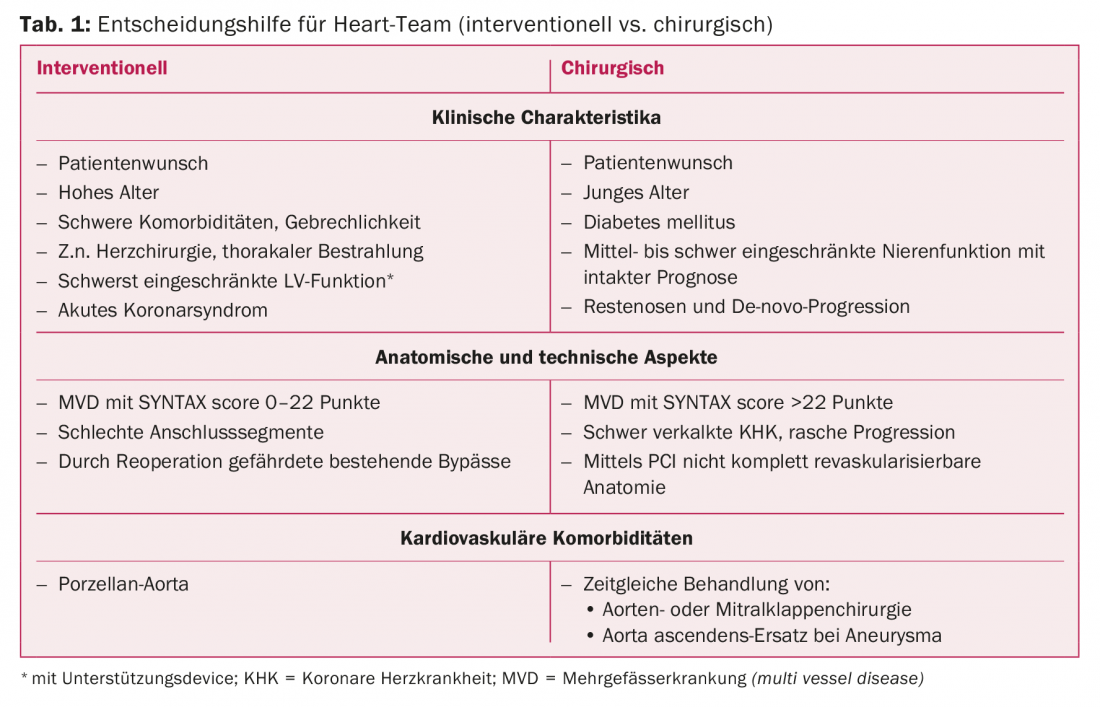
As in three-vessel coronary artery disease with high lesion complexity or diabetes mellitus as comorbidity, aortocoronary bypass grafting (ACB) has been considered superior to PCI (with first-generation DES) for main stem stenosis. The most recent randomized trials (EXCEL [7]) and meta-analyses comparing treatment of main stem stenosis by PCI versus ACB showed equivalent outcomes in the mid-term comparison in terms of death, myocardial infarction, and stroke. The advantage of a periprocedurally lower risk of myocardial infarction with PCI is lost in the long-term course due to a slightly higher rate of spontaneous myocardial infarction after 30 days. Although cardiac surgery has made advances that have led to a reduction in periprocedural stroke, there is still a slightly increased risk after ACB compared with PCI. In contrast, repeat revascularizations occur more frequently after PCI compared with ACB. Today, in the case of multivessel disease or main stem stenosis, an interdisciplinary discussion is held in the Heart Team, taking into account comorbidities and the individual situation, in order to offer the patient the optimal treatment strategy (Table 1) [1]. Recently, great progress has been made in the reopening of chronically occluded vessels (“chronic total occlusion”, CTO). In the hands of specialized surgeons, CTO can now be reopened via antegrade or retrograde approaches in >90%.
Adjunctive therapy
Although very good results are achieved with percutaneous coronary interventions for coronary artery disease (CAD), this is a focal treatment for stenoses or occlusions. However, the atherosclerosis of the coronary arteries underlying CHD requires long-term systemic therapy. In addition to control of cardiovascular risk factors, antiplatelet and cholesterol-lowering drug therapy are essential.
The antiaggregation therapy
The choice of P2Y12 inhibitor for dual antiplatelet therapy (DAPT) in addition to acetylsalicylic acid (ASA) depends on the indication and the presence of contraindications. In ACS, superiority of both prasugrel and ticagrelor over clopidogrel in terms of cardiovascular complications (cardiovascular death, myocardial infarction, and stroke) has been shown; there is no conclusive head-to-head comparison between prasugrel and ticagrelor. However, since there are contraindications to prasugrel (in particular, prior stroke or transient ischemic attack), ticagrelor is currently used more frequently. After ACS, DAPT is recommended for 12 months (Fig. 3). Prolonged DAPT (>12 months) leads to fewer ischemic complications but is associated with an increased risk of bleeding, resulting in no mortality benefit [8].
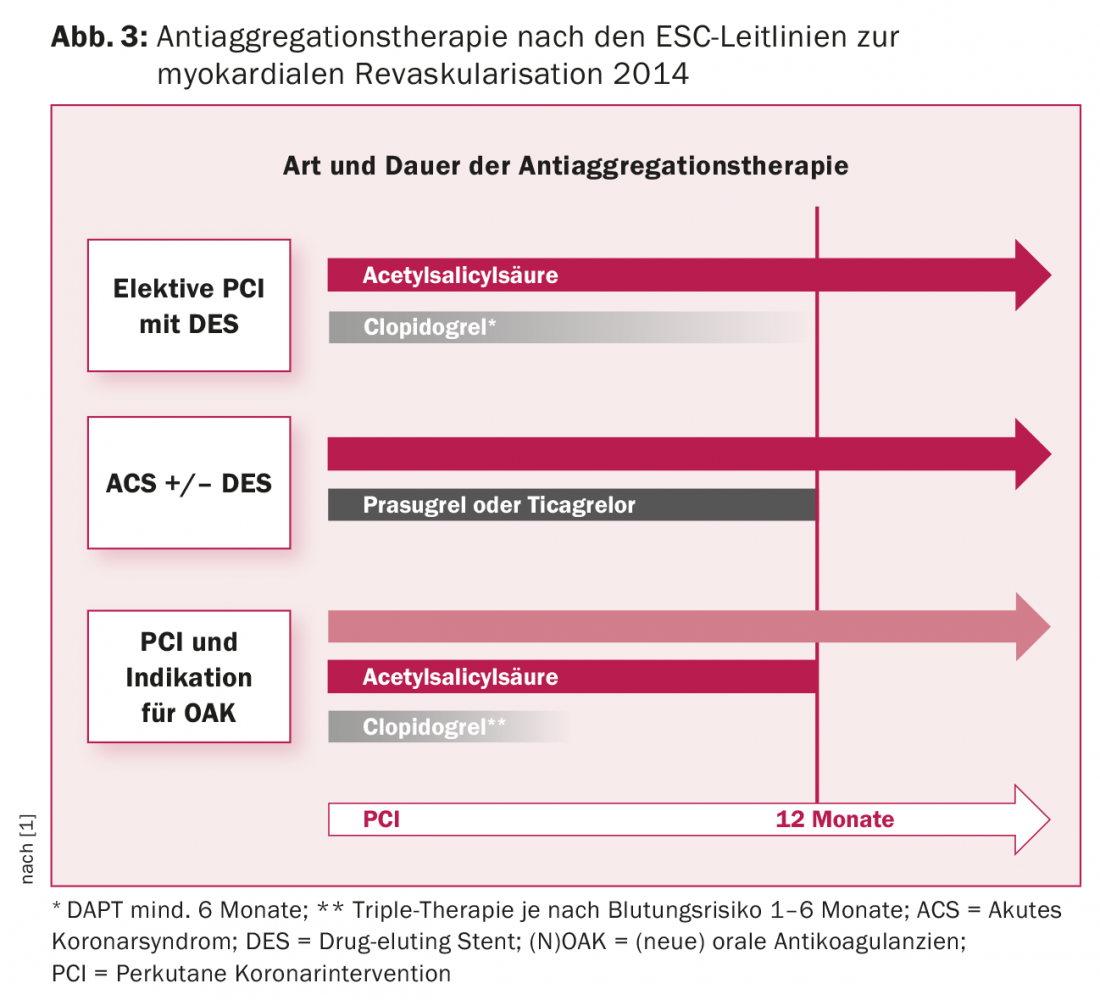
For elective PCI, DAPT with clopidogrel is recommended for a duration of 6-12 months [1]. However, a shorter duration of minimally 1-3 months may also be selected for the new DES because of the lower risk of stent thrombosis for patients with increased bleeding risk, concomitant oral anticoagulation (in terms of triple therapy), or the need for noncardiac surgery [9]. The PRECISE-DAPT score is useful for calculating an individual’s benefit-risk profile and can be a helpful guide in determining the optimal duration of DAPT [10]. Triple therapy is generally associated with increased bleeding rates. Less intensive treatment regimens with OAK and clopidogrel or rivaroxaban and clopidogrel without the application of aspirin show less bleeding [11]. In patients who require long-term anticoagulation, e.g., because of atrial fibrillation or a mechanical prosthetic heart valve, 12 months after PCI, continuation of oral anticoagulation alone without ASA is sufficient.
The cholesterol lowering therapy
Hypercholesterolemia, along with nicotine use and arterial hypertension, is the most important cardiovascular risk factor. High-dose statin therapy lowers low-density lipoprotein cholesterol (LDL-C) levels by up to 40-50% (with rosuvastatin 20 mg/d and atorvastatin 40-80 mg/d), and also achieves stabilization (and, at very high doses, regression) of preexisting plaques and a reduction in vascular inflammatory activity via pleiotropic effects and reduces cardiovascular complications in the long term. Statins are therefore indicated as secondary prophylaxis in all patients with CHD, and as intensified therapy after acute coronary syndrome. If the target LDL-C of <1.8 mmol/l (or a reduction of >50% from baseline) is not achieved with statin therapy, a further LDL-C reduction of approximately 10% can be achieved by adding ezetimibe. The new proprotein convertase subtilisin kexin type 9 (PCSK9) inhibitors have been available since 2016. These once-every-two-week subcutaneous drugs allow potent LDL-C lowering beyond statins and are approved in patients with familial dyslipidemia and as add-on therapy for patients with manifest atherosclerotic cardiovascular disease on maximally tolerated statin therapy. Evidence of long-term mortality reduction (as opposed to myocardial infarction and stroke rates) does not yet exist [12].
Take-Home Messages
- Percutaneous coronary intervention is one of the most commonly performed therapeutic interventions in medicine. The rapid and widespread availability of primary PCI has led to an impressive reduction in mortality from acute coronary syndromes.
- The new generation drug-eluting stents represent the current gold standard.
- PCI is also increasingly performed in patients with main stem and three-vessel disease.
- DAPT (ASA + P2Y12 inhibitor) is recommended for a duration of 6-12 months after PCI or acute coronary syndrome.
- PCSK9 inhibitors are now available for patients with coronary artery disease who do not achieve sufficient LDL cholesterol reduction with statin therapy or who cannot tolerate statins.
Literature:
- Windecker S, et al: 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014; 35(37): 2541-2619.
- Windecker S, et al: Revascularisation versus medical treatment in patients with stable coronary artery disease: network meta-analysis. BMJ 2014: 348: g3859.
- Räber L., et al: Very late coronary stent thrombosis of a newer-generation everolimus-eluting stent compared with early-generation drug-eluting stents: a prospective cohort study. Circulation 2012; 125(9): 1110-1121.
- Bønaa KH, et al: Drug-Eluting or Bare-Metal Stents for Coronary Artery Disease. N Engl J Med 2016; 375(13): 1242-1252.
- Sotomi Y, et al: Bioresorbable scaffold: the emerging reality and future directions. Circ Res 2017; 120(8): 1341-1352.
- Valgimigli M, et al: Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet 2015; 385(9986): 2465-2476.
- Stone GW, et al: Everolimus-eluting stents or bypass surgery for left main coronary artery disease. N Engl J Med 2016; 375(23): 2223-2235.
- Bonaca M, et al: Long-term use of ticagrelor in patients with prior myocardial infarction. N Engl J Med 2015; 372(19): 1791-1800.
- Levine GN, et al: 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2016; 68(10): 1082-1115.
- Costa F, et al: Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet 2017; 389(10073): 1025-1034.
- Gibson CM, et al: Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N Engl J Med 2016; 375(25): 2423-2434.
- Sabatine MS, et al: Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med 2017.
CARDIOVASC 2017; 16(3): 4-8









