From the vast field of ENT, some symptoms that are particularly common in practice will be highlighted with a view to current developments and new findings. Under the influence of current research, there are constant changes in therapy recommendations for certain indications and there are also numerous advances with regard to diagnostics.
Many aspects of everyday medical life are currently still dominated by the corona pandemic, yet research is not standing still and there is exciting news to report from various subfields. An overview of continuously updated ENT guidelines is available at www.orl-hno.ch/ueber-uns/guidelines.html. In daily practice, patients do not present with a diagnosis, but rather report their symptoms. In the spirit of translational medicine, Ralph Litschel, MD, ENT practice at Roter Platz, St.Gallen, presented current findings on common symptomatology from a theoretical and practical perspective [1].
Streptococcal angina: antibiotics are not always necessary
“In the United States, 80% of cases of streptococcal angina are treated with antibiotics; in Switzerland, about 40% are treated with antibiotics,” said Dr. Litschel [1]. According to an article published in 2019, streptococcal angina usually has a benign course and resolves spontaneously within a week even without antibiosis [2]. A throat swab is recommended for a McIsaac score ≥3 (rapid test for group A streptococci). If the result is negative, no antibiotic treatment is required; if the rapid test is positive, antibiotics can be used on a delayed basis, i.e., if symptoms worsen or do not improve within 72 hours. Patients should be advised that antibiotics do little to relieve symptoms or shorten symptom duration compared with analgesics and that complications are rare. Unnecessary antibiotics destroy the normal bacterial flora and contribute significantly to the spread of resistant bacteria. For symptom relief, proven home remedies (e.g. lime blossom or sage tea, and bed rest in case of fever) are advisable, and ibuprofen or paracetamol can be used to reduce pain. Furthermore, topical local anesthetics in the form of lozenges, gargle solution or throat spray, which may be disinfectant, are among the recommended measures. Patients should check back in with their physician if their condition worsens. Close follow-up is advised in very ill patients or young children (<3-5-years-old) or in very elderly or debilitated individuals, as well as in those with a positive family history of rheumatic fever.
Antibiotics are also not indicated for the relief of peritonsillar abscesses or rheumatic fever according to most international guidelines. “Nowadays, there is hardly any rheumatic fever in Switzerland,” said the speaker [1].
Laryngopharyngeal reflux vs. GERD
Symptoms such as globus sensation, clearing of throat, cough, hoarseness or burning sensation in the throat may be indicative of laryngopharyngeal reflux. This form of reflux primarily affects the posterior laryngeal area, with marked swelling of the mucosa, Dr. Litschel said [1]. While gastroesophageal reflux (GERD) occurs primarily in a recumbent position and in the evening or at night, laryngopharyngeal reflux manifests during the day. The recommended treatment consists of high-dose PPI therapy for at least two months. A classic sonographic finding is enlarged lymph nodes, and in some cases lateral or median neck cysts.
What to do in case of nasal obstruction or epistaxis?
In the area of the nose and sinuses, obstruction of nasal breathing is one of the most common symptoms. Nasal septal deviation is often present, in the form of a spur clearly visible on computed tomography, and there is often nasal turbinate hyperplasia. Another possible cause is allergic rhinitis, but this topic is not discussed here. Therapy of restricted nasal breathing consists mainly of glucocorticoid nasal spray, saline nasal rinses if necessary, and moisturizing nasal ointment if the nasal mucosa is very dry. If these measures do not bring relief, there is also the possibility of surgical treatment, explains Dr. Litschel [1].
The most common ENT emergencies include spontaneous leakage of blood from one or both nostrils or mixing of nasal secretions with blood. “There are many possible reasons for epistaxis,” emphasized the speaker, although these often cannot be conclusively determined [1]. In 90% of cases of epistaxis, anterior areas are affected, usually involving the locus Kiesselbachi. “This is located at the nasal entrance, where there is a network of lymphatic vessels where bleeding can easily occur, especially if the nose is a little dry,” Dr. Litschel explains. Few hemorrhages occur more posteriorly, in the region of the sphenopalatine artery or one of its branches. Immediate measures for nosebleeds include an upright sitting position, the head should be slightly bent forward and the nostrils compressed for at least five minutes. Many patients automatically place their head in the neck, but this is wrong, as swallowing blood can trigger an urge to gag or vomit, the speaker explains. Further, it is recommended to put a cold pack on the neck. Electrocoagulation may be required if necessary.
In uncomplicated rhinosinusitis, no X-ray diagnosis
According to the Swiss Society of Oto-Rhino-Laryngology, Otolaryngology and Facial Surgery (SGORL), acute rhinosinusitis is a clinical diagnosis and is defined by at least two of the following symptoms occurring acutely and lasting up to 12 weeks: purulent nasal secretion, nasal obstruction, facial pain, and/or diminished smell. A nasal endoscopy is performed for confirmation. If a complication of rhinosinusitis or other underlying diagnosis is suspected, cone-beam CT or computed tomography is recommended.
The “European Position Paper on Rhinosinusitis and Nasal Polyps” (EPOS) 2020 is very comprehensive and addresses various aspects in detail (overview 1) [3]. Chronic rhinosinusitis is said to occur when symptoms persist for more than 12 weeks. “There is very good evidence that surgery has an 89% chance of success,” the speaker quoted from the EPOS paper [1,3]. An imaging examination must be performed prior to performing any surgical procedure. There has been significant progress in this area in recent years. Cone-beam CT is associated with approximately 40% less radiation exposure than conventional computed tomography and the slice thickness is less than 0.3 mm [4]. Dr. Litschel offers cone-beam CT in his practice itself. By using the “long dose mode”, the radiation dose could be further reduced, and yet much could be detected in this mode. Surgical intervention is also usually performed for chronic rhinosinusitis with polyps if there is no response to medical therapy.

Dentogenic sinusitis should also not be forgotten. In the field of dentogenic abscesses, there is an increase in the number of cases, Dr. Litschel reported, referring to the EPOS position paper 2020 [3]. Treatment options include surgical intervention of the sinuses for drainage in addition to dental rehabilitation.
Tinnitus and hearing loss
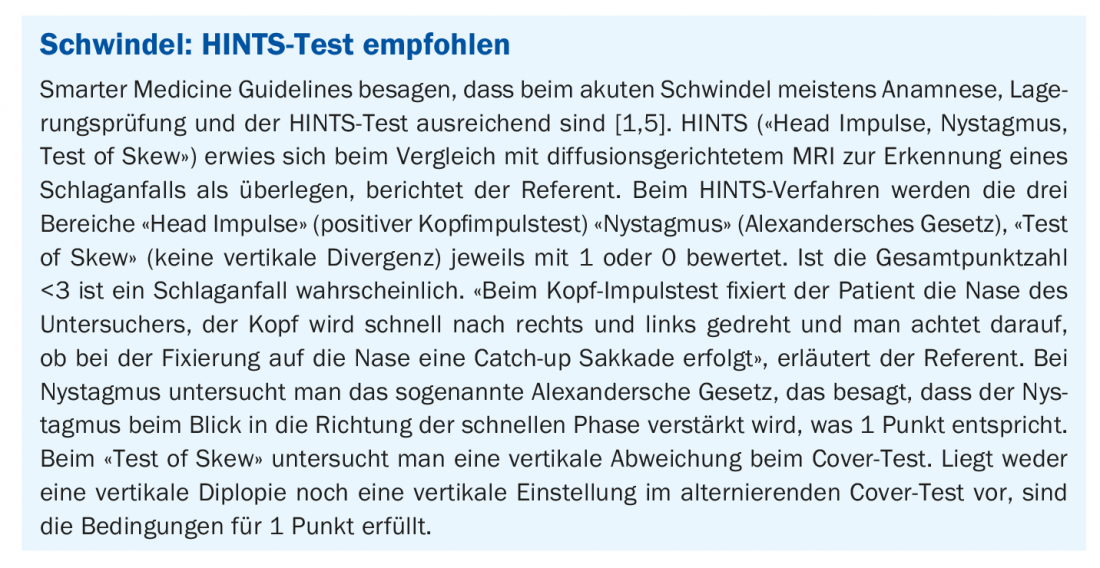
Towards the end of his presentation, Dr. Litschel discusses symptoms in the area of the auditory and vestibular organs (box) [1]. A hearing test should be performed for new-onset tinnitus, but an MRI is not necessary, the speaker explained. “Imaging is not useful for nonpulsatile tinnitus,” as can be read in the Smarter Medicine Guidelines [1,5]. There is no standard treatment for tinnitus in conventional medicine. There is evidence that hypnosis or hearing aids are helpful in certain cases, but the data are inconsistent. Sometimes psychotherapeutic treatment can help.
In case of hearing loss, therapy should be started within 1 week. The speaker reported a case in which therapy with prednisone 100 mg for 7 days was effective. A hearing test after 3 weeks showed a significant improvement in hearing loss.
Presbycusis refers to an age-related deterioration of hearing due to degenerative processes, which occurs especially at high frequencies. A hearing aid should be recommended to affected patients. Modern devices have noise suppression (e.g. wind), directional microphone technology, feedback suppression and comfort programs (e.g. music enjoyment). In Switzerland, the IV or AHV (from the age of 64 or 65 respectively) provide a cost subsidy for a hearing aid if the indication is appropriate.
Hearing problems in childhood are often due to adenoid hyperplasia. Therapy is initially conservative (Otovent balloon), and a glucocorticoid nasal spray is used if necessary. If symptoms persist for more than 3 months, surgical therapy (adenotomy, paracentesis, tympanostomy tube) is recommended.
Congress: FomF Family Doctor Training Days St. Gallen
Literature:
- Litschel R: Common ENT diseases in practice. Ralph Litschel, MD, FomF, Family Physician Continuing Education Days, 03/12/2021
- Hofmann Y, et al: Treatment of streptococcal angina, Swiss Med Forum 2019; 19(29).
- Fokkens WJ et al: European Position Paper on Rhinosinusitis and Nasal Polyps 2020. rhinology 2020; 58(Suppl S29): 1-464.
- Al Abduwani J, et al: Cone beam CT paranasal sinuses versus standard multidetector and low dose multidetector CT studies. Am J Otolaryngol 2016; 37(1): 59-64.
- Smarter Medicine Guidelines, www.smartermedicine.ch/de/top-5-listen/orl-hals-und-gesichtschirurgie.html, (last accessed Apr. 27, 2021).
HAUSARZT PRAXIS 2021; 16(7): 40-41 (published 6/28/21, ahead of print).