Renal cell carcinoma is one of the rather rare tumor entities. Therefore, treatment options were very limited for years and therapy was difficult. Meanwhile, tyrosine kinase inhibitors have expanded the options. Therapy with checkpoint inhibitors is also conceivable.
With a share of 2.4% of the annual new cancer cases in Switzerland, renal cell carcinoma is one of the rather rare tumor entities [1]. Light cell renal cell carcinoma is the largest subgroup of all renal cell carcinomas, accounting for approximately 75% [2]. Important risk factors for the development of renal tumor disease are mainly nicotine consumption as well as obesity, occupational exposure to solvents, petrolates and herbicides [3,4]. Approximately 2% of all renal cell carcinomas are associated with tumor predisposition syndromes, such as von Hippel-Lindau disease [5].
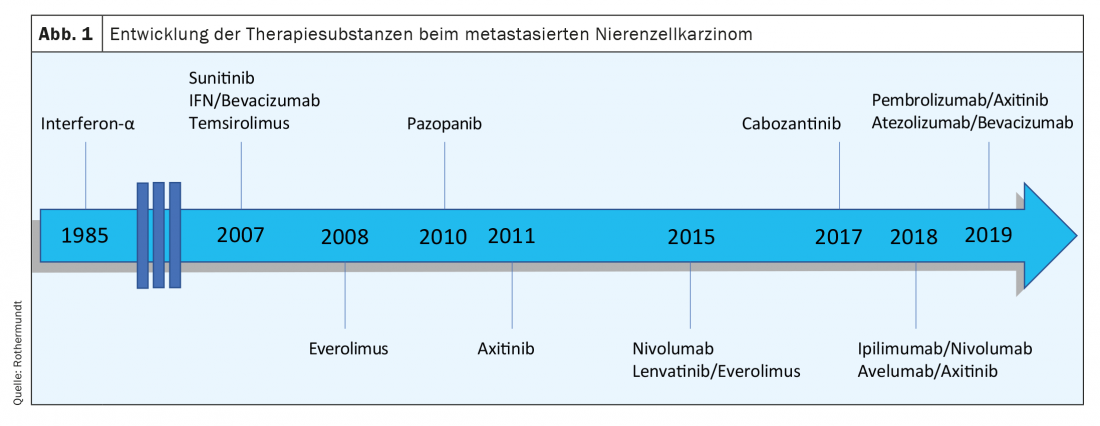
Approximately 12% of new diagnoses are primary metastatic tumors due to the presence of distant metastases [6]. For many years, treatment options for metastatic renal cell carcinoma were very limited and treatment was difficult. In 2007, sunitinib, a tyrosine kinase inhibitor (TKI), was shown for the first time to prolong progression-free survival (PFS) and increase response rate compared with interferon-alpha as first-line therapy in the metastatic setting [7]. Just over 10 years later, the phase III CheckMate-214 trial demonstrated superiority of the checkpoint inhibitor (CPI) nivolumab in combination with the CTLA-4 inhibitor ipilimumab over the standard of care sunitinib that had been used until then [8]. This investigation was followed by further studies – some with CPI alone or also combination therapies with CPI and TKI (Fig. 1). In this CME article, we will focus exclusively on the treatment of light cell renal cell carcinoma in the metastatic setting.
Risk classification
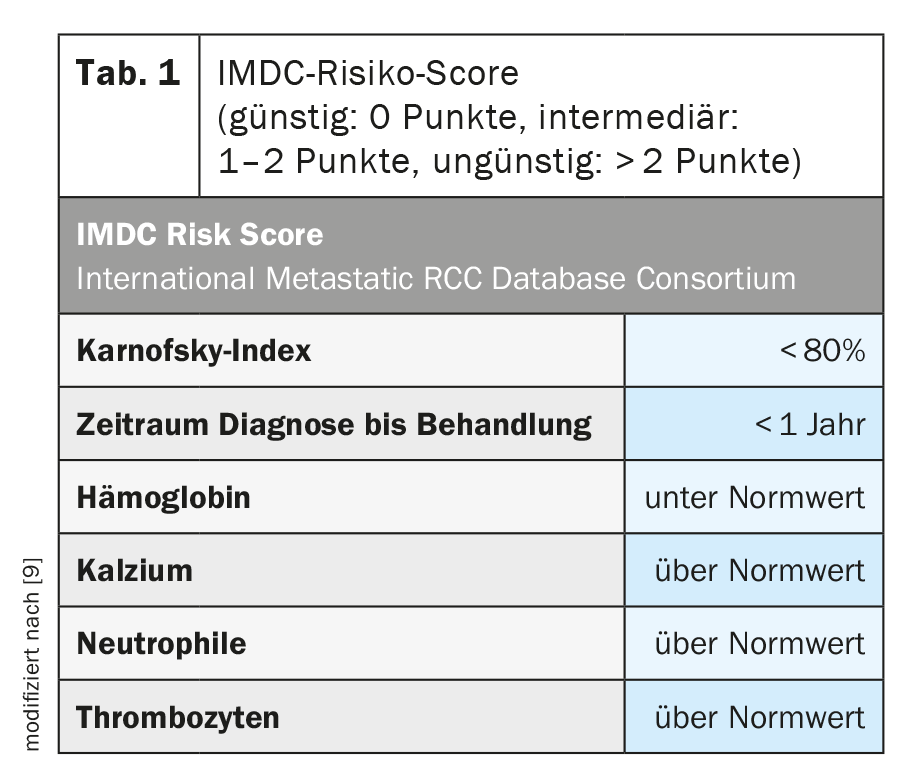
For a better assessment of the tumor situation as well as its prognosis, a risk classification has been developed (Tab. 1) . Depending on the score achieved in the IMDC risk score, the disease can be classified into the following risk groups: favorable, intermediate or unfavorable. This classification is not only important for estimating prognosis, but has been and continues to be included in clinical trials for stratification and has been shown to be predictive for therapeutic interventions [10].
First-line therapy
The treatment of metastatic renal cell carcinoma has changed significantly in recent years due to the use of new drugs from known substance groups (e.g., TKIs), but also due to the application of new therapeutic options, such as immunotherapy. In 2018, the CheckMate-214 trial demonstrated an improvement in objective response rate as well as overall survival (OS) with ipilimumab in combination with nivolumab compared to sunitinib. OS was 47 months in the ipilimumab/nivolumab arm compared with 26.6 months in the sunitinib arm with a hazard ratio (HR) of 0.66 (p<0.0001) [11]. This treatment effect is limited in the analyses to those patients with intermediate or unfavorable IMDC risk. In a favorable risk constellation, sunitinib shows a better overall response rate and also a better OS compared to immunotherapy.
Further studies in the first-line treatment of metastatic renal cell carcinoma followed. The Keynote 426 trial compared the combination of the PD-1 inhibitor pembrolizumab and the TKI axitinib with sunitinib alone. Thereby, the therapy combination significantly improved both OS and PFS compared to sunitinib (p<0.001) [12]. These outcomes were observed across all three IMDC risk groups-favorable, intermediate, and unfavorable .
In both the Checkmate-214 and Keynote-426 trials, complete remission (CR) was observed in approximately 9% for the immunotherapy approaches.
At this year’s ESMO Congress, data from the CheckMate 9ER trial were presented, comparing the combination therapy nivolumab and cabozantinib versus sunitinib, also in the first-line setting [13]. In doing so, Choueiri et al. showed that this combination therapy significantly improved PFS from 8.3 months (sunitinib monotherapy) to 16.6 months (nivolumab + cabozantinib). Also found was prolonged OS with a HR of 0.60. The objective response rate (ORR) was particularly impressive, with 55.7% in the combination arm vs. 27.1% with sunitinib. The observation period of 18 months to date is still relatively short, so it is unclear at this time to what extent the therapeutic response is longer-term.
Comparisons among these three studies are difficult because different prognostic groups were included and the patient distribution in the same was different. The observation times also differ considerably. The CPI with TKI combination regimens (Keynote-426 and CheckMate 9ER) showed a difference in overall survival after 1 month, whereas the ipilimumab and nivolumab combination showed a difference after 6 months. Accordingly, the therapeutic decision could fall on a TKI combination therapy instead of immunotherapy alone in the case of high therapeutic pressure.
For first-line treatment in metastatic renal cell carcinoma, there are also trial data on treatment with avelumab in combination with axitinib (JAVELIN-Renal-101 trial) [14]. This demonstrated prolonged PFS compared to sunitinib, but did not show this benefit in OS data. The combination of avelumab + axitinib is not being sought for approval in Switzerland.
Therapy with a tyrosine kinase inhibitor alone remains an option in the absence of availability or contraindications to one of the new standard combination therapies, especially for patients with favorable risk and very slow disease dynamics.
Active surveillance is also possible in well-selected patients, as demonstrated by a publication by Rini et al. proved: on median, patients could be observed for 14.9 months until the start of systemic therapy [15].
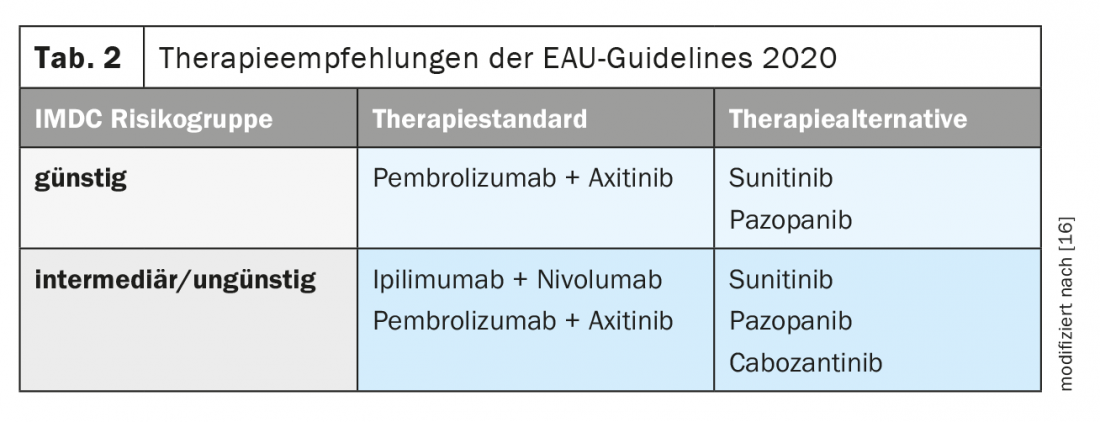
In the current guideline on renal cell carcinoma from the European Association of Urology (EAU), treatment recommendations have been recorded (Table 2) [16].
Currently, results are pending from the Phase III CLEAR trial comparing lenvatinib + everolimus or lenvatinib + pembrolizumab to sunitinib alone as first-line therapy in metastatic renal cell carcinoma with a 3-arm design. Lenvatinib and the PD-1 inhibitor showed promising results in advanced endometrial cancer in a study published this year [17].
Second-line therapy
The choice of drug class for two-line therapy is directly related to the first-line therapy already administered. The phase III Checkmate-025 study compared nivolumab with everolimus after 1-2 prior targeted VEGF therapies. Immunotherapy improved both OS and quality of life. Also, grade 3/4 toxicity was seen less frequently with nivolumab therapy compared with everolimus (19% vs. 37%). No improvement in PFS was observed [18]. A comparable improvement in OS, i.e. by approximately 5 months, was also demonstrated by cabozantinib compared with therapy with everolimus (Meteor study) [19].
The impact of first-line checkpoint inhibitor therapy on subsequent systemic therapies is unclear, as randomized trial data are not yet available. However, a phase II study (CaboPoint) is currently recruiting in Switzerland to investigate cabozantinib as second-line therapy – in cohort A after first-line therapy with ipiliumumab and nivolumab and in cohort B in case of progression to combination CPI and VEGF-targeted therapy.
Also, in a phase III study also accessible in Switzerland, the molecule MK-6482 PN011 – a HIF-2α inhibitor – is being compared to cabozantinib in combination with lenvatinib as a two-line therapy. HIF as a hypoxia-induced factor is involved in the expression of VEGF growth factors.
Data from a phase II study of lenvatinib + pembrolizumb after progression on PD-1/PD-L1 CPI therapy were presented at ASCO 2020. ORR at 24 weeks was 55% (irRECIST according to Investigator Assessment), and PFS was 11.7 months. This treatment thus appears promising even after prior immunotherapy [20].
Side effect profile
Due to different mechanisms of action of the substance classes used in metastatic renal cell carcinoma, there are also different side effect profiles. In the case of immunotherapies, these are so-called immune-mediated side effects, whereby reactions in a wide variety of organs are possible and the side effects can sometimes also be severe. It is crucial to know about, recognize and treat them at an early stage. Especially rare side effects, such as myocarditis and neurotoxicity need to be considered [21,22]. The administration of immunotherapies as well as further patient care should therefore be carried out by an experienced team of physicians, whereby an interdisciplinary approach is usually goal-oriented. The CheckMate-214 trial demonstrated that health-related quality of life was better in patients treated with ipilimumab + nivolumab compared with sunitinib alone [23]. Accordingly, the incidence of grade 3/4 adverse events was higher with sunitinib. The most common side effects of TKIs include diarrhea, skin toxicity, fatigue, and possible hematologic and cardiac changes.
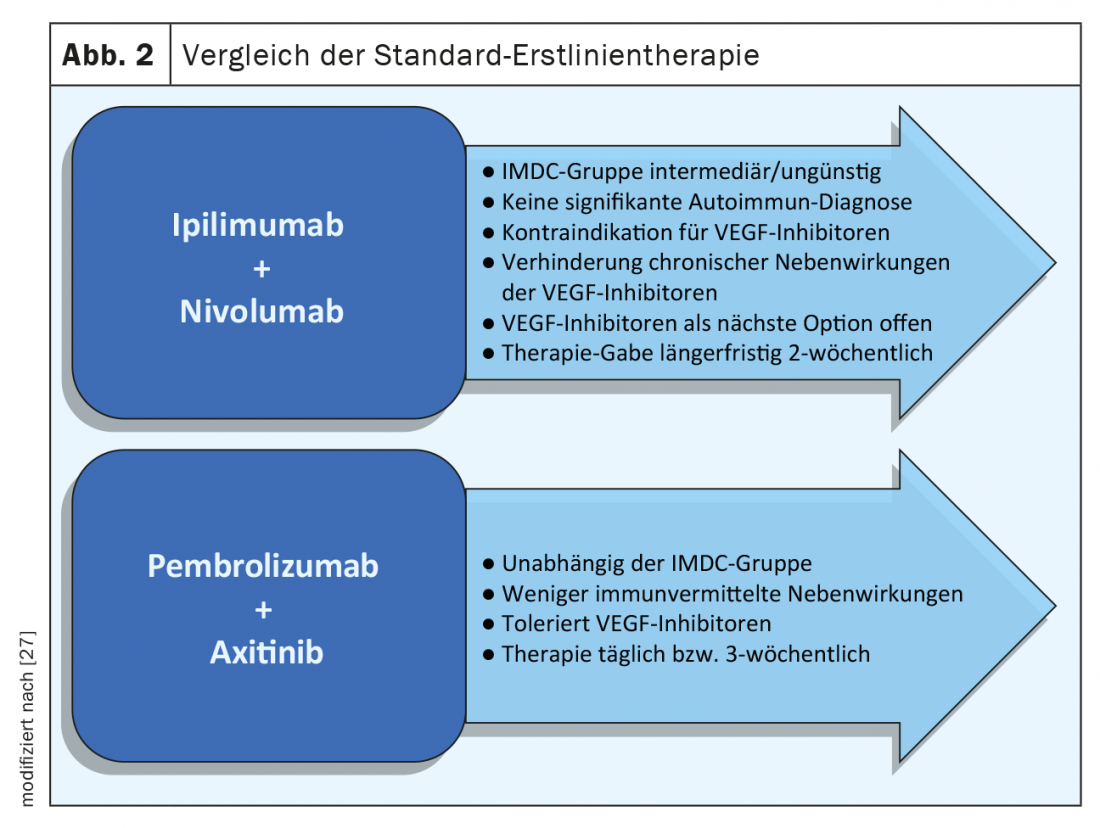
In addition to the different substance classes, there are also differences in application and therapy intervals. While ipilimumab/nivolumab switches to nivolumab alone after three months, the combination therapies CPI and TKI involve continuous tablet use with additional infusion therapy, the long-term toxicities of which must be considered. Tablet therapy is well controllable and side effects are usually rapidly reversible after discontinuation (Fig. 2) . To support patients and improve adherence and safety, leaflets from the Swiss Society of Medical Oncology (SGMO) and Oncology Care Switzerland (OPS) can be used [24].
Molecular markers
Molecular markers could help in making the best treatment choice among the multiple treatment options. However, aside from the IMDC risk score, there is no recognized predictive marker to date that can be used in decision making.
According to Checkmate-214 data, PD-L1 expression appears to be predictive of response to ipilimumab/nivolumab therapy (PD-L1 expression <1%: ORR 37%; PD-L1 expression ≥1%: ORR 54%) and PFS (PD-L1 expression <1%: PFS 11 months; PD-L1 expression ≥1%: PFS 22.8 months to be predictive [10]. However, there was no difference in terms of the OS. Thus, the role of -PD-L1 remains controversial. In the Keynote-426 study as well as in the CheckMate-9ER study, no correlation between the level of PD-L1 expression and response to therapy has been observed so far.
The IMmotion151 trial compared atezolizumab/bevacizumab with sunitinib [25]. In addition, various biomarker analyses were performed and no correlation between PFS and tumor mutational burden (TMB) could be shown. However, specific gene expression signatures have been shown to be associated with therapeutic effects. For example, evidence of an angiogenesis signature correlated with response to sunitinib. In contrast, a T-effector signature showed a benefit of immunotherapy with atezolizumab [26]. In the BIONIKK study, a randomized prospective phase II study presented at this year’s ESMO, different molecular groups were investigated with regard to the therapeutic response to the different therapeutic agents. This showed a better response of “immune-high” to immunotherapy with nivolumab and of tumors with “angio-high” to therapy with TKI. These molecular studies appear promising and will likely be available in the future to aid in therapy selection.
In addition to these molecular markers of the tumor, patient-related factors, such as age, comorbidities, and preferences, are currently the main factors influencing treatment decisions.
Take-Home Messages
- The current standard of care in first-line metastatic light cell renal cell carcinoma is pembrolizumab/xitinib for all risk groups and ipilimumab/nivolumab for intermediate- or adverse-risk patients (IMDC).
- Active Surveillance can be performed in selected patients and monotherapy with a tyrosine kinase inhibitor can be considered if the risk is favorable.
- New data are available for nivolumab in combination with cabozantinib, although this lacks approval in Switzerland.
- The side effect profile of the various drugs differs and may be decisive for the choice of therapy.
- Gene expression signature studies show differential treatment response and are promising.
Literature:
- Krebsliga Schweiz: Cancer in Switzerland: important figures. Status March 2020. www.krebsliga.ch/ueber-krebs/zahlen-fakten/-dl-/fileadmin/downloads/sheets/zahlen-krebs-in-der-schweiz.pdf.
- Linehan WM, et al. Clin Cancer Res. 2007;13: 671s-679s.
- Gelfond J, et al: Modifiable risk factors to reduce renal cell carcinoma incidence: insight from the PLCO trial. Urol Oncol, 2018. 36(7): 340.e1-340.e6.
- McLaughlin JK, Lipworth L: Epidemiologic aspects of renal cell cancer. Semin Oncol, 2000. 27(2): 115-123.
- Shuch B, Zhang J: Genetic Predisposition to Renal Cell Carcinoma: Implications for Counseling, Testing, Screening, and Management. J Clin Oncol, 2018: Jco2018792523.
- Siegel RL, Miller KD, Jemal A: Cancer statistics, 2020. CA Cancer J Clin, 2020. 70(1): 7-30.
- Motzer RJ, et al: Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med, 2007. 356(2): 115-124.
- Motzer RJ, et al: Nivolumab plus ipilimumab versus sunitinib in advanced renal cell carcinoma. N Engl J Med, 2018. 378(14): 1277-1290.
- Heng DY, et al: Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol, 2009. 27(34): 5794-5799.
- Méjean A, et al: Sunitinib Alone or after Nephrectomy in Metastatic Renal-Cell Carcinoma. N Engl J Med, 2018. 379(5): 417-427.
- Motzer RJ, et al: Nivolumab plus ipilimumab versus sunitinib in first-line treatment for advanced renal cell carcinoma: extended follow-up of efficacy and safety results from a randomised, controlled, phase 3 trial. Lancet Oncol, 2019. 20(10): 1370-1385.
- Rini BI, et al: Pembrolizumab plus axitinib versus sunitinib for advanced renal cell carcinoma. N Engl J Med, 2019. 380(12): 1116-1127.
- Choueiri TK: 696O_PR- Nivolumab + cabozantinib vs sunitinib in first-line treatment for advanced renal cell carcinoma: first results from the randomized phase 3 CheckMate 9ER trial. 2020: ESMO.
- Motzer RJ, et al: Avelumab plus axitinib versus sunitinib for advanced renal cell carcinoma. N Engl J Med, 2019. 380(12): 1103-1115.
- Rini BI, et al: Active surveillance in metastatic renal-cell carcinoma: a prospective, phase 2 trial. Lancet Oncol, 2016. 17(9): 1317-1324.
- Ljungberg, EAU Guidelines on Renal Cell Carcinoma. 2020: https://uroweb.org/guideline/renal-cell-carcinoma.
- Makker V, et al: Lenvatinib Plus Pembrolizumab in Patients With Advanced Endometrial Cancer. J Clin Oncol, 2020. 38(26): 2981-2992.
- Motzer RJ, et al: Nivolumab versus everolimus in advanced renal cell carcinoma. N Engl J Med, 2015. 373(19): 1803-1813.
- Choueiri TK, et al: Cabozantinib versus everolimus in advanced renal cell carcinoma. N Engl J Med, 2015. 373(19): 1814-1823.
- Chung-Han L: Phase II trial of lenvatinib (LEN) plus pembrolizumab (PEMBRO) for disease progression after PD-1/PD-L1 immune checkpoint inhibitor (ICI) in metastatic clear cell renal cell carcinoma (mccRCC). 2020: Journal of Clinical Oncology.
- Bonaca MP, et al: Myocarditis in the Setting of Cancer Therapeutics: Proposed Case Definitions for Emerging Clinical Syndromes in Cardio-Oncology. Circulation, 2019. 140(2): 80-91.
- Astaras C, et al: Neurological Adverse Events Associated with Immune Checkpoint Inhibitors: Diagnosis and Management. Curr Neurol Neurosci Rep, 2018. 18(1): 3.
- Cella D, et al: Patient-reported outcomes of patients with advanced renal cell carcinoma treated with nivolumab plus ipilimumab versus sunitinib (CheckMate 214): a randomised, phase 3 trial. Lancet Oncol, 2019. 20(2): 297-310.
- https://oraletumortherapie.ch.
- Rini BI, et al: Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): a multicentre, open-label, phase 3, randomised controlled trial. Lancet, 2019. 393(10189): 2404-2415.
- McDermott DF, et al: Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat Med, 2018. 24(6): 749-757.
- Heng DY: ASCO 2020.
InFo ONCOLOGY & HEMATOLOGY 2020; 8(6): 6-9.