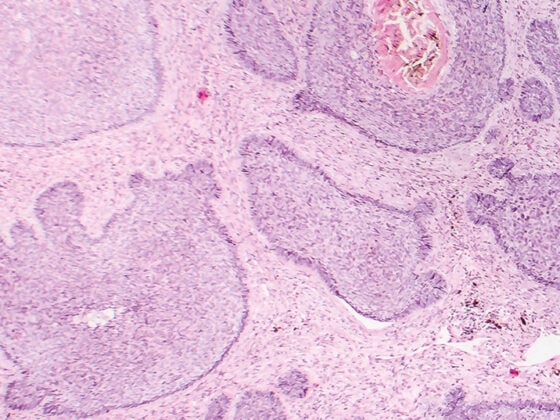
Benign adipose-derived tumors from mature adipocytes are among the most common mesenchymal tumors, but are uncommon in cervical and intrathoracic soft tissues. Imaging reveals fat-equivalent density values in the smoothly confined mass on CT. On MRI, characteristic T1w and T2w sequences indicate tissue character. If a lipoma grows, malignancy (liposarcoma) should be considered.
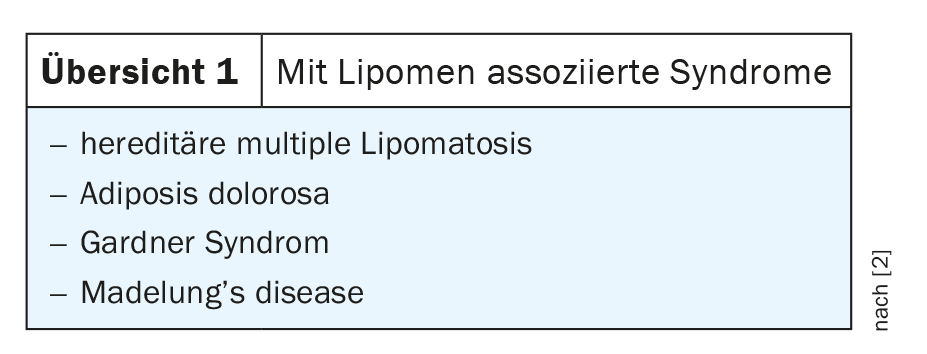
Lipomas are adipose tissue tumors, primarily occurring in subcutaneous tissue, but also in internal organs and rarely intracranially. Dominance is observed in the head and neck, shoulder area and back. Occasionally they are also found on the extremities. They can occur in all age groups, clinically manifest mainly between 40 and 60 years [2,3,5]. Men are affected slightly more often than women. Clinically, lipomas usually present as slow-growing, painless, and palpably mobile tumors with soft, doughy resistance. The average size varies between 2 and 10 cm. Lipomas may be associated with various syndromes (Overview 1).
Intrathoracic lipomas are relatively rare, and intracardiac lipomas, usually residing on the endocardium, are rarities [1]. Liposarcoma, which may present clinically like the benign variant, must be differentiated. Contrast-associated MRI is critical for differentiating tumor entities. In general, surgical excision is the treatment of choice in cases of growth progression, even in cases of image morphological suspicion of degeneration.
Radiographs cannot directly detect lipomas or distinguish between benign and malignant variants. However, above a certain size and depending on their location, the space-occupying effect, for example with displacement and/or impression of the trachea and esophagus, may be apparent.
Sonographically, the superficially located lipomas in particular are easy to identify.
Computed tomographic examinations can detect lipomas well. Measurement of hypodense tissue density shows typical values in the negative range of the Hounsfield scale. The contour is smooth, occasionally delicate connective tissue septa are visible.
Magnetic resonance imaging can also reliably identify the lipoma in the corresponding sequences if the tissue signal is hyperintense in T1 and T2 sequences. Tender fibrous septa may be present, and a tender capsule is also occasionally delineable hypointensely. In principle, MRI is the imaging study of choice for the differentiation of soft tissue tumors [4]. The synopsis of the different sequences (T1w and T2w hyperintense, in fatty suppression hypointense) clearly indicates tissue character. After intravenous application of Gd-DTPA, benign uncomplicated lipoma shows no signal increase.
Case studies
The first case report demonstrates a relatively large lipoma (approximately 10 × 3.5 cm, measured on axial scan), in a 37-year-old female patient with progressive retrosternal pressure and lumpiness. Already sonographically (Fig. 1A) , a large lipoma was conspicuous on thyroid examination, confirmed by subsequent MRI (Fig. 1B-E). The homogeneous lipoma-equivalent signal did not show any malignoma-specific enhancement even in the contrast-enhanced measurements. The mass was retrothyroidally extended into the upper mediastinum and had a smooth contour.

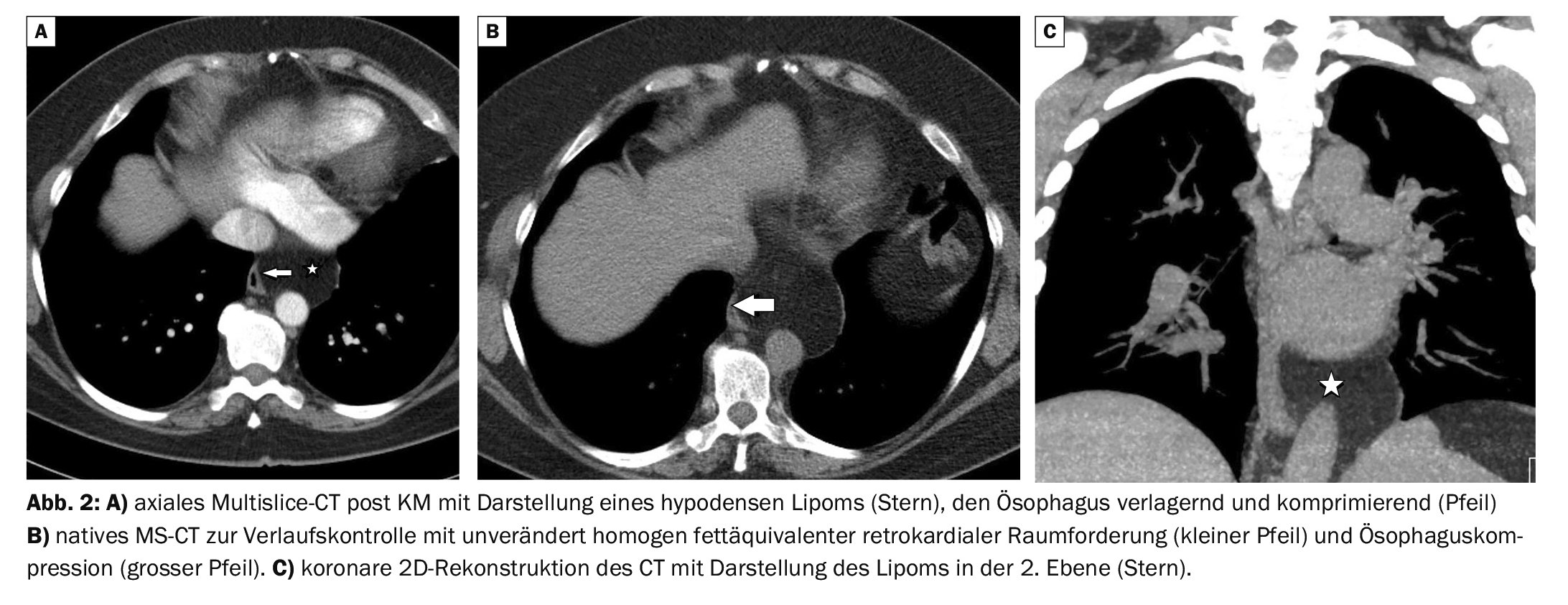
In case report 2, a retrocardiac lipoma of the thorax was detected in a 53-year-old female patient with dysphagia, resulting in compression and displacement of the esophagus to the right (Fig. 2A-C) . Follow-up of the findings after 6 months showed a trend of unchanged findings on multisclice CT, which was then performed natively. There was no evidence of malignant degeneration.
Take-Home Messages
- Lipomas are fatty tissue space-occupying lesions.
- They grow with smooth contour displacing with different symptomatology depending on the size and location.
- Magnetic resonance imaging is the method of choice for imaging and differentiation of tumor entity.
- If there are signs of environmental infiltration and portions with signal increase in the MRI examination with contrast medium, malignant degeneration must be assumed.
Literature:
- Burgener FA, et al: Differential diagnostics in MRI. Georg Thieme Verlag, Stuttgart, New York 2002: 486.
- Gohar AS: Lipoma excision. Am Fam Physician 2002; 65(5): 901-904.
- Grassmeier N. Lipoma. www.netdoktor.de/krankheiten/lipom. 2021 Nov.
- Johnson CN, et al: Lipomatous soft-tissue tumors. J Am Acad Orthop Surg 2018; 26(22): 779-788.
- Kosztyuova T, Shim TN: Rapidly enlarging lipoma. BMJ Case Rep. 2017 Sep 23; 2017.
HAUSARZT PRAXIS 2022; 17(12): 40-41
InFo ONCOLOGY & HEMATOLOGY 2022; 10(6): 32-33.