
Epidemiologic evidence suggests that respiratory syncytial virus (RSV) may have similar effects to non-pandemic influenza in older adults. Dutch researchers have investigated the extent to which RSV seasonality and latitude/region of residence may play a role in the spread of the virus and infection control.
An infection with the RS virus can be dangerous for older people, people with cardiopulmonary diseases and immunocompromised people, and the clinical symptoms are sometimes difficult to distinguish from those of influenza: In older people, they vary greatly and range from a mild cold to severe shortness of breath. However, the diagnosis of RSV infection in adults is difficult as the virus culture and antigen detection are insensitive, which is probably due to the low virus titers in nasal secretions; however, early bronchoscopy is useful in immunocompromised patients.
Four methods for diagnosis
The four most important methods for diagnosing RSV infection in adults are culture, antigen detection by immunofluorescence assay (IFA) or enzyme immunoassay (EIA), RNA detection by reverse transcription PCR (RT-PCR) and serological detection of RSV-specific IgM in the acute stage or by a significant increase in RSV-specific IgG antibodies between the acute and convalescent phases. The latter method only provides a retrospective diagnosis.
The culture is considered the standard against which all other methods are measured. In infants, it is highly sensitive and specific. Since adults excrete much less virus than infants (≤103 versus ≤106 PFU/ml) and the duration of infection is shorter (about 3 to 4 days), culture is not likely to be as sensitive in this population. The thermolability of RSV makes culture detection difficult, and most researchers have relied on serology for diagnosis in adults.
Detection of RSV antigens in respiratory secretions by IFA or EIA, methods with a sensitivity of 75 to 95% in infants, are even less useful than cultures in older adults.
Various serologic methods, including complement fixation reaction and EIA, have been used to diagnose RSV infection in adults with variable results. In an early study in a nursing home, an IgG EIA with purified F and G glycoproteins was positive in 85% of culture-positive individuals [1]. Consistently high titers were seen in the seronegative infections, which may indicate that the disease existed for several days prior to collection of the acute phase sera, which may have masked an increase in titer.
RT-PCR has been described as a useful diagnostic tool in infants, but there are no published reports for adults. In an analysis of 30 serologically confirmed RSV infections in adults, RT-PCR was positive in 12 of 13 (92%) culture-positive samples, also detected seropositive disease in 7 of 17 culture-negative samples, and was negative in all 20 culture-negative, seronegative samples.
Correlation between RSV activity and latitude?
Transmission of RSV requires close person-to-person contact or contact with contaminated surfaces in the environment as well as autoinoculation. To limit the spread of nosocomial RSV, various infection control strategies, especially hand washing, have been used. Masks are not justified in the control of RSV as transmission is not aerosolized and common masks only cover one potential route of autoinoculation, the nose. The use of eye-nose protection has been shown to limit the spread of RSV, but this is rarely implemented in everyday life. It is also recommended that infected patients be isolated and grouped together if possible.
Effective prevention and control of RSV requires a better understanding of the seasonality of this virus.
An international research group led by Lisa Staadegaard from the Netherlands Institute for Health Services Research (Nivel) in Utrecht, the Netherlands, conducted a study in which they analyzed the seasonality of RSV using a uniform method in a cross-national dataset of virologically confirmed surveillance data.
The GERi study provided data from 12 countries worldwide, resulting in a total of 501,425 RSV cases from 210 seasons (131 of which were subnational) [2].
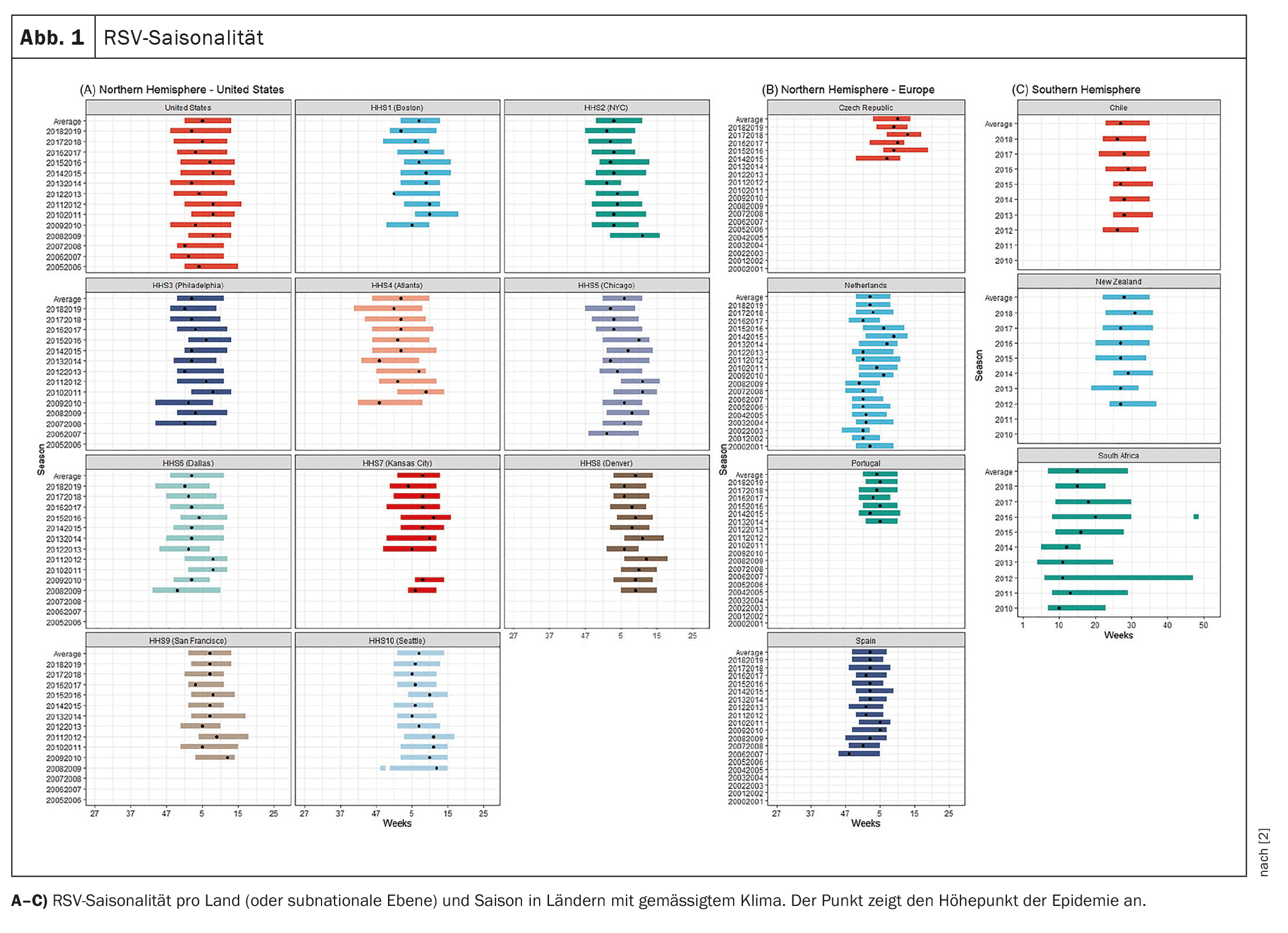
In most temperate countries, RSV epidemics occurred in winter and lasted a median of 10-21 weeks.
Not all outbreaks consistently followed this pattern, and some occurred later or at irregular intervals, the researchers emphasize.
Greater differences in timing were observed in (sub)tropical countries.
In addition, significant differences in seasonality were observed at the sub-national level.
The results also suggest that the predominant RSV subtype has a limited influence on the seasonality of RSV.
According to Staadegaard et al. the results largely confirm previous studies that have shown consistent annual RSV epidemics in temperate climates during the winter months and less consistent epidemics in the (sub)tropics. In addition, these studies found a correlation between RSV seasonality and the latitude and longitude of a country. In most cases, a positive correlation was found with latitude, as the peak of RSV activity in both the northern and southern hemispheres generally occurs later in the year and with further latitude. One region where this is not the case is Europe, where three different studies have come to contradictory conclusions. One study found a positive association between latitude and RSV activity, another found that the epidemic is shifting from several northern European cities (e.g. Helsinki and Stockholm) to the south (as well as further north), and a third found no association. In the latter study, however, it was found that RSV epidemics occur later in the east than in the west (i.e. a longitudinal relationship).
The positive association between latitude and RSV seasonality is largely confirmed in this analysis, but some exceptions were noted, as the authors emphasized. In the United States, RSV activity appears to begin in the southernmost region (HHS4), with a later onset in higher latitudes (e.g., HHS 1, 8, or 10) (Fig. 1A). However, not all HHS regions fit this pattern perfectly, as shown by the relatively late onset in HHS9 (San Francisco). In Europe, one would have expected the data to show the earliest RSV peak in Portugal, followed by Spain, the Czech Republic and finally the Netherlands – but this was generally not the case (Fig. 1B). The longitudinal association described above could explain the later onset of the RSV epidemic in the Czech Republic compared to the results for other European countries.
In the Southern Hemisphere, the results were largely consistent with the hypothesis that there is a correlation between RSV activity and latitude, as peak activity occurred first in (sub)tropical countries (Ecuador and Brazil), followed by temperate countries (Chile and New Zealand). An exception was South Africa, which is located in the same hemisphere and climate zone as Chile, but where RSV epidemics tended to start much earlier (the median onset in Chile was week 23 compared to week 8 in South Africa) (Fig. 1C). In addition, the results showed that the end and thus the duration of the epidemics in South Africa apparently fluctuate more strongly. Both factors are considered rather atypical for a country with a temperate climate.
The issue of RSV seasonality is important to ensure optimal timing of prevention and control measures. Therefore, it is crucial to standardize the methods used to define seasonality and to better understand RSV seasonality at the (sub)country level worldwide. This is important as previous generalizations about influenza seasonality have led to suboptimal vaccination strategies, which would be particularly problematic in the case of RSV as the administration of prophylaxis is often more time-dependent or requires multiple doses during the RSV season. Greater awareness of the timing of RSV epidemics could therefore ensure that optimal levels of protection are achieved in a cost-effective manner, the authors say.
Literature:
- Falsey AR, Treanor JJ, Betts RF, Walsh EE: Viral respiratory infections in the institutionalized elderly: clinical and epidemiologic findings. J Am Geriatr Soc 1992; 40: 115-119.
- Staadegaard L, Caini S, Wangchuk S, et al: Defining the seasonality of respiratory syncytial virus around the world: National and subnational surveillance data from 12 countries. Influenza and Other Respiratory Viruses 2021; 15: 732-741; doi: 10.1111/irv.12885.
FAMILY PHYSICIAN PRACTICE 2024; 19(8): 52-53









