
Cystadenomas are benign epithelial tumors that grow like glands and form cysts. Mature teratomas of the ovary are benign neoplasms from various cotyledons and can exhibit different phenotypes. Cystadenomas often lead to a feeling of abdominal pressure and teratomas are not always asymptomatic. Imaging procedures such as ultrasound, CT or MRI are helpful for the diagnosis.
Benign changes of the uterus and ovary have already been described in the previous articles. Benign ovarian neoplasms also include serous or mucinous cystadenomas, granulosa cell tumors and arrhenoblastomas [1].
Cystadenomas are usually unilocularly growing masses. They can reach a considerable size with typically slow growth and only cause symptoms at a late stage. Postmenopausal women are then often symptomatic. A significant increase in abdominal circumference and a feeling of abdominal pressure are noteworthy, but the picture of an acute abdomen is rather rare. Due to the size of the findings, sonography is usually supplemented by computer tomography or magnetic resonance imaging in order to assess the full extent of the tumors. Adnexectomy should be performed in postmenopausal patients. Complete tumor removal is also necessary, as otherwise there is a risk of recurrence [2].
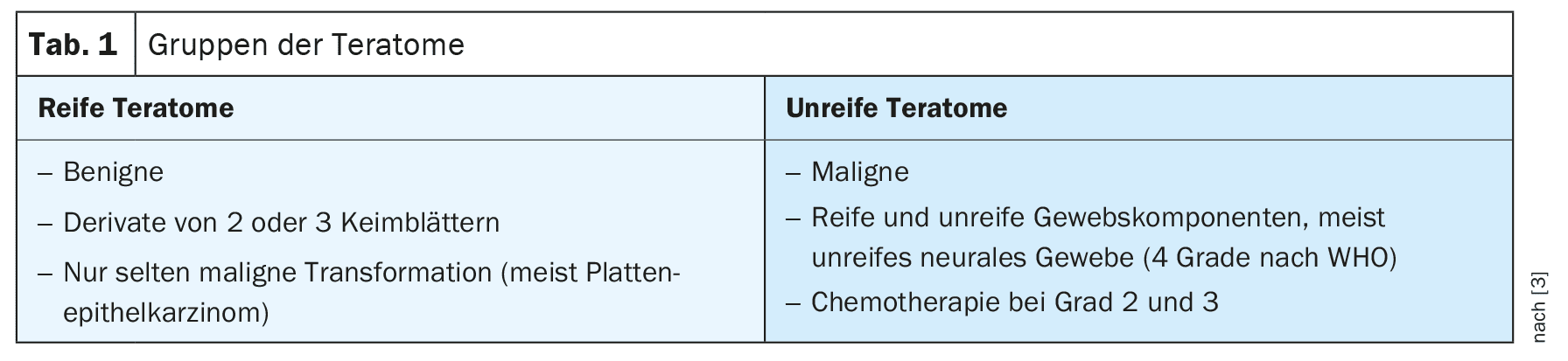
Teratomas are often found in women of childbearing age, including children and infants. They are primarily benign tumors, and the degeneration rate is relatively low at less than 3% [1,4]. Men can also develop teratomas, but less frequently than women. However, they are more likely to be affected by immature teratomas. The distribution pattern of teratomas can be seen in Figure 1 . Teratomas consist of all three germ cell layers. Solid and cystic parts are present, calcifications or abortive teeth and bone components are typical, hair is also found. Usually asymptomatic, symptoms of an acute abdomen can occur in the event of stem rotation or rupture. Two large groups of teratomas (Table 1) can be distinguished [3].
In the case of mature teratomas in women, a distinction is made between dermoid cysts, the most common ovarian tumor in childhood, and struma ovarii. These are primarily benign changes with a very low risk of degeneration. If hyperthyroidism is diagnosed and the thyroid gland is unremarkable, thyroxine production in the struma ovarii should always be considered [4].
Complete resection is the treatment of choice for mature teratomas. Treatment of the immature form corresponds to that of ovarian cancer with surgery and, depending on the stage, polychemotherapy.
Sonographically, the diagnosis of a teratoma is usually an incidental finding. The ultrasound image is determined by the complex composition of different tissue components. Histological clarification should always be carried out, as the morphological differentiation between the mature and immature form is not clear from an image diagnosis.
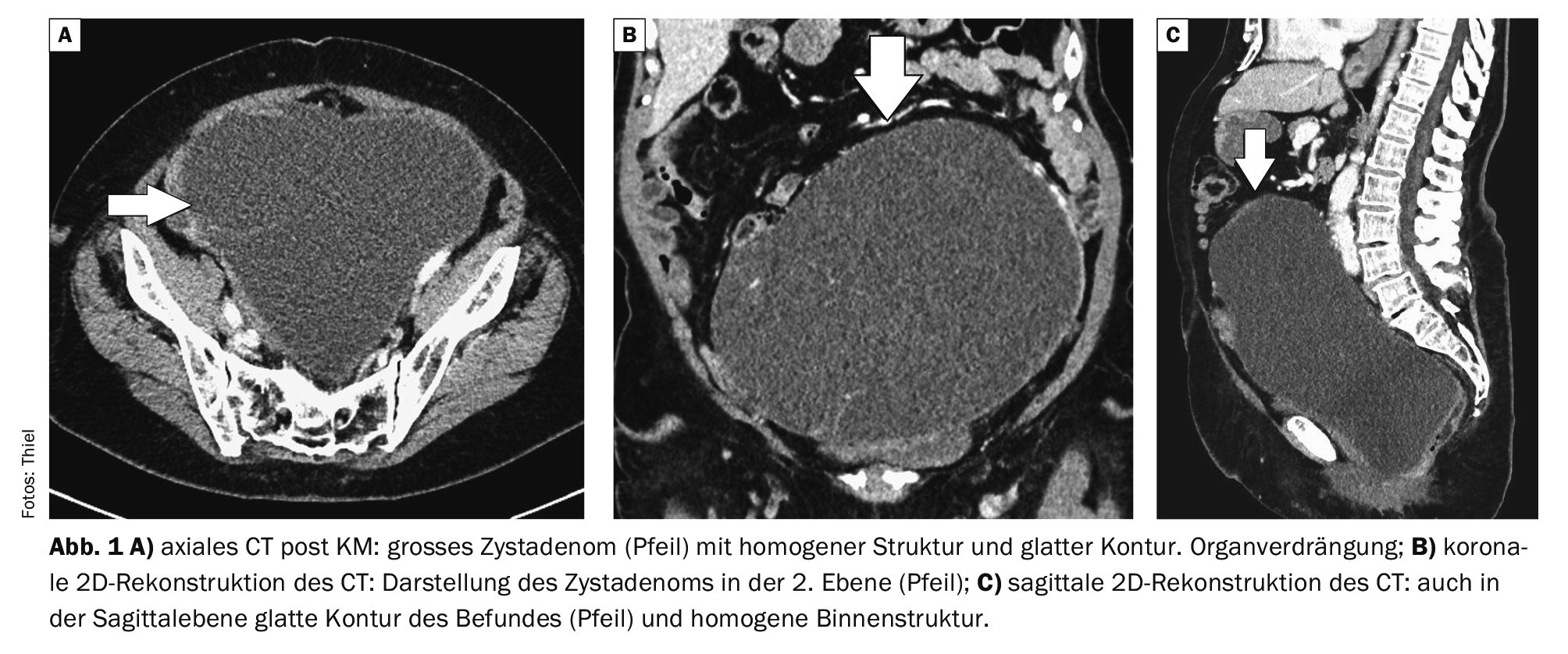
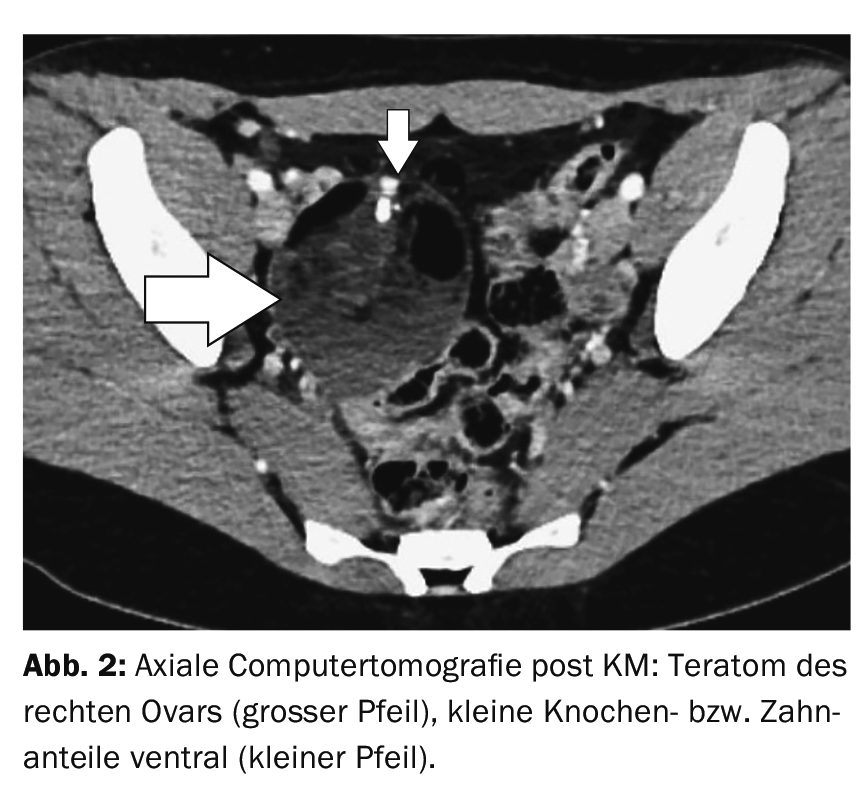
The full extent of the masses can be determined using computer tomography. The sometimes considerable organ displacement by the cystadenomas is documented in the multiplanar reconstruction. The teratomas can be differentiated by the different tissue proportions and the teeth and bone parts in particular can be identified as such by density quantification.
Magnetic resonance imaging enables the reliable differentiation of various soft tissues, and the administration of contrast medium allows the visualization of accompanying inflammatory complications or tissue necrosis.
Case studies
In case example 1 (Fig. 1A to 1C), a large cystadenoma can be seen in the CT scan of a 52-year-old female patient. In addition to a small increase in circumference, there was a feeling of abdominal pressure and an increased urge to urinate. The mass led to a considerable displacement of the adjacent bowel loops and to a considerable compression of the urinary bladder.
Case 2 demonstrates a teratoma of the right ovary in a 25-year-old female patient (Fig. 2). The suspected diagnosis was made by sonography during a pelvic examination. Heterogeneous internal structure, including tooth and bone material in the ventral part of the mass.
Case 3 shows a cystic solid tumor of the left ovary in a 71-year-old female patient with left lower abdominal pain on CT examination (Fig. 3), approx. 9 cm in diameter. Morphologically, the findings were compatible with a cystadenocarcinoma.

Case 4 shows a large intrapelvic teratoma on MRI in a 47-year-old female patient with Lynch syndrome (Fig. 4) with considerable displacement of the uterus to the right and compression of the urinary bladder.

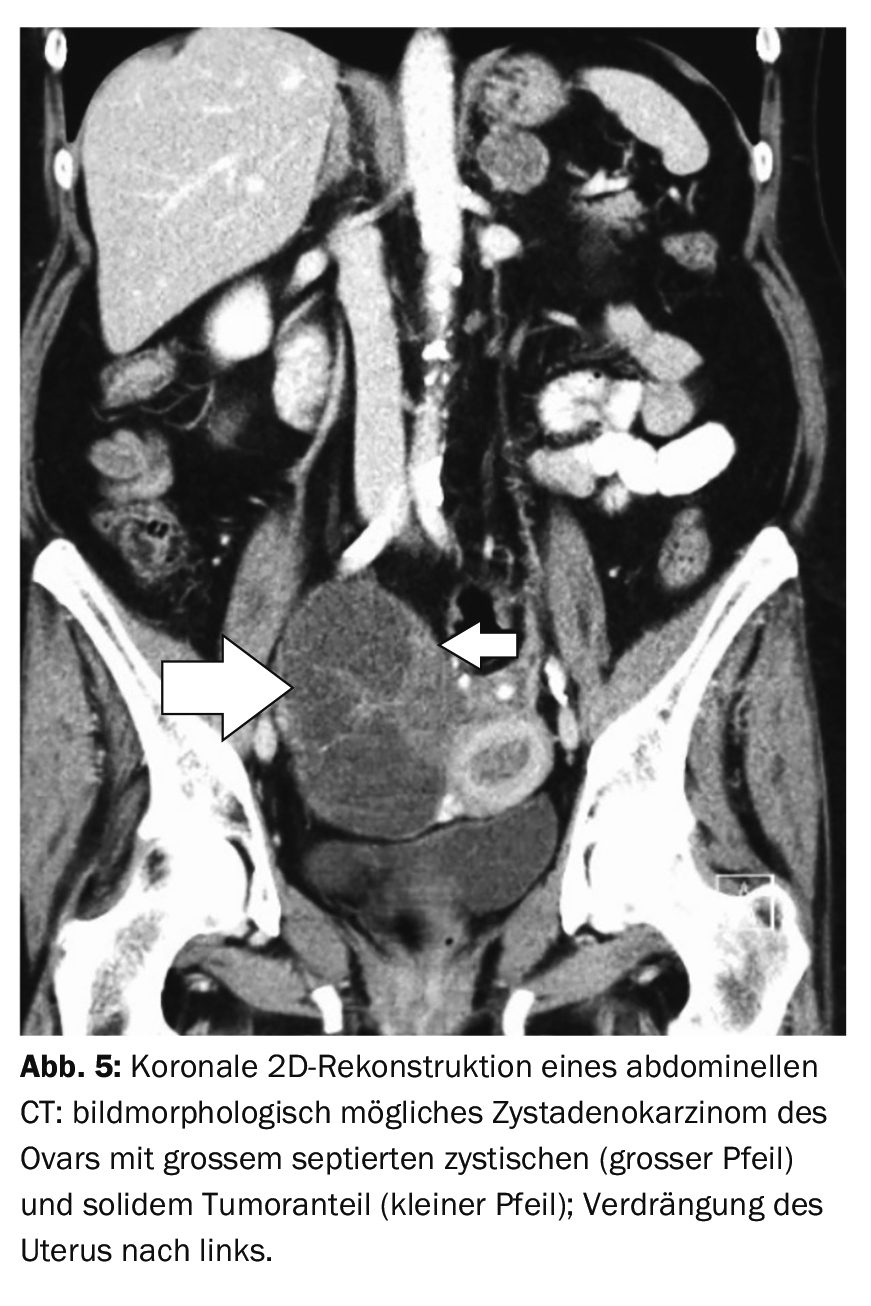
In case 5, a 62-year-old female patient with vaginal bleeding for 14 days had a suspicious cystic finding of the right ovary on preoperative sonography. Abdominal computed tomography revealed an 11 cm cystic solid tumor (Fig. 5). A cystadenocarcinoma could not be ruled out.
Take-Home-Messages
- Teratomas and cystadenomas usually show a typical image on cross-sectional examination and are easy to distinguish from simple ovarian cysts.
- The malignant variants often cannot be clearly identified, so surgical treatment should always be carried out.
- The often considerable size of the masses can result in displacement of the neighboring organs and an increase in the circumference of the abdomen.
Literature:
- Burgener FA, Meyers SP, Tan RK, Zaunbauer W: Differential diagnosis in MRI. Georg Thieme Verlag Stuttgart, New York: 2002; pp. 626.
- “Cystadenomas”, www.med-specialists.com/behandlungen/zystadenome,(last accessed 15.08.2023).
- Kamp D, van den Höfel N: Teratoma. https://flexikon.doccheck.com/de/Teratom,(last accessed 02.07.2024).
- Schmidt D, Kommoss F. Teratomas of the ovary. The Pathologist 2007; 28: 203-208.
FAMILY PHYSICIAN PRACTICE 2024; 19(9): 46-48









