
Inflammatory rheumatic diseases can potentially cause severe joint and organ damage without (adequate) therapy. The capacity of specialized centers and specialists is far from sufficient to treat all patients in a timely manner. One possible solution could be early or screening consultations.
In clinical and practical everyday life there is a high demand for at least one rheumatological clarification. Approximately one quarter of the population has at least intermittent chronic or acute musculoskeletal symptoms that could be differentially diagnosed as rheumatic. The prevalence of adults with ongoing rheumatology care needs is 2%. However, the capacities in rheumatology do not allow this, especially the acute need for clarification cannot be covered well. For rheumatoid arthritis (RA), it is recommended that the patient be evaluated rheumatologically within 3-6 months after the onset of symptoms and that therapy be initiated.
However, the reality in many regions is quite different: In Germany, the waiting time for the first rheumatology appointment from request alone is about 6 months in many places. In Switzerland, the situation is not much different. In addition, there is the time that the patient waits before presenting to the primary care provider with his or her complaints, plus the time that the primary care provider then needs to identify the need for rheumatological clarification.
A look at the ratio of rheumatology capacity to need is sobering: only about half of the rheumatologists needed are actually available. Such a gap cannot be closed in the short term. Possible solutions to eliminate this bottleneck may lie, for example, in reorganizing existing capacities and access routes. Early or screening consultations are one approach to this. Dr. Karolina Benesova from Heidelberg University Hospital (D) presented the screening consultation “SCREENED” (SCREEN for Early Diagnosis), which has been offered at her hospital since 2018 as a tool for early diagnosis and therapy of inflammatory rheumatic diseases [1].
Early intervention = economic advantage
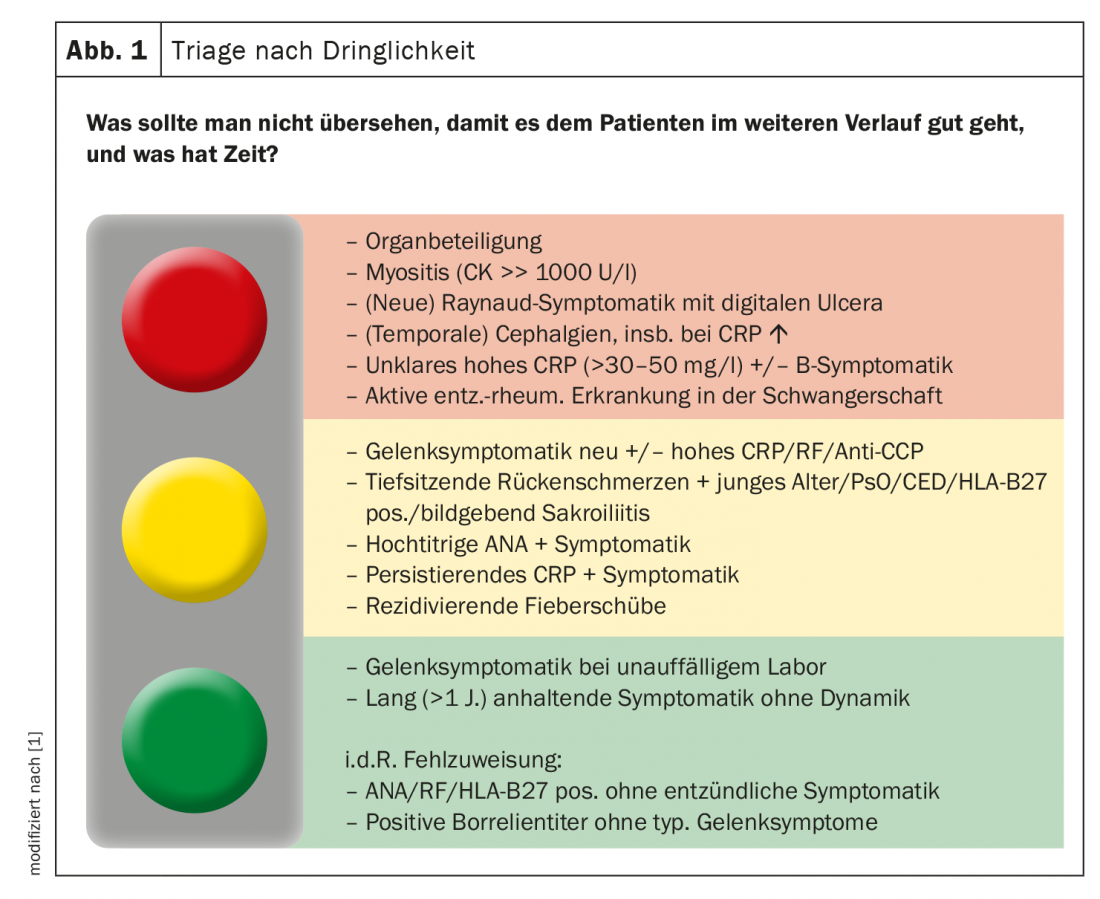
The consultation offers capacity for approximately 12 patient appointments per week on-site in Heidelberg. The doctor-patient contact is 30 minutes each time. The time from the request to the appointment is 7-60 days depending on the urgency. The basis and also the prerequisite for being admitted to the consultation is first a standardized patient questionnaire, which the patient submits with the referring physician. After a formal check for completeness of the documents, they are reviewed by a rheumatologist, who makes an initial tentative diagnosis and defines the urgency on the basis of this (Fig. 1) . The regional care goals of SCREENED are to shorten the waiting time for initial rheumatological clarification, but also to ensure transparent processes that are as timely and standardized as possible. In addition, communication with patients and referring physicians is to be optimized so that waiting times can also be reduced in primary care. In addition, there are overarching goals, which include improving the quality of rheumatologic care regionally and nationally by sharing information with other early intervention centers.
Dr. Benesova highlighted that initial presentation within the required 3-6 months currently reaches only about one-third of RA patients and one-fifth of PsA patients. “Around a third of RA patients and around half of PsA sufferers have already been ill for more than a year before they first contact us.” This is significant not least because, according to evaluations in Heidelberg, patients who achieve remission are ill for an average of about 100 weeks before they present for the first time. The disease duration in patients who did not achieve remission was in a min. 2-year follow-up period, on the other hand, was about twice as long. “Rheumatology is cost-intensive. However, we have been able to show that patients who are treated earlier have less need for biologics and targeted DMARDs in the further course,” the expert stated.
Regarding the question of what not to overlook in order for the patient to do well down the road, Dr. Benesova presented some casuistry from her screening clinic to illustrate that often you don’t need that much information to decide if you need to see a patient and if so, how soon.
1. particularly urgent need for clarification
-> Decision within 1 week, inpatient admission if necessary.
Case report: 31-year-old patient without significant preexisting conditions. In this case, the call came from the orthopedics department of the UK Heidelberg: The man had severely swollen ankles, pressure-dolent skin lesions on the legs, and a fever of 38.3 °C. CRP was 91 mg/l.
Fever and CRP alone should be red flags here, the rheumatologist noted. Photographs sent on request also showed typical erythema nodosa, which was very painful on pressure. In the questionnaire, the man stated that the pain was 8 out of 10 on a scale at the beginning and that, according to subjective perception, the ankle and knee were the affected joints. Symptomatically, he had stated, among other things, shortness of breath, but also cough.
Recommendation: The physicians recommended to their colleagues from orthopedics to complete the diagnostic workup (sCD25, ACE as a follow-up parameter, chest x-ray in case of a possible acute sarcoidosis (Löfgren), and to start a 30 mg prednisone therapy until the appointment in 10 days. The laboratory showed that sCD25 was significantly elevated with >2100 U/ml (<900), ACE was normal. X-ray confirmed the v.a. peripheral lymphadenopathy.
Course: The further course was encouraging: already at the presentation appointment after 10 days, a clear improvement was observed under the steroid shot, there was no more OSG arthritis, and the erythema nodosa faded away. The cough was clearly regressing and the patient no longer had a fever.
Nevertheless, Prof. Dr. Clemens Cohen, Munich Clinic Harlaching and scientific director of the Rheuma Nephro Refresher, from the online plenary, took issue with this and asked whether this patient should not have been seen rheumatologically immediately? His main concern was that with immediate steroid administration, differential diagnoses such as septic arthritis could have been missed. Dr. Benesova quite agreed with his colleague. In this case, however, the case had been so clear – also with the skin changes and the fact that the orthopedic colleagues had examined the patient on site – that she had called her bluff. “But if it had been a patient I didn’t know anything else about and didn’t have images or labs, that would have been a candidate to admit as an inpatient if necessary.”
2. urgent need for clarification
-> Decision within 4 weeks
Case history: A 71-year-old female patient without significant preexisting medical conditions had only been symptomatic for approximately 2 weeks with pain and swelling in her fingers/wrist and shoulders. She subjectively reported a typical RA pattern, with a DAS28 of 6.1 at initial presentation. CRP was 21.4, CCP positive, rheumatoid factor elevated (21), and SS-A positive (93.00). So overall, a clear indication that this patient needs to be seen and cared for rheumatologically.
Recommendation: The Heidelberg experts made the diagnosis of seropositive, anti-CCP-positive rheumatoid arthritis. Therapeutically, a steroid regimen of prednisone 30mg and MTX 15 mg/week s.c. was initiated.
Course: Again, a positive course was observed: After 4 months, the patient was in remission on only 5 mg prednisone.
3. less urgent need for clarification
Patients who have been ill for a long time and whose symptoms are not dynamic, or patients who have joint symptoms but with an inconspicuous laboratory, especially if it is only pain without swelling, should of course be clarified. However, there is no particular urgency for this, as Dr. Benesova summed up.
– FomF Rheumatism Nephro Refresher (online), Oct. 29-31, 2020.
Source:
- Industry symposium “SCREENED to target: who needs to see a rheumatologist and when?”, 10/29/2020, Janssen-Cilag.
InFo PAIN & GERIATRY 2020; 2(2): 34-35 (published 11/12/20, ahead of print).









