
A new study provides insights into the mechanisms of resistance in triple-negative breast carcinoma (TNBC) and therapy with CDK4/6 inhibitors. Previously known from the treatment regimen of advanced hormone receptor (HR)-positive, HER2-negative breast cancer, a subtype of TNBC also shows sensitivity in this preclinical study.
Breast carcinoma is the most common malignant tumor in women. Statistically, 112/100,000 women per year in Switzerland develop breast carcinoma, making this cancer the highest incidence of all malignancies in women in Switzerland [1].
At the same time, breast carcinoma is also responsible for the highest carcinoma-related mortality in women at 18.9% [2]. The therapy regime differs depending on the stage of the disease the patient is in. In metastatic findings, the goal of therapy often shifts. The focus is then on palliative measures, maintaining a good quality of life and prolonging survival as far as possible without progression.
In breast carcinoma, the characteristics of the tumor at each stage of the disease play a decisive role in optimal therapy. Among many other classifications, breast carcinoma has been subdivided into different molecular genetic subtypes since the seminal work of Perou and Sorlie [3]. If hormone receptor (HR) status, HER2 status and proliferation index (Ki-67) are included, the following classification is found:
- Luminal A-like type (HR-positive, HER2-negative, Ki-67 low),
- Luminal-B-like type (HR-positive, HER2-negative, Ki-67 high),
- HER2-type non-luminal (HR-negative, HER2-positive) and
- triple-negative/basal-like type (HR-negative, HER2-negative)
This latter subdivision also simultaneously indicates a certain predictive value with regard to the response to various therapeutic concepts and thus with regard to prognosis. For luminal or hormone receptor-positive, HER2-negative breast cancer, an effective therapy in terms of progression-free survival in locally advanced or metastatic breast cancer exists in the form of palbociclib – a CDK 4/6 inhibitor – in combination with endocrine therapy. The drug interferes with the complex regulatory mechanisms of the cell cycle through cyclins and their cyclin-dependent kinases (CDK). Dysregulations in this system, e.g. by inactivation of a tumor suppressor protein, are key events in the development of carcinomas.
Clinical practice has shown that the complexity of cell cycle regulation requires constant adaptation of therapeutic solutions. During the course of therapy with the above-mentioned palbociclib, a development of resistance was demonstrated, which can be circumvented with simultaneous administration of a phosphoinositide 3-kinase (PI3K) inhibitor (e.g. ribociclib) from the beginning. According to the data available to date, the development of resistance that has already taken place cannot be reversed [4]. It is therefore of great interest to understand the exact mechanisms of resistance development in order to develop potential targets for future therapies. Equally significant is finding targeted therapies for advanced triple-negative breast carcinoma (TNBC). The prognosis here is much worse compared to luminal breast carcinoma [5].
Mechanisms of resistance and treatment option in triple-negative breast carcinoma.
To gain further insight into the mechanisms of resistance in triple-negative breast carcinoma, Asghar et al. both in vitro and in vivo the mode of action of palbociclib tlw. in combination with taselisib was investigated, working here with xenotransplanted mice [6]. A subset of TNBC, the luminal androgen receptor positive subtype, was found to be highly sensitive to palbociclib administration compared to the basal-like subtype (p<0.001). This result seen in vitro was confirmed in vivo with seven partial remissions (decrease in tumor size, n=10 palbociclib 50 mg/kg; n=10 vehicle). Similarly, a decreased level of phosphorylated retinoblastoma protein (pRb), a tumor suppressor protein crucial for cell cycle regulation in its active – i.e., non-phosphorylated – form, was shown.
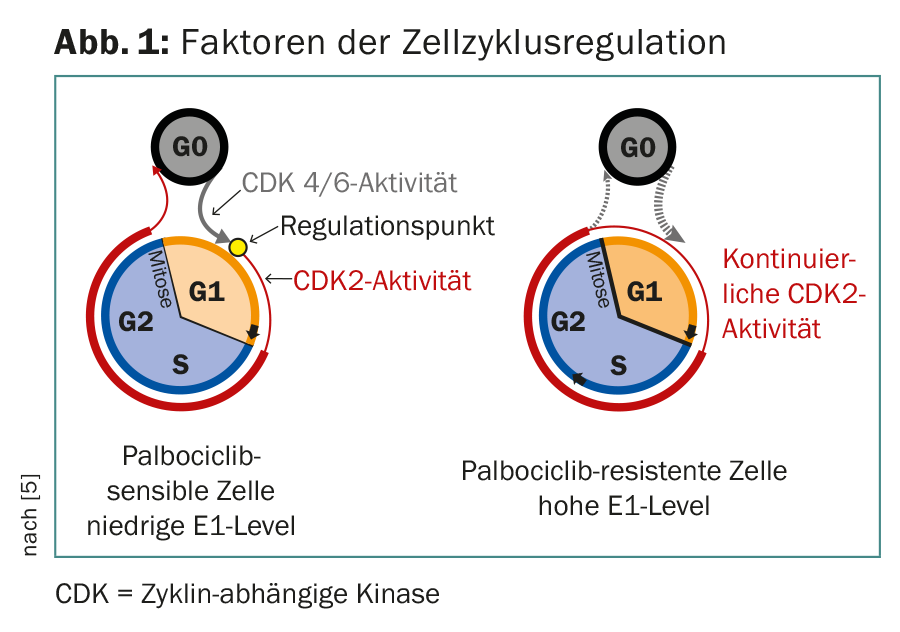
Cells sensitive to palbociclib were in a quiescent state with respect to CDK2 activity and were dependent on CDK4/6 for cell cycle initiation. The cells that were resistant to palbociclib were already in a proliferation stage with high CDK2 activity after mitosis and were thus able to bypass the regulatory point of CDK4/6 kinase, with rapid transformation to S phase and shorter cell cycles (Fig.1). These resistant cells showed equally increased levels of cyclin E1 (p=0.094) during early G1 phase compared to the sensitive ones, the silencing of which led to sensitization of the cell to palbociclib. In the presence of a PIK3CA mutation, a synergistic effect was also demonstrated in the combination of CDK4/6 and PI3K inhibitors.
Thus, cyclin E1 may be one of the key factors in the context of resistance formation in CDK4/6 inhibition. An ongoing clinical trial is expected to provide further insight into therapeutic options for CDK4/6 inhibitors in TNBC.
Take-Home Messages
The IMPAKT Breast Cancer Conference was held in Brussels in May 2017. One focus of the event was the topic of resistance formation in drug therapy for breast carcinoma and further research into the possible circumvention of this very resistance. One of the studies presented provided insights into the aforementioned mechanisms in triple-negative breast carcinoma (TNBC) and therapy with the CDK4/6 inhibitor palbociclib. Previously known from the treatment regimen of advanced hormone receptor (HR)-positive, HER2-negative breast cancer, a subtype of TNBC also shows sensitivity in this preclinical study.
Source: IMPAKT Breast Cancer Conference, May 4-6, 2017, Brussels.
Literature:
- Federal Statistical Office: Specific Cancer Diseases. 2016; www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitszustand/krankheiten/krebs/spezifische.html
- Krebsliga Schweiz: Cancer in Switzerland: important figures. 2016; www.krebsliga.ch/ueber-krebs/zahlen-fakten/dl/fileadmin/downloads/sheets/zahlen-krebs-in-der-schweiz.pdf
- Sørlie T, et al: Geneexpression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci 2001; 98: 10869-10874.
- Herrera-Abreu MT, et al: Early adaptation and acquired resistance to CDK4/6 inhibition in estrogen receptor-positive breast cancer. Cancer Res 2016; 76(8): 2301-2313.
- Rampurwala M, Wisinski KB, O’Regan R: Role of the androgen receptor in triple-negative breast cancer. Clin Adv Hematol Oncol 2016; 14(3): 186-193.
- Asghar U, et al: Unraveling mechanisms of resistance to CDK4/6 inhibitors using triple negative breast cancer (TNBC). Ann Oncol 2017; 28(1): mdx145.
InFo ONCOLOGY & HEMATOLOGY 2017; 5(3): 34-35.









