
Psoriasis is one of the most common inflammatory skin diseases. But it is only in the last thirty years that research in this field has become increasingly intensive. As it turned out, various comorbidities can accompany it and influence not only the course but also the treatment.
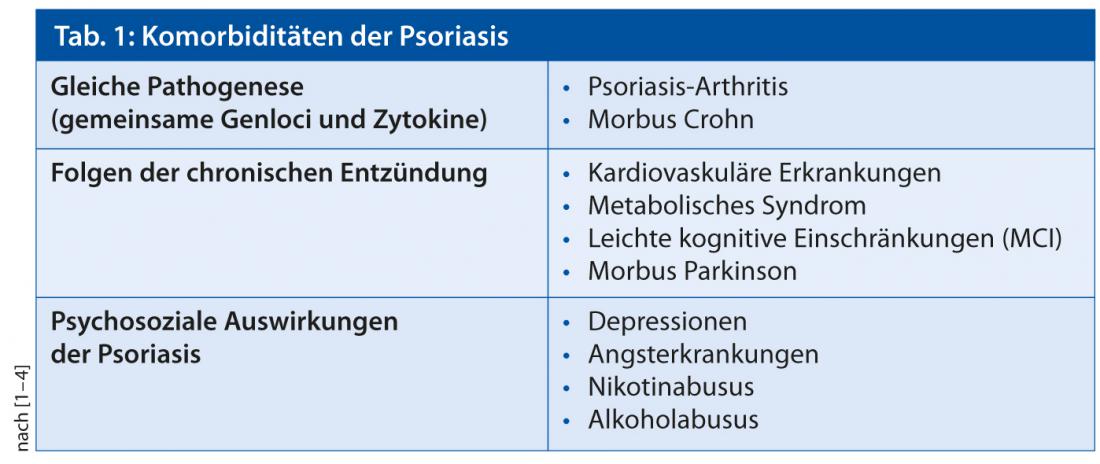
The growing knowledge about the pathogenesis of the disease not only led to tremendous progress in the treatment of psoriasis, it also showed that psoriasis is associated with a number of comorbidities that play an important role in the management of the disease,” said Prof. Giampiero Girolomoni, MD, Verona, at the SGDV Congress in Montreux (Tab. 1) [1–4].
Psoriatic Arthritis
Psoriatic arthritis affects approximately 10-40% of psoriatic patients. It usually occurs in the late 20s to 40s, in young patients, and usually after the first skin manifestations. Joint involvement usually begins oligoarticular, but over time can develop into severe polyarticular arthritis. The dermatologist plays a critical role in both the early diagnosis of psoriatic arthritis and the identification of patients with an aggressive form, as well as in identifying patients at increased risk for arthritis. Risk factors for the development of arthritis are: Obesity [5–8], smoking (especially in women) [9], psoriatic scalp involvement and intergluteal/perianal lesions [10], nail dystrophies [10] and subclinical enthesopathies (check quadriceps tendon thickness) [11, 12]. In addition to imaging techniques, various validated questionnaires are available for the diagnosis of arthritis.
Psoriasis and cardiovascular disease
Psoriatic patients have a significantly higher risk of developing metabolic syndrome than the normal population (OR 2.26; 95% CI 1.70-3.01), and the prevalence of metabolic syndrome correlates with the severity of psoriasis [13]. Regarding the risk of cardiovascular disease and stroke, only patients with severe psoriasis have a significantly increased risk (myocardial infarction: RR 3.04; 95% CI 0.65-14.35; cardiovascular mortality RR 1.37; 95% CI 1.17-1.60; stroke RR 1.59; 95% CI 1.34-1.89) [14]. “The question of whether psoriasis treatment can reduce cardiovascular risk is still controversial. However, in my opinion, there is more data in favor than against that the risk can be reduced with proper therapy,” Prof. Girolomoni opined. For example, in the Kaiser cohort, cardiovascular risk was significantly reduced by treatment with TNF inhibitors compared with topical treatment [15]. And in a Danish cohort, significantly fewer cardiovascular events occurred in patients treated with biologics or methotrexate than in those treated with other regimens [16].
Psoriasis and obesity
Obesity is the most important extracutaneous risk factor in psoriasis patients and severely affects treatment. Thus, patients with a high BMI have a poorer short-term response to systemic therapy [17]. Fixed-dose biologics such as etanercept, adalimumab, and ustekinumab may have limited efficacy in obese patients [18, 19]. Furthermore, obesity increases the risk of liver or renal toxicity with methotrexate and cyclosporine [20, 21]. “So could psoriasis patients benefit from weight loss?” the speaker asked. The answer: “Yes,” he said. Weight loss can significantly improve both treatment response and clinical symptoms [22, 23]. For these reasons, weight loss should definitely be targeted therapeutically.
Source: 95th Annual Meeting of the SGDV, September 19-21, 2013, Montreux.
Literature:
- Smith CH, Barker JN: Psoriasis and its management. BMJ 2006; 333: 380-384.
- Ludwig RJ, et al: Psoriasis: a possible risk factor for development of coronary artery calcification. Br J Dermatol 2007; 156: 271-276.
- Vena GA, et al: Can early treatment with biologicals modify the natural history of comorbidities? Dermatol Ther 2010; 23: 181-193.
- Menter A, et al: Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol 2008; 58: 826-850.
- Tam LS, et al: Cardiovascular risk profile of patients with psoriatic arthritis compared to controls – the role of inflammation. Rheumatology 2008; 47: 718-723.
- Bhole VM, et al: Differences in body mass index among individuals with PsA, psoriasis, RA and the general population. Rheumatology 2012; 51: 552-556.
- Soltani-Arabshahi R, et al: Obesity in early adulthood as a risk factor for psoriatic arthritis. Arch Dermatol 2010; 146: 721-726.
- Love TJ, et al: Obesity and the risk of psoriatic arthritis: a population-based study. Ann Rheum Dis 2012; 71: 1273-1277.
- Li W, et al: Smoking and risk of incident psoriatic arthritis in US women. Ann Rheum Dis 2012; 71: 804-808.
- Wilson FC, et al: Incidence and clinical predictors of psoriatic arthritis in patients with psoriasis: a population-based study. Arthritis Rheum 2009; 61: 233-239.
- Gisondi P, et al: Lower limb enthesopathy in patients with psoriasis without clinical signs of arthropathy: a hospital-based case-control study. Ann Rheum Dis 2008; 67: 26-30.
- Tinazzi I, et al: Preliminary evidence that subclinical enthesopathy may predict psoriatic arthritis in patients with psoriasis. J Rheumatol 2011; 38: 2691-2692.
- Armstrong AW, et al: Psoriasis and metabolic syndrome: a systematic review and meta-analysis of observational studies. J Am Acad Dermatol 2013; 68: 654-662.
- Samarasekera EJ, et al: Incidence of cardiovascular disease in individuals with psoriasis: a systematic review and meta-analysis. J Invest Dermatol 2013; 133: 2340-2346.
- Wu JJ, et al: Association between tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis. Arch Dermatol 2012; 148: 1244-1250.
- Ahlehoff O, et al: Cardiovascular disease event rates in patients with severe psoriasis treated with systemic anti-inflammatory drugs: a Danish real-world cohort study. J Intern Med 2013; 273: 197-204.
- Naldi L, et al: Impact of body mass index and obesity on clinical response to systemic treatment for psoriasis. Evidence from the Psocare project. Dermatology 2008; 217: 365-373.
- Clark L, Lebwohl M: The effect of weight on the efficacy of biologic therapy in patients with psoriasis. J Am Acad Dermatol 2008; 58: 443-446.
- Puig L: Obesity and psoriasis: body weight and body mass index influence the response to biological treatment. J Eur Acad Dermatol Venereol 2011; 25: 1007-1011.
- Rosenberg P, et al: Psoriasis patients with diabetes type 2 are at high risk of developing liver fibrosis during methotrexate treatment. J Hepatol 2007; 46: 1111-1118.
- Thaçi D, et al.: Body-weight-independent dosing of cyclosporine micro-emulsion and three times weekly maintenance regimen in severe psoriasis. A randomised study. Dermatology 2002; 205: 383-388.
- Gisondi P, et al: Weight loss improves the response of obese patients with moderate-to-severe chronic plaque psoriasis to low-dose cyclosporine therapy: a randomized, controlled, investigator-blinded clinical trial. Am J Clin Nutr 2008; 88: 1242-1247.
- Jensen P, et al: Effect of weight loss on the severity of psoriasis: a randomized clinical study. JAMA Dermatol 2013; 149: 795-801.
Dermatology Practice 2013, No. 5









