
Polyneuropathies are generalized diseases of the peripheral nervous system. With a prevalence of 5-8%, patients with chronic alcohol abuse, diabetes or malignant diseases are most affected. In addition to treatment of the causative disease, analgesics, antidepressants or anticonvulsants are mainly used to alleviate the symptoms.
In polyneuropathies (PNP), the motor, sensory and autonomic nerves all affect those parts of the nervous system that lie outside the central nervous system. Distal symmetric PNP is most common, starting in the legs, with a neuronal axonal length-dependent disease process as the causative factor. In addition, polyradiculoneuropathies with proximal and distal involvement or mononeuropathia multiplex with an asymmetric clinical picture may also occur. The pain that occurs in PNP results from damage or destruction of the nerve fibers, not from external stimuli such as inflammation or injury. Sensory stimuli are either not reported at all, reduced or increased to the brain. The first symptoms are often felt as discomfort such as tingling and burning. As it progresses, there is then a diminished perception of touch and pain. These false sensations can occur as false sensations of cold or heat or as sensations of pain in response to non-painful stimuli.
Consequence of other diseases
PNP is usually a consequence of other diseases, such as advanced diabetes. Diabetic neuropathy can be detected in nearly half of all type 2 diabetics. The increased blood sugar is held responsible, which damages the corresponding nerves. But there are other risk factors. In PNP caused by chronic alcohol abuse, the nerves are toxically damaged. The duration of abuse as well as the lifetime amount of alcohol play a role in the development. Chemotherapy-induced neuropathies are the most common neurologic side effect of tumor therapy. As malignancies have increased, the incidence is also rising. Neurotoxicity depends on the amount of the single dose, the total cumulative dose, and the duration of chemotherapy. However, other drugs and environmental toxins can also trigger PNP.
Guideline-based diagnostics and possible triggers
The S1 guideline “Diagnostics in Polyneuropathies” has also addressed other possible triggers and their management. These include, for example, drugs in oncology, the Zika virus and gene mutations. Immune checkpoint inhibitors in particular can cause neurological side effects, such as acute inflammatory demyelinating or axonal polyneuropathy (AIDP/ASMAN/AMAN) and chronic inflammatory demyelinating polyneuropathy (CIDP). However, organ transplantation, the hepatitis E and Zika viruses, the anti-FGF3 antibody, and mutations of the SCN9A, SCN10A, SCN11A (small fiber neuropathies) genes and the GLA gene can also cause different PNP.
Detect emergencies
Chronic PNP can usually be recognized by its symptoms. A physical examination, electromyography and measurement of nerve conduction, as well as blood and urine tests, then usually provide information about the underlying cause of the PNP. In addition, an expanded laboratory, CSF diagnostics, muscle/nerve/skin biopsy, genetics, and diagnostic imaging are recommended. Most importantly, neurological emergencies, such as Guillain-Barré syndrome or vasculitis, should be detected.
Consistent therapy of the underlying disease and effective symptom control
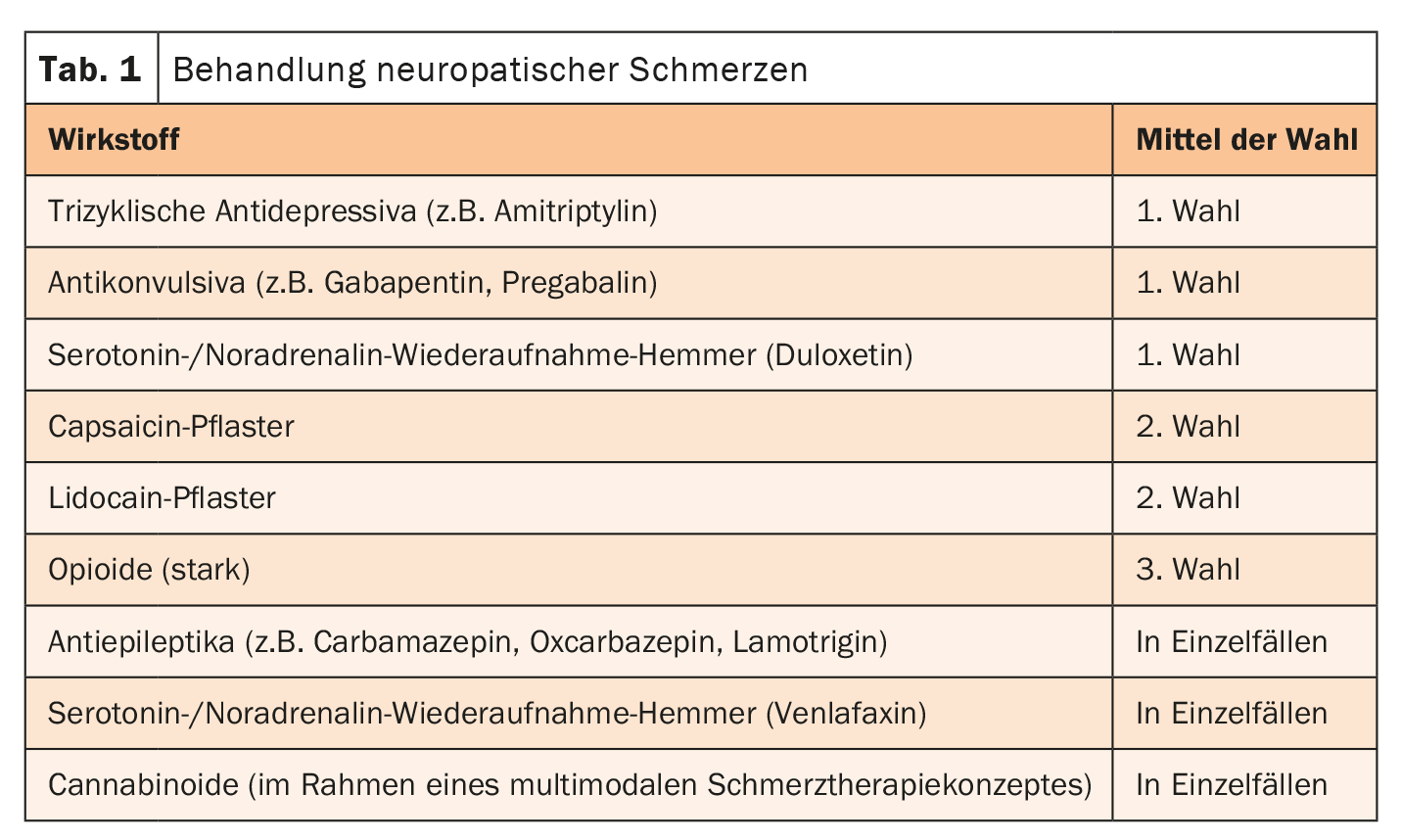
Treatment management is primarily based on the underlying disease. This should be optimally treated. Well-controlled blood sugar or abstinence from alcohol can prevent further progression of nerve damage. In addition, it is important to effectively control the symptoms – first and foremost the pain. However, the mechanisms of neuropathic pain are fundamentally different from those of nociceptive pain. Therefore, a special therapy concept is indicated. Analgesics are often not effective. The drugs of choice are primarily tricyclic antidepressants, serotonin/norepinephrine reuptake inhibitors, and anticonvulsants (Table 1) .
Further reading:
- www.neurologen-und-psychiater-im-netz.org/neurologie/erkrankungen/polyneuropathie
(last accessed 11.10.2023) - www.msdmanuals.com/de-de/heim/st%C3%B6rungen-der-hirn-,-rückenmarks-und-nervenfunktion/erkrankungen-der-peripheren-nerven-und-verwandte-erkrankungen/polyneuropathie (last accessed 11.10.2023)
- www.dgn.org/leitlinien/3754-ll-030-067-diagnostik-bei-polyneuropathien-2019 (last accessed 11.10.2023)
- Sommer C, Geber C, Young P, et al: Polyneuropathies – etiology, diagnosis, and treatment options. Dtsch Arztebl Int 2018; 115: 83-90.
- Petersen JA, Schlereth T: Diagnosis and therapy of neuropathic pain. Psychiatry + Neurology 2022; 3: 20-24.
InFo NEUROLOGY & PSYCHIATRY 2023; 21(5): 33.









