
Basic skin care with emollients is an essential part of the treatment of atopic dermatitis. In mild forms, such as those found in a majority of affected children, skin care products can effectively treat xerosis, even if pronounced, and normalize skin hydration. Systematic basic care is essential for relapse prevention.
Skin care products are part of any treatment for atopic dermatitis. Both the American and the European guidelines recommend the use of emollients as basic care in all stages – even if “only” xerosis cutis is present [1, 2]. Systematic basic care has been shown to reduce the use of topical steroids in atopic dermatitis [3]. Furthermore, skin care products have been shown to improve the skin barrier and thus protection against pollutants [4] and prevent skin drying due to bathing [5]. “However, the crucial question is whether xerosis cutis can be improved in children with atopic dermatitis with basic skin care products alone. Although the majority of affected children suffer only from mild atopic dermatitis with xerosis, there are hardly any studies on this stage,” said Prof. Franck Boralevi, MD, Bordeaux, at a satellite symposium organized by Pierre Fabre (Suisse) SA at the SGDV Congress in Montreux.
Emollients significantly reduce the xerosis score
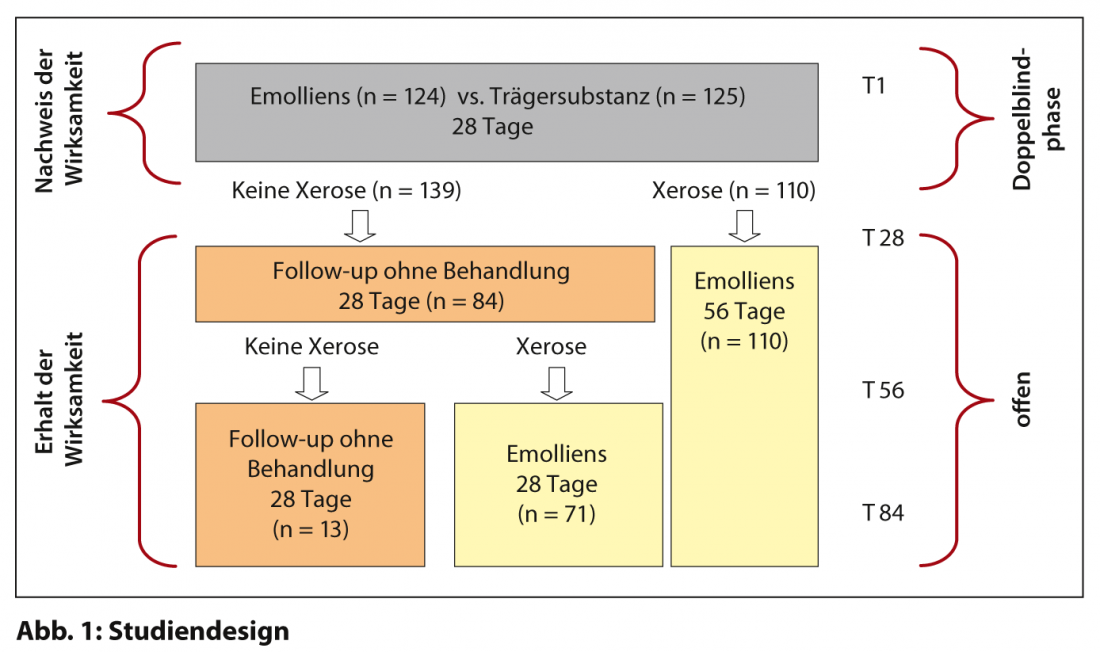
For this reason, a randomized, multicenter, double-blind study was conducted in five European countries between November 2011 and May 2012 to evaluate the efficacy of a glycerol-based emollient in 249 children with mild atopic dermatitis but moderate to severe xerosis. (DEXERYL®) regarding moderate to severe xerosis and hydration of the skin [6]. The study was divided into two phases, double-blind and open-label. In the double-blind phase, the emollient was compared with the pure carrier substance over a period of 28 days. In the subsequent open phase, 194 patients from both groups were followed up for another 56 days; patients who still showed xerosis were treated with the emollient, while in responders, treatment was stopped and, if necessary, restarted after another 28 days if xerosis recurred ( Fig. 1).
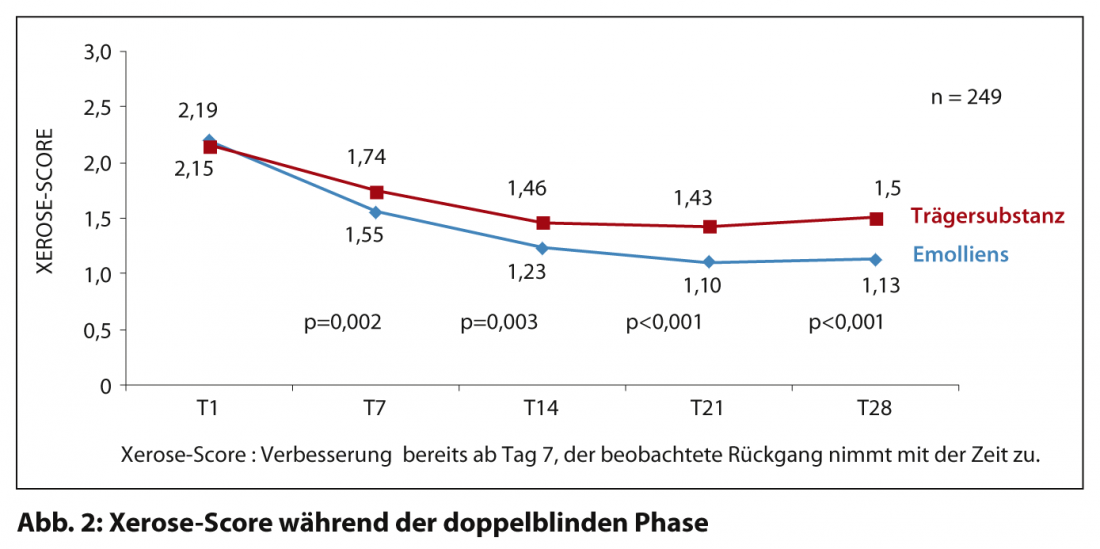
Children aged two to six years with mild atopic dermatitis without florid efflorescences were included. Additional inclusion criteria were a xerosis score ≥2 (SCORAD subscore), a SCORAD score <15, and, as clinical markers for a predisposition to atopic dermatitis, hyperlinearity of the palms and soles and/or scales on the inner side of the shins. At inclusion in the study, all baseline characteristics were comparable in both groups. The xerosis score averaged 2.17, and the SCORAD score averaged 15.3. After 28 days, the xerosis score had improved significantly in both groups, but significantly more in the verum group than in the control group (decrease in xerosis score: -0.93 resp. -0.63; p<0.001) (Fig. 2). Skin hydration also improved in both groups, with the verum also performing significantly better than the carrier substance alone (increase in hydration index: +11.14 resp. +5.56; p<0.001; decrease in objective SCORAD: -5.38 resp. -3.10; p<0.001).
Recurrence after discontinuation of the emollient
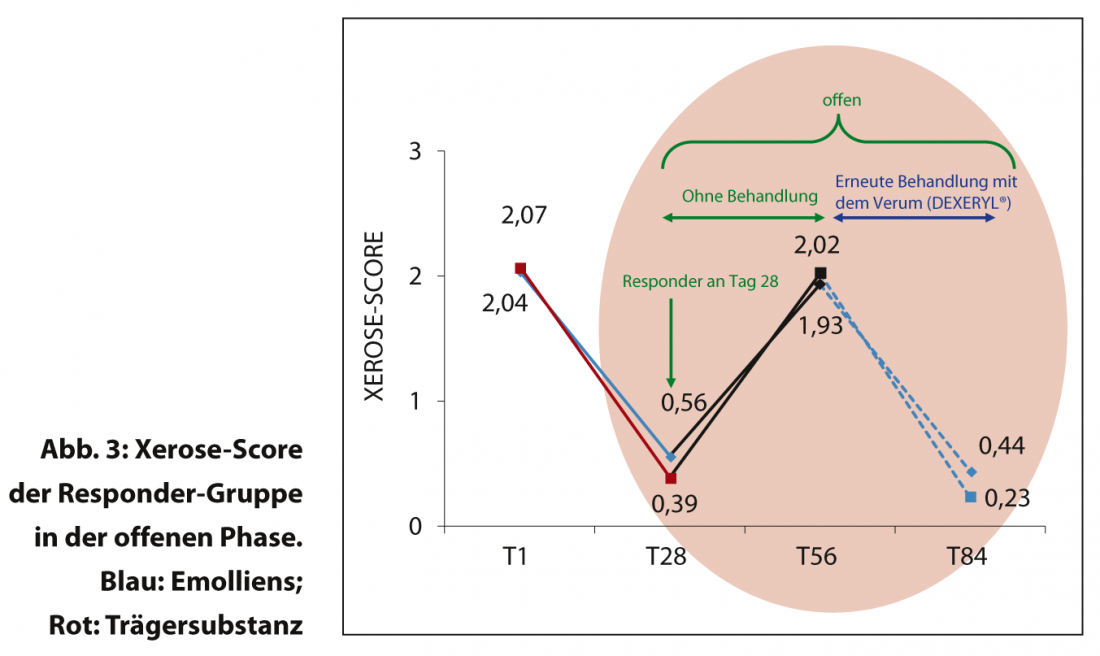
The double-blind phase was followed by an open phase, as described above, in which treatment was suspended in responders. In 84% of these patients, xerosis recurred rapidly without baseline care, so that the xerosis score had virtually returned to baseline at the 28-day follow-up. In parallel, the hydration index also deteriorated. After resuming basic care with the emollient, xerosis again improved rapidly (Fig. 3), and the hydration index also returned to normal. This impressively demonstrates the importance of consistent basic care with an emollient for xerosis cutis in atopic dermatitis. Without basic care, recurrence occurs very quickly.
Conclusion
In children with mild atopic dermatitis, even with moderate to severe xerosis, systematic skin care with a glycerol-based emollient significantly improves the xerosis score and normalizes skin hydration. To avoid recurrence, permanent systematic basic care with emollients is essential.
Source: Lunchsymposium “Systematic basic care in atopic dermatitis a must! A multicenter study proves the necessity”, 95th Annual Meeting of the SGDV, September 19-21, 2013, Montreux Kindly supported by Pierre Fabre (Suisse) SA, Allschwil.
Literature:
- NICE: Atopic eczema in children: Management of atopic eczema in children from birth up to the age of 12 years. Clinical guidelines, CG57 – Issued: December 2007.
- Darsow U, et al: ETFAD/EADV eczema task force 2009 position paper on diagnosis and treatment of atopic dermatitis. J Eur Acad Dermatol Venereol 2010; 24: 317-328.
- Grimalt R, et al: The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology 2007; 214: 61-67.
- Lodén M, et al: Improvement in skin barrier function in patients with atopic dermatitis after treatment with a moisturizing cream (Canoderm). Br J Dermatol 1999; 140: 264-267.
- Chiang C, et al: Quantitative assessment of combination bathing and moisturizing regimens on skin hydration in atopic dermatitis. Pediatr Dermatol 2009; 26: 273-278.
- Vaillant L, Georgesco G, Rivollier C: Study Report V00034 CR 202, 2003. Dermatology department, University hospital of Tours, France.
- Cetta F, et al: Newborn chemical exposure from over-the-counter skin care products. Clin Pediatri 1991; 30: 286-289.









