
More and more patients express that they do not want any therapeutic measures in case of foreseeable irreversible unconsciousness or severe permanent brain damage. Valid forecast parameters are needed for such decisions, and the coincident coexistence of several indicators of an unfavorable forecast should be present.
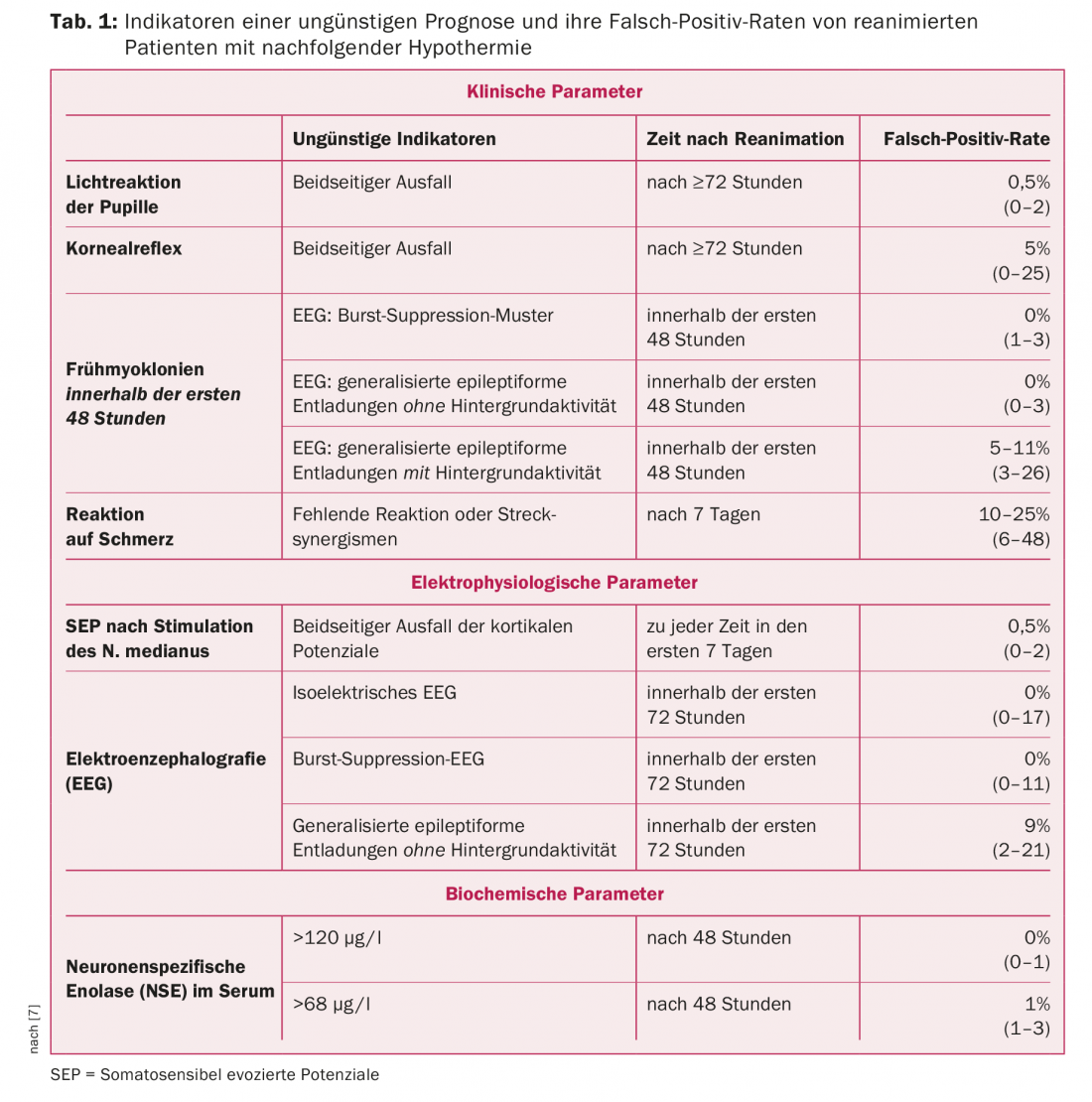
Approximately 80% of patients who reach the hospital after cardiopulmonary resuscitation initially remain comatose. These patients often have an unfavorable prognosis, meaning they die or survive with severe irreversible brain damage [1,2]. Understandably, there is a great interest in assessing the prognosis as reliably as possible, especially since more and more patients express in an advance directive or in discussions with their relatives that they do not want any therapeutic but only palliative measures in the event of foreseeable irreversible unconsciousness or severe permanent brain damage. Decisions of such magnitude can only be made on the basis of valid parameters, whereby for the greatest possible certainty of the prognosis assessment, the coinciding coexistence of several indicators of an unfavorable prognosis should be present (Tab. 1).
After it was shown 15 years ago (in a very selected group of patients) that 24 hours of hypothermia (around 33°C) after resuscitation improves prognosis [3], therapeutic hypothermia quickly found its way into appropriate treatment guidelines. Following this, the question arose as to the reliability of the forecast parameters previously considered valid. This has led to a whole series of studies in which many more patients have been examined than was the case before the introduction of therapeutic hypothermia [reviews 4-7]. Thus, the indicators of an unfavorable forecast presented below can be considered very reliable. These parameters have a high specificity but only a relatively low sensitivity, so that in the absence of reliable indicators of an inauspicious prognosis, a good prognosis cannot be safely assumed.
Assessment of the forecast
The fundamental prerequisite for a reliable assessment of prognosis is the lack of influence of sedating drugs during clinical and electrophysiological examinations. It is therefore advisable to use only substances with a short half-life (e.g., propofol) for sedation in the first few days, which can then be discontinued before the examination. It should be borne in mind that analgesic and sedative substances are probably degraded at a slower rate during therapeutic hypothermia. However, systematic studies of larger patient groups are still lacking.
Clinical indicators of an inaustere prognosis
Clinical findings are still the leading factor in the assessment of prognosis and continue to be of great importance despite the increasing use of instrumental and biochemical tests. In this regard, the following clinical indicators of an unfavorable prognosis are based on studies of the largest number of patients overall.
Brainstem reflexes: Absence of pupillary light response and corneal reflex on the third day after resuscitation (or at least 24 hours after discontinuation of analgesic and sedative medications) are valid indicators of an unfavorable prognosis quoad functionem, with the failed light response being the most reliable [4–7].
Early myoclonia: Postanoxic early myoclonia occurring in the first two days after resuscitation is another clinical indicator of an unfavorable prognosis. They may be suppressed during hypothermia by deep sedation and/or relaxation and therefore may only become apparent after rewarming or discontinuation of sedating and/or relaxing drugs. These are spontaneously occurring and typically with external stimuli (touching the patient, suction, acoustic stimuli) clearly increasing in severity, sometimes also occurring only with external stimuli, irregular short twitches of individual muscles or muscle groups. These primarily affect the facial, upper arm and shoulder muscles as well as the diaphragm, but in principle can involve all muscle groups. Patients with generalized myoclonia almost invariably have an unfavorable prognosis [4–7]. Patients with focal myoclonias have a much better prognosis according to recent findings [8]. Therefore, the latter cannot be considered as sure indicators of an unfavorable prognosis. In this regard, an EEG can provide additional important information because there is an unfavorable prognosis in the presence of burst suppression EEG or generalized epileptiform discharges without preserved background activity [9].
Response to pain: Lack of motor response to pain or stretch synergism is not a valid indication of an unfavorable prognosis until seven days after resuscitation. This may be due to the fact that during therapeutic hypothermia patients are treated with analgesic and sedative substances in sometimes relatively high doses, which are also metabolized more slowly under these conditions, so that prolonged drug-induced attenuation of protective reflexes is to be expected.
Electrophysiological indicators of an inaustere prognosis
There are no established concentration-response relationships for centrally depressant substances that may lead to an influence of electrophysiological parameters. Also, findings from brain-healthy patients are not easily transferable to patients with acute hypoxic brain injury. Therefore, for the greatest possible diagnostic certainty, only findings after discontinuation of analgesic and sedative substances should be evaluated prognostically.
Somatosensory evoked potentials (SEP): Failed cortical components after stimulation of the median nerve after cessation of therapeutic hypothermia reliably indicate an inadequate prognosis. A good outcome has been reported in bilateral loss of cortical components only very occasionally [4–7].
Electroencephalography (EEG): a failure of brain electrical activity (isoelectric EEG), burst suppression EEG (as commonly defined by professional societies or standard textbooks), and continuous generalized epileptiform discharges (such as “spikes” or “sharp waves”) without background activity and lack of reactivity to external stimuli are reliable indicators of an unfavorable prognosis quoad functionem [4–7].
Biochemical parameters of an inaustere prognosis
Neuron-specific enolase (NSE) in serum: The upper limits for an inauspicious prognosis reported by different research groups vary, which was also the case before the introduction of therapeutic hypothermia. In these studies, it is not always possible to determine with certainty whether other causes of high NSE had been reliably ruled out, since erythrocyte decay during extracorporeal procedures or erythrocyte transfusions or tumor diseases can lead to high NSE. After 48 hours, an NSE above 120 µg/l can be considered a valid indicator of an inaustere prognosis [4–7]. Other biochemical markers, such as protein S-100, which may also be highly sensitive, have been studied in far fewer patients and thus do not have as high prognostic confidence as NSE.
Imaging techniques
Previous findings suggest that certain CT and MRI findings may indicate an unfavorable prognosis [6,7]. However, by far not as many patients have been examined here as is the case with the above-mentioned parameters, so that these parameters are not to be regarded as so reliable. Also, these examinations are not possible everywhere. In particular, MRI superior to CT in detecting structural lesions and the ability to perform MRI in intubated ventilated patients is not universally available.
Consequences for practice
A foreseeably inauspicious prognosis, i.e., the patient’s death, a permanent coma or a syndrome of unresponsive wakefulness (“waking coma,” “apallic syndrome,” “persistent vegetative state”), as well as a severe neurological defect syndrome with a permanent need for care and assistance are of considerable consequence. In such cases, the nature and extent of further intensive care should be reconsidered and discussed with the relatives and the ICU team. In particular, if the patient’s will is known and he or she would have wished only palliative treatment in the face of a foreseeably unfavorable prognosis, this must be respected and the therapy limited accordingly. In this case, the administration of morphines and benzodiazepines is also justified and welcomed by the relatives in order to safely exclude the possibility that the affected person is suffering, even if a conscious perception of pain is not possible given the existing massive brain damage. Decisions of such magnitude cannot be made on the basis of a single finding. Only in the case of the coincident coexistence of (a) at least one unfavorable clinical sign; and b) an infaused electrophysiological parameter or a significantly elevated NSE, preferably both, an infaused prognosis can be reliably assumed.
Take-Home Messages
- There are a number of valid clinical, instrumental, and biochemical indicators of an inauspicious prognosis.
- In the absence of valid indicators of an inauspicious prognosis, a good prognosis cannot be safely assumed.
- The fundamental prerequisite for a reliable assessment of prognosis is the lack of influence of sedating drugs during clinical and electrophysiological examinations.
- Only in the case of the coincident coexistence of (a) at least one unfavorable clinical sign; and b) an infaused electrophysiological parameter or a significantly elevated neuron-specific enolase (NSE), preferably both, can be reliably assumed to have an infaused prognosis.
Literature:
- Peberda MA, et al: Cardiopulmonary resuscitation of adults in the hospital: a report of 14,720 cardiac arrests from the National Registry of cardiopulmonary Resuscitation. Resuscitation 2003; 58: 297-308.
- Madl C, Holzer M: Brain function after resuscitation from cardiac arrest. Curr Opin Crit Care 2004; 10: 213-217.
- The Hypothermia after Cardiac Arrest Study Group: Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002; 346: 549-556.
- Thömke F: Assessment of prognosis after cardiopulmonary resuscitation and therapeutic hypothermia. Dtsch Arztebl Int 2013; 110: 137-143.
- Cahill EA, et al: An update in postcardiac arrest management and prognosis in the era of therapeutic hypothermia. Neurohospitalist 2014; 4: 144-152.
- Sandronia C, et al: Prognostication in comatose survivors of cardiac arrest: An advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Resuscitation 2014; 85: 1779-1789.
- Rossetti AO, et al: Neurological prognostication of outcome in patients in coma after cardiac arrest. Lancet Neurol 2016; 15: 597-609.
- Bouwes A, et al: Acute posthypoxic myoclonus after cardiopulmonary resuscitation. BMC Neurology 2012, 12: 63.
- Elmer J, et al: Clinically distinct electroencephalographic phenotypes of early myoclonus after cardiac arrest. Ann Neurol 2016; 80: 175-184.
CARDIOVASC 2018; 17(3): 25-28









