
In the lower extremities, the most common location for fracture is the lower leg (11.4%), with 7% involving the distal lower leg. Femur fractures are quite rare at 2.9%. What should be considered in practice when encountering such fractures? How to diagnose and treat them? This second part of the series on pediatric traumatology (the first appeared in HAUSARZT PRAXIS 5/2014) is intended to provide information about this.
Avulsion spina iliaca anterior inferior or superior (osseous avulsion of the rectus femoris) is a fracture often caused by forced flexion in the hip joint (kick in football, sprint in athletics) with sudden onset of pain. The therapy of choice is usually conservative treatment by means of cane unloading and mobilization according to the symptoms.
Pertrochanteric femur fracture/ femoral neck fracture
This is a rare injury in children, usually caused by high-energy trauma. Open reduction and plate osteosynthesis is usually indicated in this case. Very rarely, conservative treatment in the form of immobilization and unloading can be performed for undislocated fractures (undislocated fissures).
In children younger than four years, therapy of pertrochanteric fracture or femoral shaft fracture by Bryant extension is possible for three to four weeks (Fig. 1). Here, the child’s own body weight eliminates the muscle pull of the dislocating muscles (iliospsoas muscle, etc.), so that a quasi-anatomical reduction of the fracture is achieved. In older children, this is then no longer possible due to body weight and lack of compliance.

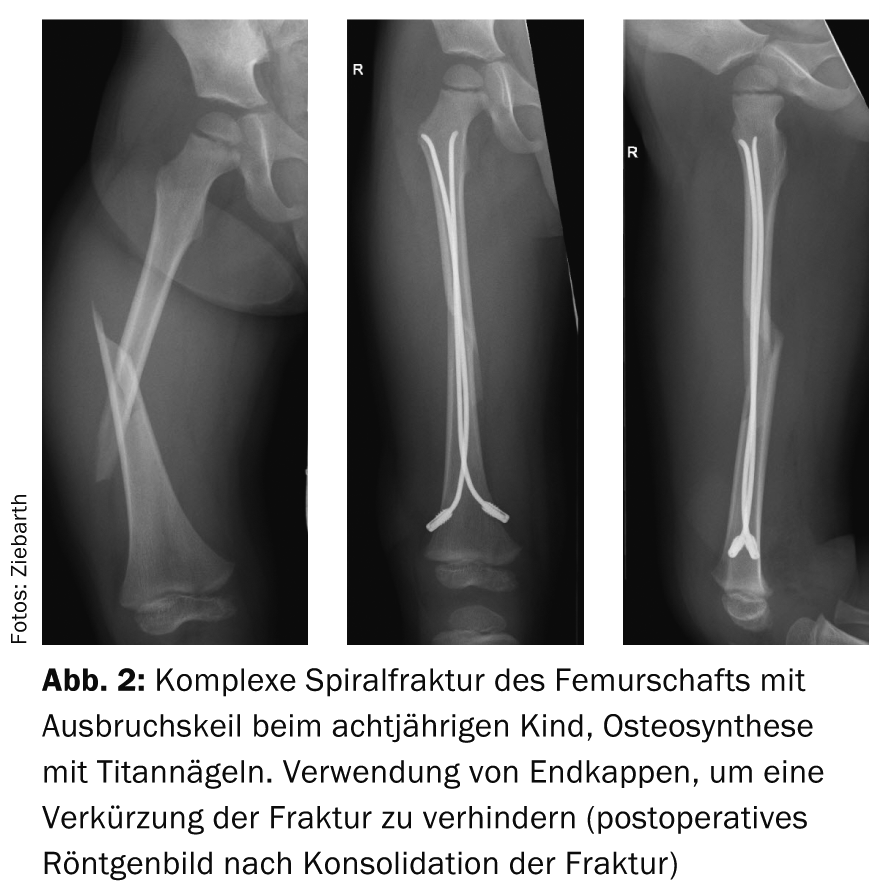
In children over four years of age, the domain of femoral shaft fracture therapy is closed reduction and intramedullary splinting (ESIN technique, Fig. 2). Here, too, no further immobilization is necessary postoperatively.
Intraarticular fractures
Such are very rare, but require anatomic reduction and screws vs. Kirschner wire osteosynthesis. Here, if the distal femoral growth plate is injured, disruption of further growth must be expected and this must be explained to the parents at an early stage.
Special forms of knee injuries
Avulsion Eminentia interkondylaris (classification according to Myer/McKeever): This is often caused by a fall on a bicycle. A hemarthros is visible. The injury corresponds to an osseous avulsion of the anterior cruciate ligament. For undislocated fractures, conservative treatment is used. Open reduction or arthroscopically assisted reduction and fixation is performed using cannulated screws or osteosuturing (suture fixation) for dislocated fractures.
Rupture of the anterior cruciate ligament (ACL)/meniscus lesion: In the case of ruptures of the anterior cruciate ligament, early reconstruction of the ACL should be aimed for, even in young children, in order to avoid secondary damage [1], since nowadays children are very active in sports at a young age and the knee joints are exposed to heavy loads. Numerous studies have shown that to a large extent meniscal damage is already present after ACL injuries in children and that additional meniscal lesions occur after conservative treatment of ACL rupture [2]. Arthroscopic refixation is also indicated for isolated meniscal injuries in children.
In addition, the Inselspital is the only hospital to offer cruciate ligament-preserving surgery (interligamentary stabilization) of the anterior cruciate ligament for children, with promising results to date.
Lower leg fractures
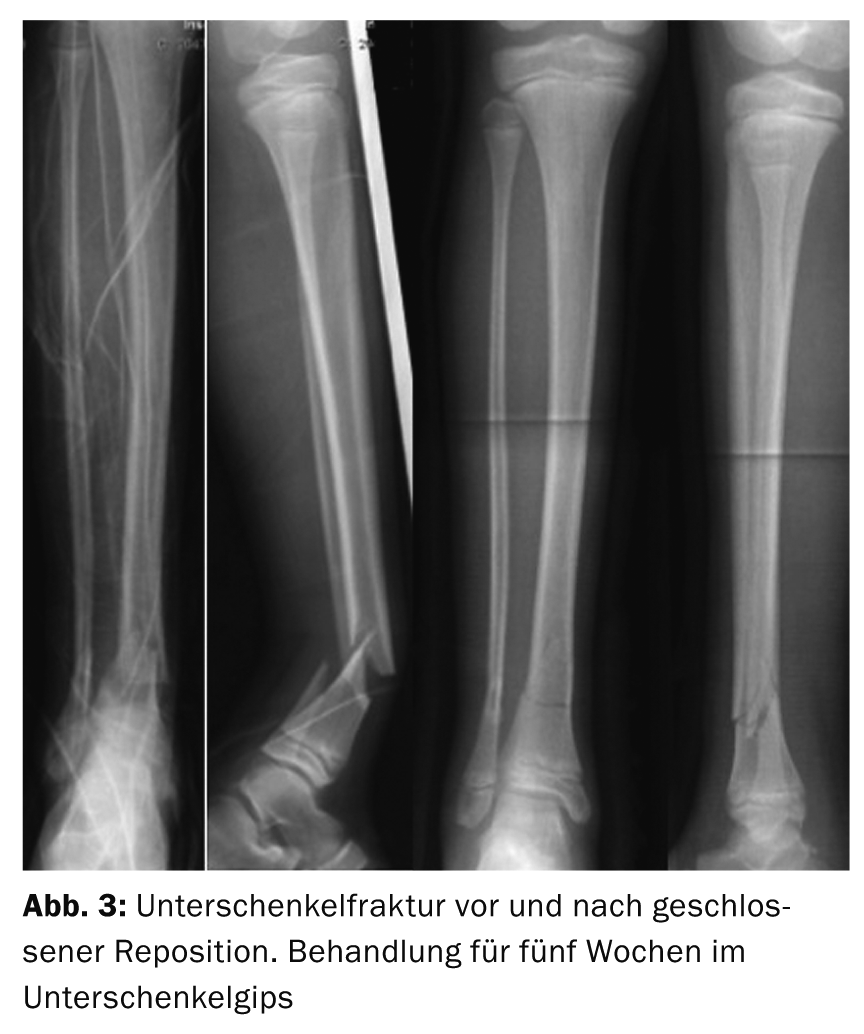
These are often treated conservatively in a thigh cast. In the case of severely dislocated fractures, a closed reduction is performed under anesthesia followed by plaster immobilization. If the fracture cannot be held in place intraoperatively by plaster immobilization, external fixator treatment or ESIN treatment is indicated, depending on the location of the fracture. In the case of distal (supramalleolar) tibial fractures, it may also be possible to immobilize the fracture in a tibial cast (Fig. 3). In case of instability, reduction and Kirschner wire fixation with subsequent immobilization in plaster are performed.
Malleolar fractures
Most often, the medial malleolus is affected. Immobilization in a lower leg cast is sufficient for undislocated injuries. Only in severely dislocated fractures, or intra-articular fractures, closed vs. open reduction and Kirschner wire or screw osteosynthesis must be performed.
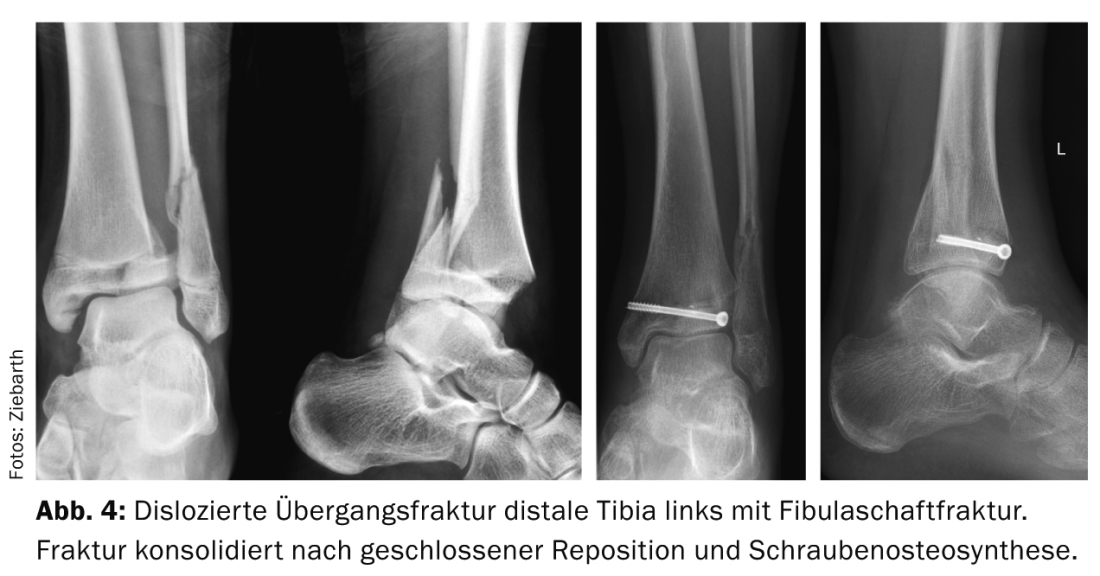
Special forms – transitional fractures (Fig. 4): This special fracture occurs in older children during adolescence. Due to partial closure of the distal tibial growth plate in adolescence, the fracture proceeds in two or three planes (twoplane, triplane). Here, the exact course of the fracture must be followed radiologically. If necessary, three-dimensional imaging (CT) is helpful. Undislocated fractures (<2 mm) are immobilized in a lower leg cast. Dislocated fractures require closed reduction and ostoeosynthesis with cannulated screws, or even open reduction and screw osteosynthesis. This depends on the particular type of transitional fracture.
Foot/toe fractures
The same applies here as for hand and finger injuries (see Part I in HAUSARZT PRAXIS 5/2014, p. 28). Only in the case of rotational defects or open fractures is reduction under conduction anesthesia or surgical osteosynthesis indicated. Otherwise, immobilization takes place in a lower leg plaster cast or with a hard sole.
Dislocated fractures of the tarsal bones (talus, calcaneus, etc.) are extremely rare and belong in the hands of a specialist.
Kai Ziebarth, MD
Literature:
- Ziebarth K, et al: Anterior cruciate ligament injuries in children and adolescents: a review of the recent literature. Eur J Pediatr Surg 2013 Dec; 23(6): 464-469.
- Fabricant PD, et al: Reconstruction of the anterior cruciate ligament in the skeletally immature athlete: a review of current concepts: AAOS exhibit selection.
- J Bone Joint Surg Am 2013 Mar 6; 95(5): e28.
CONCLUSION FOR PRACTICE
- Avulsion spina iliaca anterior inferior or superior (osseous avulsion M. rectus femoris): The therapy of choice is usually conservative treatment by means of cane unloading and mobilization according to the symptoms.
- Pertrochanteric femur fracture/ femoral neck fracture: Open reduction and plate osteosynthesis is usually indicated here.
- Femoral shaft fractures can be treated in children <4 years in overhead extension. In larger children, closed reduction and osteosynthesis is performed using the ESIN technique.
- Intra-articular fractures require anatomic reduction and screws vs. Kirschner wire osteosynthesis.
- Lower leg fractures are often treated conservatively (thigh cast).
- Malleolar fractures: In undislocated injuries, immobilization in a lower leg cast is sufficient.
- Foot/toe fractures: Reduction under conduction anesthesia or surgical osteosynthesis are indicated only for rotational fractures or open fractures.
A RETENIR
- Avulsion de l’épine illiaque antérieure inférieure ou supérieure (arrachement osseux M. rectus femoris): le traitement de choix est principalement le traitement conservateur avec décharge à l’aide de cannes anglaises et mobilisation selon l’ampleur de l’atteinte.
- Fracture pertrochantérienne du fémur/fracture du col du fémur: une reposition ouverte et une ostéosynthèse du plateau est principalement indiquée ici.
- Les fractures du fût fémoral peuvent être traitées en Overhead-Extension chez les enfants de moins de 4 ans. Pour les enfants plus âgés la reposition fermée avec ostéosynthèse dans la technique ESIN est réalisée.
- Les fractures intra-articulaires nécessitent la reposition anatomique et des vis vs. ostéosynthèse par broche de Kirschner.
- Les factures de la jambe sont souvent traitées de manière conservatives (plâtre de la cuisse).
- Fractures des malléoles: en cas de lésions non- disloquées une immobilisation dans un plâtre de la jambe est suffisante.
- Fractures du pied/des orteils: une reposition avec anesthésie loco-régionale ou une intervention pour ostéosynthèse ne sont indiquées qu’en cas d’absence de rotation ou de fractures ouvertes.
HAUSARZT PRAXIS 2014; 9(6): 38-40









