
With the introduction of PDE5 inhibitors in the late 1990s, the treatment of erectile dysfunction experienced a breakthrough. However, ED is not an isolated phenomenon. It may be a manifestation of deeper vascular disease.
“The big upheaval in the treatment of erectile dysfunction occurred about 20 years ago, when PDE5 inhibitors were introduced,” explained Ashkan Mortezavi, MD, of the Department of Urology at University Hospital Zurich. Despite the new drugs at the time, which offered an attractive alternative to invasive methods and thus for the first time held out the prospect of a significantly less burdensome therapy for erectile dysfunction, the inhibition to talk about the subject was and still is high. Only a quarter of those affected go to a doctor – and this only after two years on average. It turns out that sexual interest by no means disappears with age. In surveys [1], even among older and very old men up to 95 years of age, almost half still agree that sex is still relevant. At the same time, almost the same number of persons were dissatisfied or saw their sexual desires insufficiently satisfied (“less frequently than desired”). Still, older men don’t just want sex, they have it. The percentage of sexually active men in their 70s is still over 60%.
However, it is precisely this age group that suffers particularly frequently from erectile dysfunction. A Cologne study found a prevalence of over 50% in Germans aged 70-80 years (overall prevalence 19.2%) [2]. By definition, erectile dysfunction is present when there is (repeated) erectile dysfunction for more than six months that does not allow satisfactory sexual intercourse. “The results also show that almost one in 10 people are already affected by it in their 40s. Younger people tend to talk about it even less often with their family doctor,” he said. “The key factor in an erection is blood flow. Nerves also play a role, but a much smaller one than blood, so it’s not surprising that erectile dysfunction often occurs with other cardiovascular risk factors.”
The tip of the iceberg
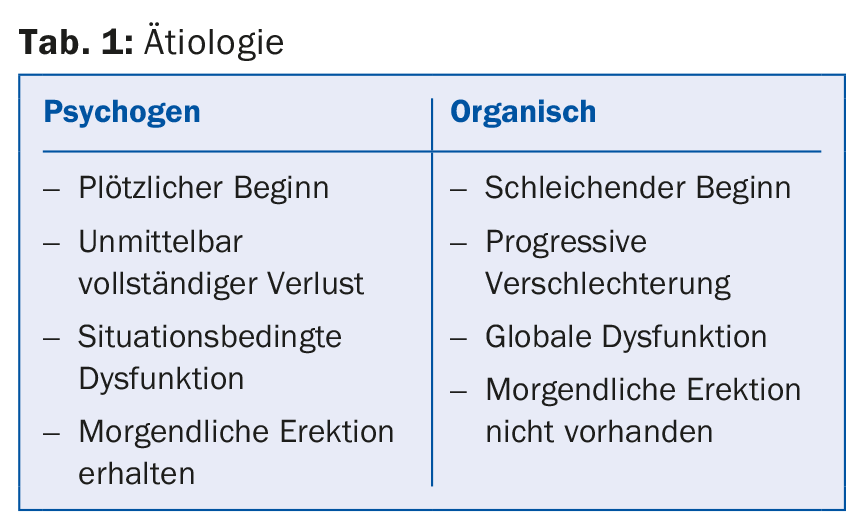
Basically, it can be said that the younger the patient, the more often a psychogenic cause. Overall, about 50% of erectile dysfunctions are due to purely organic causes and 20% to purely psychogenic causes, with the remaining third being mixed pathologies (Table 1). Organically, vascular causes are by far the most common (over two-thirds). “Little surprising, if you consider the importance of the blood for the erection of the corpus cavernosum. If the vessels in the penis no longer function properly, dysfunction is likely elsewhere as well. Erectile dysfunction, for example, may indicate the presence of CHD,” the expert explained. So are erectile problems just the tip of an iceberg, which in this case is systemic vascular disease, as suggested by a 2003 study [3]? Almost 70% of CHD patients suffered from erectile dysfunction before angina symptoms. There was an interval of more than three years between the onset of erectile dysfunction and CHD. Further clarifications in this direction are therefore useful in ED patients. Other associated risk factors include hypertension and diabetes (which is bad for all vessels).
“Also relevant are drug-induced erectile dysfunction and, especially represented in urology, dysfunction after surgery, radiation or trauma to the pelvis” explained Dr. Mortezavi. Neurogenic causes (altogether responsible for about 5% of organically caused cases) can be dementia, stroke, Parkinson’s disease, but also epilepsy or MS. Trauma and spinal cord injury are more likely to play a role in younger patients. Regarding medications, it has been known for many years that beta-blockers, thiazides, and clonidine can induce erectile dysfunction. With antidepressants, erectile dysfunction is often accompanied by loss of libido.
Is erectile dysfunction fatal?
If erectile dysfunction and CHD share common risk factors, is the former even a “life-threatening” disorder? Indeed, a significant 19% increase in relative mortality risk is found in ED patients compared with non-ED patients [4]. In contrast, coital death is very rare and accounts for only about 0.6% of sudden deaths. It is more common in men than women, especially when sexual intercourse occurs out of wedlock, with younger partners, and in unfamiliar settings.
Therapy is useful
“The associations with other cardiovascular diseases are not meant to suggest that we can’t or shouldn’t do anything about erectile dysfunction itself. Most patients benefit from therapy, and it is becoming clear that the demands on treatment lie primarily in its reliability, safety, and good side effect profile, rather than in price or rapid effect,” he said.
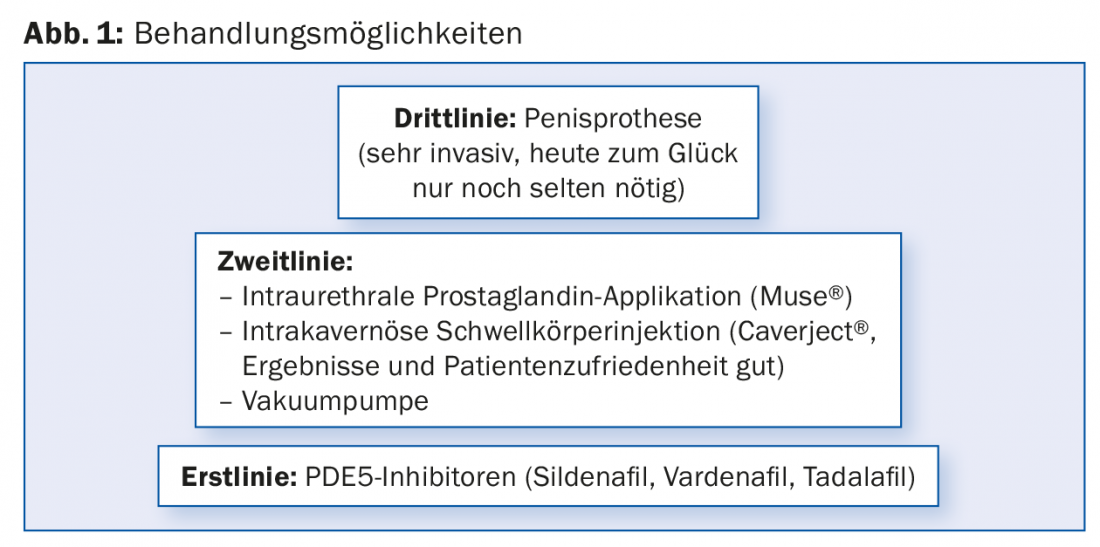
Lifestyle measures are recommended first. These are worthwhile, especially quitting smoking can “work wonders,” according to Dr. Mortezavi. Weight reduction is also important. The treatment options are shown in Figure 1, where a distinction must be made between invasive and noninvasive approaches.
“Those who care about sexual spontaneity during a planned weekend can take a tablet of tadalafil on Friday afternoon, for example. This has the longest half-life of 17.5 hours,” says Dr. Mortezavi. “The PDE5 inhibitors are well tolerated overall. They are very effective in many different forms of ED [5]. Controlled and postmarketing studies showed no increased risk of myocardial infarction or death. Caution is advised in aortic stenosis, left ventricular outflow tract obstruction, hypotension, and hypovolemia. Nitrates including poppers are an absolute contraindication.”
If the effect is insufficient, therapy can be optimized in several ways:
- Reminder: sexual stimulation is a prerequisite
- Reduced food intake (“not after 7-course meal”)
- Dose increase
- Training (“the longer erectile dysfunction has existed, the longer it takes to work again”), optimal result only after the ninth or tenth intake
- Non-responders: at least four attempts required.
Accelerated onset of action
Most men do not know in advance when they will have sex. New drugs such as Spedra® (avanafil) therefore promise an accelerated onset of action. This is a highly selective, effective PDE5 inhibitor that can also be used for more or less “spontaneous” sexual desire (effect after only ten minutes). The side effect profile is very low, but there is still relatively little empirical data.
Source: General Internal Medicine Update Refresher, May 10-13, 2017, Zurich.
Literature:
- Hyde Z, et al: Prevalence of sexual activity and associated factors in men aged 75 to 95 years: a cohort study. Ann Intern Med 2010 Dec 7; 153(11): 693-702.
- Braun M, et al: Epidemiology of erectile dysfunction: results of the ‘Cologne Male Survey’. Int J Impot Res 2000 Dec; 12(6): 305-311.
- Montorsi F, et al: Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. Eur Urol 2003 Sep; 44(3): 360-364; discussion 364-365.
- Jackson G: Erectile dysfunction and coronary disease: evaluating the link. Maturitas 2012 Jul; 72(3): 263-264.
- Fink HA, et al: Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med 2002 Jun 24; 162(12): 1349-1360.
HAUSARZT PRAXIS 2017; 12(6): 54-55









