Modern immunomodulatory therapy options allow for significantly greater and more rapid symptom reduction compared to the past. Appropriate testing should be performed to control the risk of reactivation of a previous hepatitis infection.
Hepatitis B (HBV) is one of the most common infectious diseases. If left untreated, severe complications such as liver failure are possible. It is usually an acute viral disease, but chronic courses also occur. In a review published in JAAD in 2019, it is recommended to screen all psoriasis patients before starting systemic therapy, including the following parameters: Antibodies against hepatitis B core (anti-Hbc), hepatitis B surface antigen (HbsAg), and antibodies against HCV (anti-HCV) [1].
Prophylaxis as an important factor
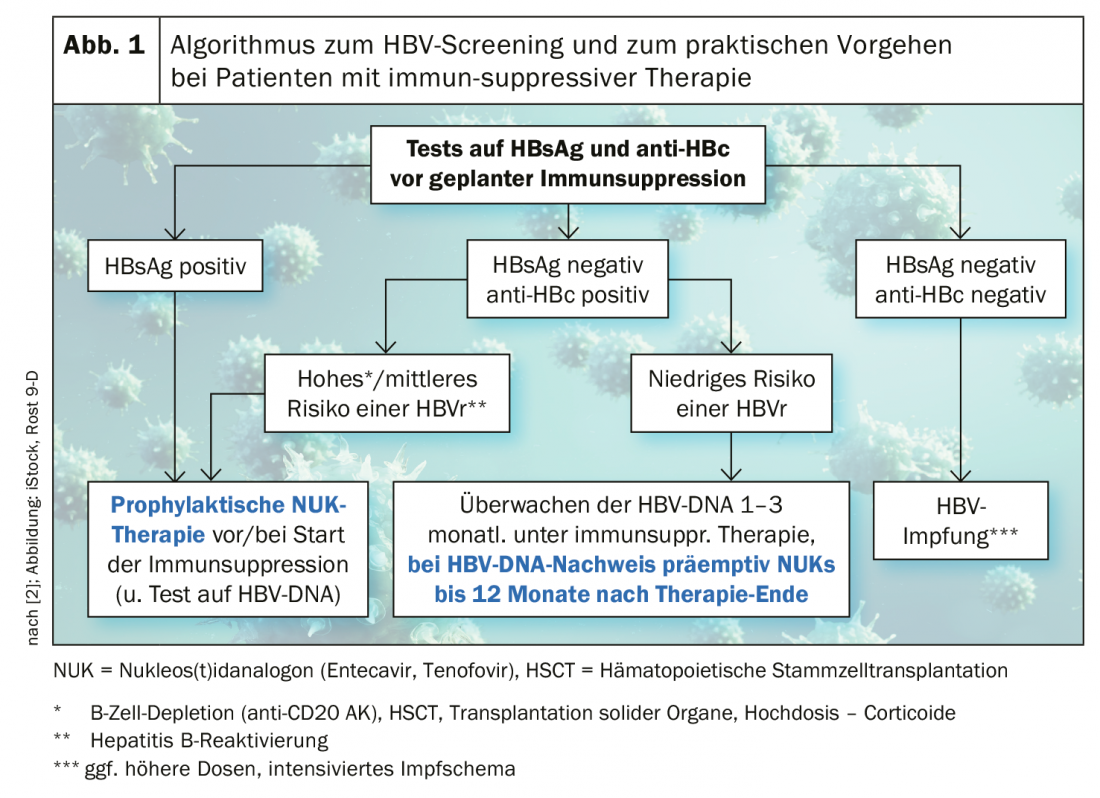
For HbsAg+ or high/intermediate risk of hepatitis B reactivation (HBVr), prophylactic therapy with a nucleos(t-id analog (entecavir, tenofovir) is suggested before/when starting systemic therapy. If the risk is low, monitoring of HBV DNA is sufficient. If there are negative results for HBsAg and anti-HBc, vaccination is the best preventive method [2,3]. The findings on the specific risk profiles of individual active ingredients with regard to HBVr vary.
Regarding methotrexate (MTX), it is known that there is an increased risk of HBVr [1,4,5]. To date, there are no evidence-based data on apremilast and dimethyl fumarate. With regard to TNF-alpha inhibitors, one study found a re-emergence of serum HBV DNA in 39% of patients testing positive for HBV markers, showing that the rate of reactivation was several-fold higher in anti-HBc+ subjects than in HBsAg+ carriers [6]. The empirical data on interleukin antagonists are rather limited. A prospective cohort study of ustekinumab demonstrated that HBVr was relatively rare under this IL12/23 inhibitor [7]. Data are based on a sample of 93 patients treated with ustekinumab for 24 ± 12 months from 2011 to 2016. At baseline, all subjects were serologically tested and HBV DNA testing was performed annually. Among the 54 subjects who were carriers of inactive or healed HBV or who had isolated anti-HBC+ findings, virological reactivation occurred in only 3 patients.
| Take-Home-Message Several international guidelines recommend hepatitis screening before starting psoriasis systemic therapy [4]. Depending on the findings, vaccination or antiviral prophylaxis may be considered. Systemic therapies that interfere with the immune system may be associated with the risk of reactivation of previous hepatitis infections. Empirical data on the risk profiles of the individual active ingredients in this regard are still scarce. Regular monitoring of liver values enables this factor to be controlled and, if necessary, appropriate measures to be initiated. |
Monitoring of liver values is essential
According to the current S3 guideline of the AWMF, systemic psoriasis therapies should be avoided during acute hepatitis B until the infection could be brought under control by antiviral therapy [4].
There is no vaccine against hepatitis C (HCV), but antiviral drugs can cure 90% of those treated [8]. Methotrexate is contraindicated in HCV because of its hepatotoxic potential and tendency to promote viral replication [4]. Bonifati et al. recommend monitoring liver enzymes and HCV viral load every 3-6 months and, if necessary, consider interdisciplinary collaboration with hepatology [9].
Literature:
- Kaushik SB, Lebwohl MG: Psoriasis: which therapy for which patient: J Am Acad Dermatol 2019; 80(1): 43-53.
- Zachoval R: Prevention of hepatitis B reactivation, Hepatitis &more 1/2017.
- Lockwood SJ, Prens LM, Kimball AB: Karger Compass Dermatol 2017; 5: 195-199. DOI: 10.1159/000481335, www.karger.com/Article/Pdf/481335
- AWMF 2017, www.awmf.org/uploads/tx_szleitlinien/013-001l_S3_Therapie_Psoriasis-vulgaris_2017-12.pdf
- Patterson AT: JAAD 2020; 82(2): 532.
- Perez-Alvarez R, et al: Medicine (Baltimore) 2011; 90: 359-371.
- Ting S-W, Chen Y-C, Huang Y-H. Clin Drug Investig 2018, doi:10.1007/s40261-018-0671-z.
- Federal Office of Public Health Switzerland (FOPH): www.bag.admin.ch
- Bonifati C, Lora V, Graceffa D, Nosotti L: World J Gastroenterol 2016; 22: 6444-6455.
- EADV: Kirby B: Psoriasis treatment, slide presentation, Professor Brian Kirby, MD FRCPI, EADV Congress, Madrid, Oct. 12, 2019.
DERMATOLOGY PRACTICE 2020; 30(3): 26