
Screening programs are increasing the incidence of early-stage lung cancer. Surgery is still the first choice of therapy. With thorough lymphadenectomy, anatomic segmental resection is an equivalent alternative to lobectomy.
Lung cancer is the second most common cancer in Switzerland, with an incidence of 11.9% in men and the third most common in women, with an incidence of 8.7%. The mortality rate is the highest in men (21.9%) and the second highest in women (15.4%), and the trend is upward [1]. This is mainly due to the fact that the initial diagnosis is often made at an advanced and prognostically poor stage. That’s why early detection programs have come to the fore.
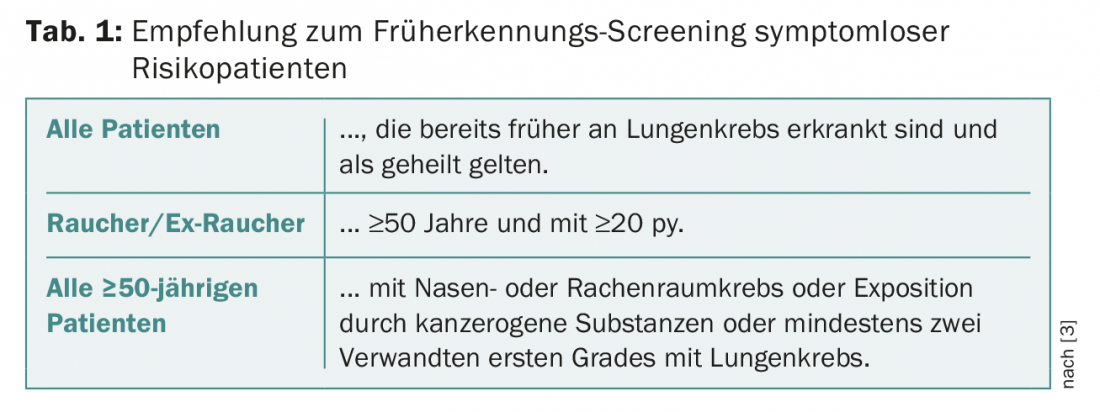
I-ELCAP (International Early Lung Cancer Action Program), the international program for the early detection of lung cancer, has been in existence since 1992. In Switzerland, the National Lung Cancer Screening Program is part of the I-ELCAP and is implemented by the Foundation for Lung Diagnostics, established in 2011 [2]. The most important tool of this screening program is to perform a “low-dose” CT scan on high-risk patients without symptoms such as cough, hemoptysis, dyspnea, hoarseness, dysphagia, or chest pain. This includes all patients who have had lung cancer previously and are now considered cured, all smokers over 50 years of age, and ex-smokers with at least 20 packyears (py). In addition, all patients over 50 years of age who already have tumors of the nose and throat or who are exposed to carcinogenic substances (asbestos, passive smoke, chromium, arsenic, etc.) or who have at least two first-degree relatives suffering from lung cancer (Table 1) [3].
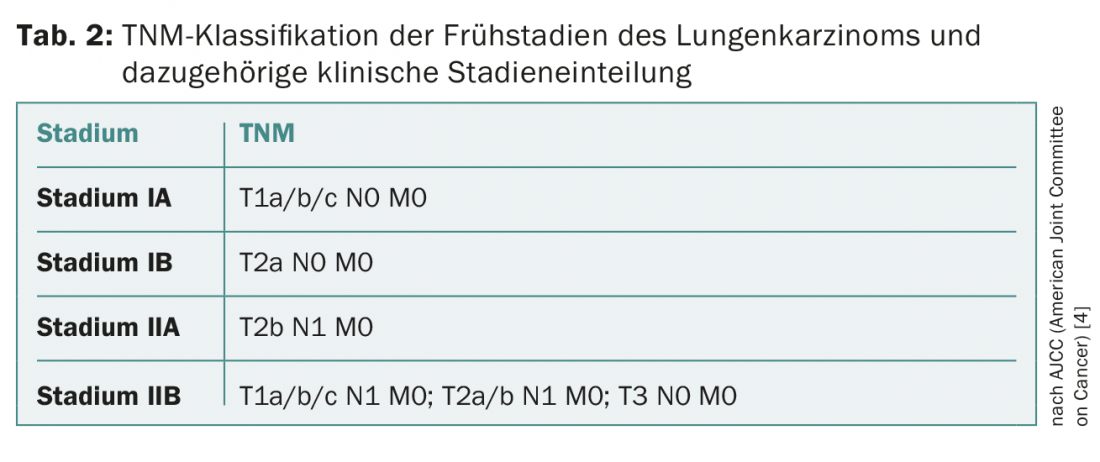
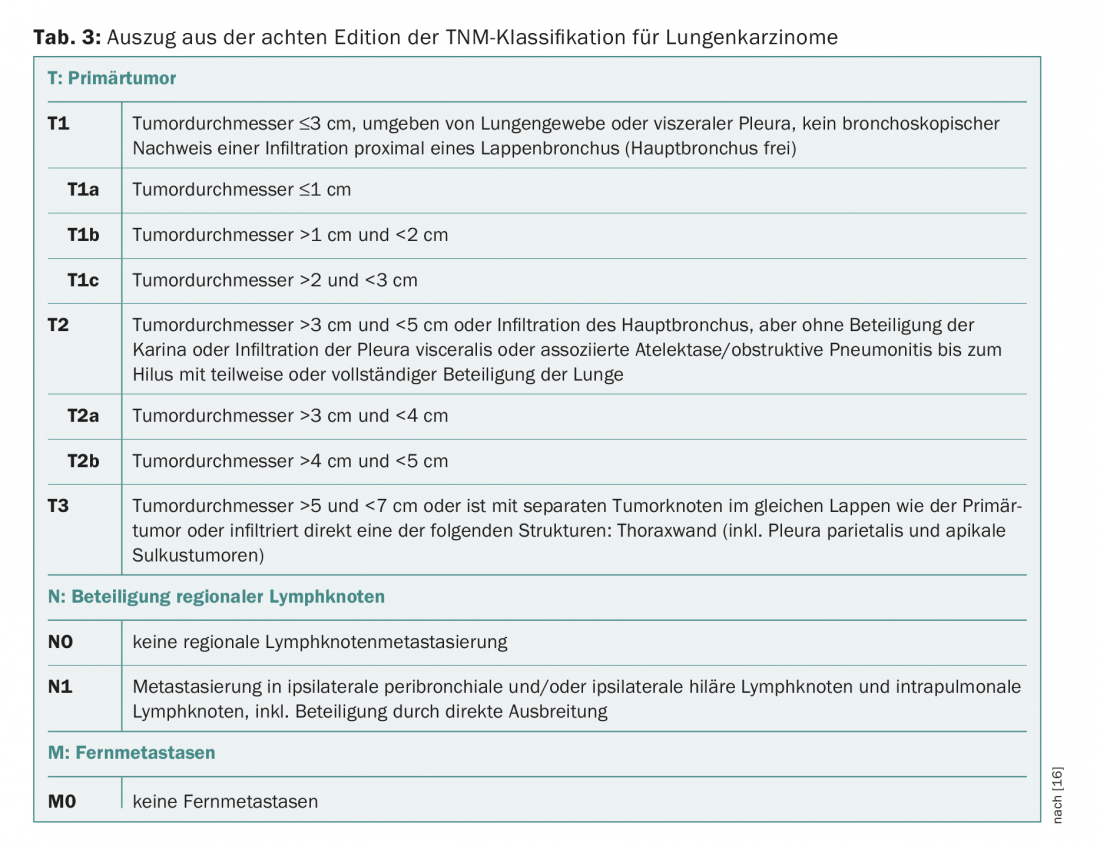
If non-small cell lung cancer (NSCLC) is suspected as part of this screening program, further investigations such as bronchoscopy with EBUS and PET-CT are performed. The findings obtained in this process are used for classification in the TNM (“tumor node metastasis”) classification. Depending on the TNM stage, the clinical stage is IA, IB, IIA, IIB, IIIA, IIIB or IV, classified according to the eighth edition of the AJCC.
Since this article is intended to focus on the treatment of early stages of lung cancer, we will limit ourselves below to an overview of stages IA, IB, IIA, and IIB and their associated TNM classification (Table 2 and 3).
Therapy options
Based on this staging, further therapeutic steps can now be planned within the framework of the obligatory interdisciplinary tumor board. There are two different treatment options for early stages I and II: Surgical and non-surgical or radiotherapy. To make a decision between these two, examinations such as pulmonary function tests, ergometry and, in critical cases, spiroergometry in combination with perfusion scintigraphy are performed to assess the patient’s general condition. It is recommended that the ESMO guidelines be followed in this regard [4].
Radiotherapy
Radiotherapy is recommended for patients who are not suitable for surgical options due to comorbidities or impaired lung function (postoperative FEV1 minimal <1 liters). Within this spectrum of therapies are stereotactic radiotherapy (SBRT), stereotactic ablation radiotherapy (SABR), and radiofrequency ablation (RFA).
Although radiotherapy has gained significantly in precision and accuracy in recent years due to technical progress, it has an important disadvantage in addition to the known side effect profile: Treatment is based only on clinical staging without pathoanatomical confirmation or diagnostic confirmation. Consider that clinical staging is often incorrect and clinical stage often does not correspond to pathologic stage [5]: Occult affected lymph nodes are found in 11-14% of cases and are not detected with radiotherapy alone [6]. Without surgical resection and lymph node sampling or radical lymphadenectomy, these patients are not properly staged and, accordingly, are underserved therapeutically. Therefore, surgery remains the agent of first choice for NSCLC patients in an operable general condition.
Surgery
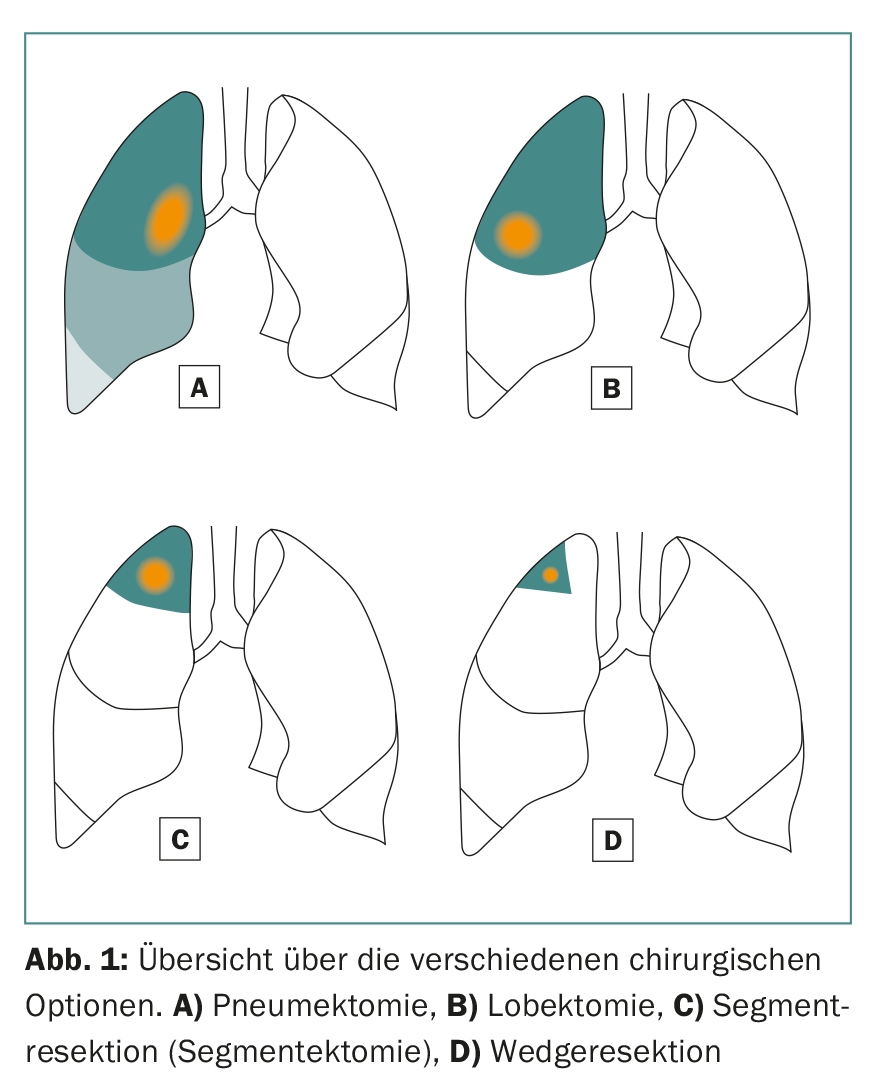
Surgical options include lobectomies and sublobar resections (anatomic segment resection and wedge resection) (Fig. 1) . In general, a minimally invasive (VATS) or open approach (thoracotomy) is chosen depending on tumor location and intraoperative conditions. In our own patient population, a minimally invasive technique is chosen in a good 70% and thus offers therapeutic options for patients with reduced general condition at best.
In lobectomy, as the name implies, at least one entire lobe of the right or left lung is removed. This is recommended for tumors larger than 3 cm. This procedure also has a major disadvantage: a lot of healthy, vital lung tissue is lost in the process.
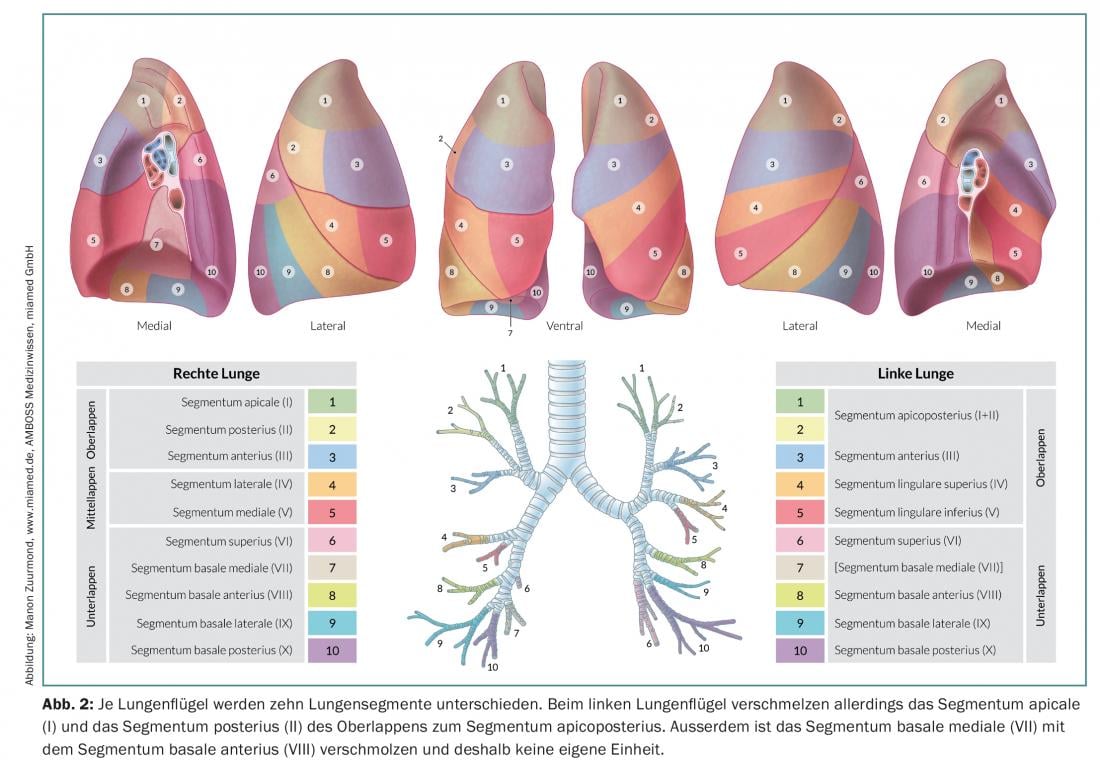
Anatomic segment resection (segmentectomy) resects individual lobes or up to three segments (trisegment resection) of individual lobes, which allows much more vital lung tissue to be preserved than lobectomy. This is particularly important for patients with impaired lung function or for possible further resections in case of a second or third primary lung carcinoma [7]. To perform a successful anatomical segment resection, it is important for the surgeon to know the exact anatomical relationships, i.e., the lung and its division into ten or nine segments per lung (Fig. 2).
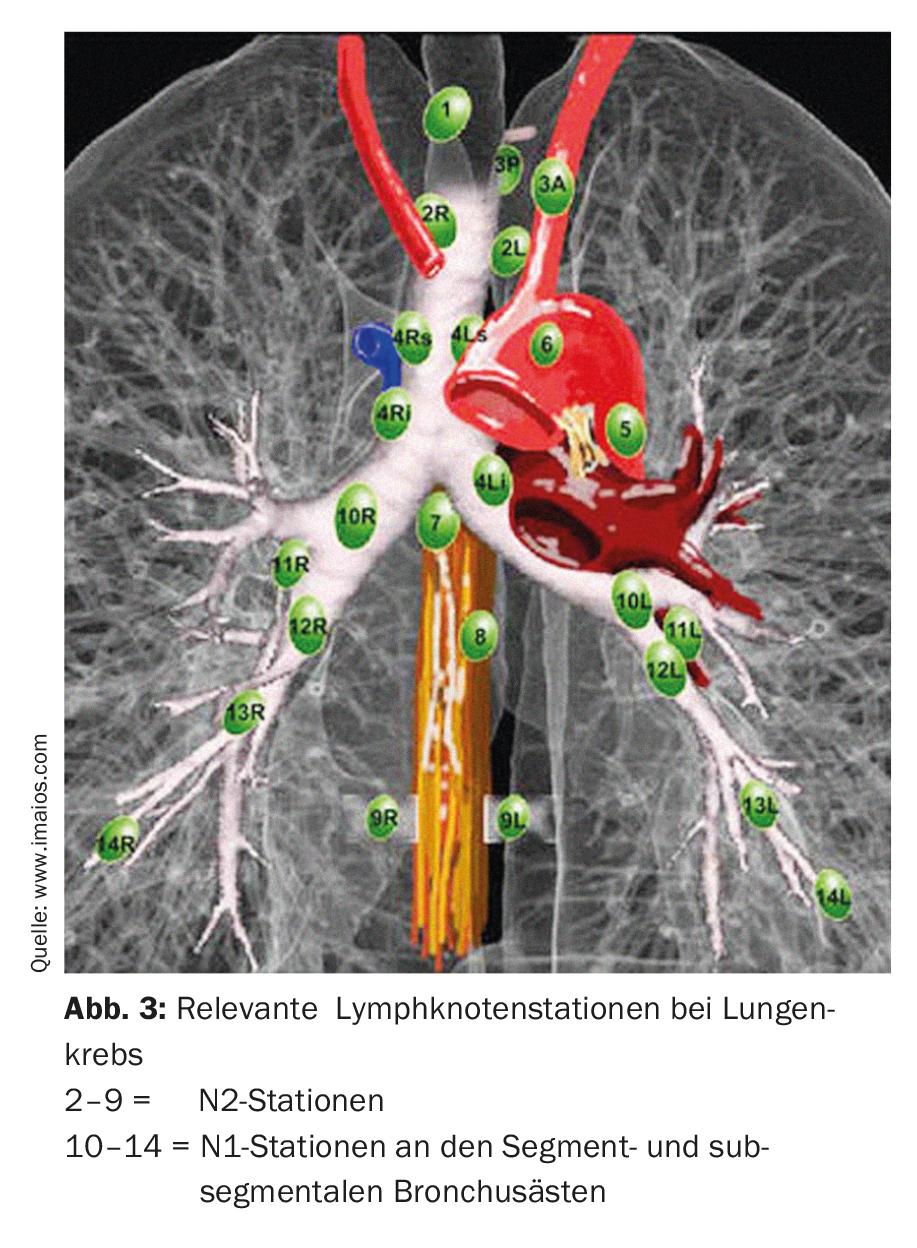
Depending on tumor location and size, a decision is made between segmentectomy or lobectomy. In all cases, it is important to confirm N0 status with a thorough mediastinal lymph node dissection (from the hilus to the segmental and subsegmental bronchus branches) with frozen section analysis. If intraoperative N1 or N2 involvement is evident, surgical therapy must be changed immediately and a completion lobectomy with radical lymphadenectomy must be performed. The patient’s age and general condition must also be taken into account. In addition, the surgeon must know the prognostic factors for the surgical treatment of NSCLC. According to current knowledge, the following factors are independent prognostic factors (weighted by importance) [8]:
- Number of affected lymph node stations
- Grading and histological differentiation
- Lymphangioinvasion in definitive histology
- Total number of affected lymph nodes
- Response to neoadjuvant therapy
- Sex and age of the patient
- Tumor size.
If a patient has undergone segment resection and is found postoperatively to have many of the aforementioned prognostic risk factors, a completion lobectomy in the sense of a second procedure is necessary and additive chemotherapy should be discussed in the tumor board.
Comparison of lobectomy vs. segmentectomy and lymphadenectomy
In the past, there have been several discussions as to whether anatomic segmental resection could replace lobectomy as the gold standard for the treatment of stage IA carcinomas. The greatest advantage of anatomic segmentectomy is the ability to resect the tumor while preserving the patient’s functional reserve, which may also primarily displace nonsurgical options as a treatment for lung cancer in patients with low lung function. Previous studies showed worse survival rates with sublobar resection compared with lobectomy [9]. However, it should be noted that non-anatomic and anatomic resections were grouped together in these studies and that the data collection is now 25 years old.
From previous studies, increasing numbers of resected lymph nodes are associated with a survival benefit: Ludwig et al. showed that the survival benefit peaked at 13-16 resected lymph nodes, and Gulack et al. found similar results (eleven resected lymph nodes) [10,11].
A recent paper by Stiles et al. investigated the role of lymphadenectomy in stage IA NSCLC and was able to show a significant advantage for long-term survival and local recurrence-free survival in patients with sublobar resection (segmentectomy or wedge resection) and lymphadenectomy compared to sublobar resection without lymphadenectomy [12].
Thus, if sublobar resection is chosen, systematic lymphadenectomy is critical for postoperative outcome and long-term survival.
Radiotherapy vs. surgery
Radiotherapy may be considered the procedure of choice in cases of stage I and II lung cancer in patients who are not candidates for surgical resection because of comorbidities or reduced lung function.
The most weighty disadvantage of radiotherapy is the fact that no histologic diagnosis is available before the therapeutic decision is made and no staging lymphadenectomy is performed. This can be fatal for the patient’s health future, because clinical and pathological stage diverge, as shown in a study of almost 3000 patients by López-Encuentra et al. showed. There, the concordance was only 47% [5]. Occultly affected lymph nodes are not detected during stereotactic ablation, although, as mentioned above, these are present in 11-14% of cases [6]. This results in the assignment of an incorrect TNM and ultimately an incorrect clinical stage.
On the other hand, today almost all early stages are treated surgically with minimally invasive methods (with thoracoscopy and/or robot-assisted procedures). Histology is always obtained, and anatomic segmental resection and N1/N2 lymphadenectomy are systematically performed. In addition, intraoperative rapid diagnostics (primary tumor and lymph nodes) provide the opportunity to adjust the optimal therapeutic strategy during the same anesthesia – if necessary (extension of resection in case of lymph node involvement). This will also provide all relevant and prognosis-determining factors for the postoperative procedure and the re-presentation at the tumor board, which is completely lacking in stereotactic ablative radio procedures.
Postoperative procedure
If definitive histology reveals T1a/b/c N0 M0 or T2a N0 M0 and, accordingly, stage IA or IB, no further adjuvant therapies are recommended. Physical examinations and “low-dose” CT scans at six-month intervals during the first two postoperative years are included as follow-up. Thereafter, the checks are carried out annually. From stage II onwards, options for adjuvant therapy should be discussed in the context of an interdisciplinary tumor board [13].
Adjuvant therapies
Cisplatin-based therapies have been shown to be successful adjuvant agents in terms of long-term survival in stage II in three clinical trials. For stage I patients, these benefits could not be shown; on the contrary, adjuvant chemotherapy proved to be rather harmful here [14].
Newer systemic therapies such as targeted cancer therapy with monoclonal antibodies are currently not established outside of clinical trials. Currently, several randomized clinical trials are evaluating the role of EGFR- or ALK-targeted therapies in the adjuvant setting for EGFR- or ALK-positive patients, respectively. To date, there is evidence that patients with EGFR mutations have longer relapse-free survival with erlotinib. However, it is not yet clear whether this also increases long-term survival or whether only the time to recurrence is prolonged.
Postoperative radiotherapy is recommended only in cases in which an R0 situation could not be created surgically [15].
Summary
In recent years, more and more early-stage lung cancers have been diagnosed as part of screening efforts. Depending on the clinical stage and general condition of the patient, a treatment decision between radiotherapy and surgery must be thoroughly weighed. Surgery remains the first-line treatment for the early stages of NSCLC. In this field, with increasing experience and expertise, anatomic segmental resection with complete lymphadenectomy is becoming more and more important due to its anatomic accuracy and preservation of the patient’s functional reserve. It is an equivalent alternative to lobectomy and a better therapy compared to radiotherapy if the lymphadenectomy is thorough enough.
Take-Home Messages
- Screening programs are increasing the incidence of early stages of lung cancer. Mortality can be significantly reduced as a result.
- The 5-year survival rate could be increased from the current level of approximately 17% (all lung cancer stages) to over 50%.
- Surgery remains the first choice for treatment of early stages of lung cancer, with appropriate expertise on the part of the surgeon
- almost three quarters of all procedures can be performed using the latest minimally invasive techniques.
- Anatomic segment resection is ideally suited for resection in patients with impaired lung function because of the sparing of vital lung tissue.
- With appropriate thoroughness of lymphadenectomy, anatomic segmental resection is an equivalent alternative to lobectomy.
- Stereotactic radiotherapy and other ablative procedures are second-line procedures because of the usual lack of pathoanatomic diagnostic confirmation.
Literature:
- Krebsliga: Cancer in Switzerland: important figures. 2016. www.krebsliga.ch/ueber-krebs/zahlen-fakten/-dl-/fileadmin/downloads/sheets/zahlen-krebs-in-der-schweiz.pdf.
- I-ELCAP: Foundation for Lung Diagnostics. %C3%diagnostics.
- Foundation for Pulmonary Diagnostics: Frequently Asked Questions. www.lungendiagnostik.ch/index.php/haufige_fragen.html.
- Vansteenkiste J, et al: 2nd ESMO Consensus Conference on Lung Cancer: early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann Oncol 2014; 25(8): 1462-1474.
- López-Encuentra A, et al: Comparison between clinical and pathologic staging in 2,994 cases of lung cancer. Ann Thorac Surg 2005; 79(3): 974-979.
- Stiles BM, et al: Point: Clinical stage IA non-small cell lung cancer determined by computed tomography and positron emission tomography is frequently not pathologic IA non-small cell lung cancer: the problem of understaging. J Thorac Cardiovasc Surg 2009; 137(1): 13-19.
- Hattori A, et al: Oncological outcomes of sublobar resection for clinical-stage IA high-risk non-small cell lung cancer patients with a radiologically solid appearance on computed tomography. Gen Thorac Cardiovasc Surg 2016; 64(1): 18-24.
- Schöb O: Surgical therapy for lung cancer. Staging, operability, and prognostic factors determine the indication. InFo ONCOLOGY & HEMATOLOGY 2015; 3(1): 13-17.
- Ginsberg RJ, et al: Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Ann Thorac Surg 1995; 60(3): 615-622.
- Ludwig MS, et al: Postoperative survival and the number of lymph nodes sampled during resection of node-negative non-small cell lung cancer. Chest 2005 Sep; 128(3): 1545-1550.
- Gulack BC, et al: The Impact of Tumor Size on the Association of the Extent of Lymph Node Resection and Survival in Clinical Stage I Non-Small Cell Lung Cancer. Lung Cancer 2015; 90(3): 554-560.
- Stiles BM, et al: The importance of lymph node dissection accompanying wedge resection for clinical stage IA lung cancer†. Eur J Cardiothorac Surg 2017; 51(3): 511-517.
- No authors listed: Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. Non-small Cell Lung Cancer Collaborative Group. BMJ 1995; 311(7010): 899-909.
- Pignon JP, et al: Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol 2008; 26(21): 3552-3559.
- Wang EH, et al: Postoperative Radiation Therapy Is Associated With Improved Overall Survival in Incompletely Resected Stage II and III Non-Small-Cell Lung Cancer. J Clin Oncol 2015; 33(25): 2727-2734.
- Thomas KW, Gould MK: Tumor, node, metastasis (TNM) staging system for non-small cell lung cancer. UpToDate 2017 Jan 16.
InFo ONCOLOGY & HEMATOLOGY 2017; 5(3): 8-12.









