
Haglund’s heel (Haglund’s exostosis) is a ganglion at the upper edge of the heel bone. Dorsal calcaneal spur is an ossification of the attachment of the Achilles tendon to the calcaneus. Due to the pressure of the bony process in the shoe, inflammation or swelling of the soft tissues such as the bursa often occurs. While heel spurs and Haglund’s heel can be differentiated radiographically, inflammations of the Achilles tendon can be detected sonographically in particular.
The calcaneus is the bone of the human body where most bone spurs form. Plantar calcaneal spur has already been reported. Analysis of 1027 lateral heel radiographs showed that plantar than dorsal calcaneal spurs were slightly more common (11.2% versus 9.3%) [1]. With increasing age, productive fibroostitis manifests at both sites. The distribution on the right and left is about the same. Females are significantly more likely to have plantar spurs than males; in contrast, they are more common dorsally in males than in females over the age of 70. It is also interesting to note that with increasing age and increasing frequency of osteoarthritic changes in the limb joints, the incidence of calcaneal spurs increases even further [2].
Symptomatology is load- and movement-dependent, and local pain can be provoked on clinical examination when pressure is applied. In Haglund’s heel, mechanical irritation also often occurs due to footwear. The possible differential diagnoses in dorsal (also upper) symptomatic calcaneal spur are shown in review 1 [3].
Haglundexostosis and dorsal calcaneal spur must be differentiated with regard to localization. The spur is located more caudally (Fig. 1A). The local symptomatology is about 2 to 3 cm caudal to the Achilles tendon, and the Achillodynia is about 3 to 5 cm cranial to the tendon insertion at the calcaneus. While in Haglund’s heel (Fig. 1B) a mechanical irritation of the adjacent tissue causes the discomfort, the heel spur results from excessive traction of the Achilles tendon, often as a consequence of shortening of the calf muscles.

Therapeutically, conservative measures such as offloading, analgesic and antiphlogistic drug treatment, cryotherapy and special cushioning insoles dominate. Orthovolt therapy [4] has an analgesic effect in more than 80% (6 × 0.5 Gray within 3 weeks).
X-rays in lateral projection can differentiate heel spurs and Haglund’s heel, but say nothing about the inflammatory process. Sonographically, inflammation of the Achilles tendon can be detected well. Computed tomographic examinations with the sagittal 2D reconstruction lead to similar information as the X-ray image. However, with regard to the statement about inflammatory soft tissue activities, the method also has clear limitations. Magnetic resonance imaging can underestimate the extent of the spurs, but local accompanying changes such as bursitis, tendinitis or spongiosa edema are excellently visualized. Thus, in more than 85% of patients with Haglund’s exostosis, Haglund’s syndrome can be verified with bursitis and tendinitis of the Achilles tendon [5].
Case studies
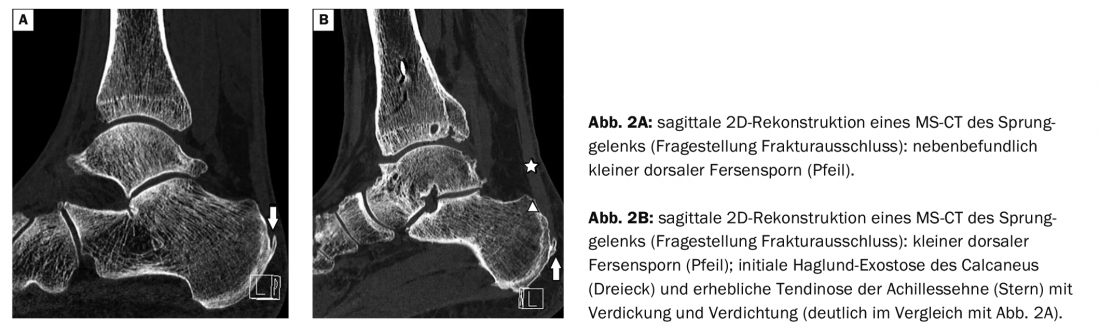
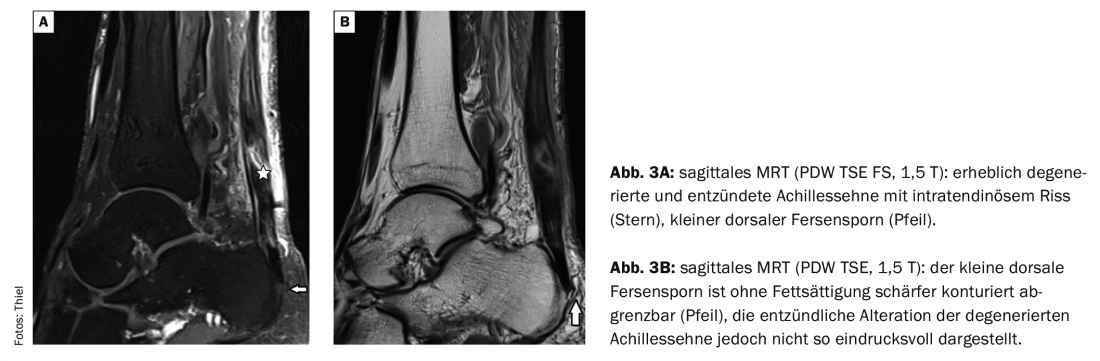
Case report 1 shows a lateral radiograph (Fig. 1A) of a 57-year-old man with dorsal pain symptoms provocable by dorsiflexion of the foot, a powerful dorsal calcaneal spur, and a small plantar. The radiograph of a 54-year-old female patient with upper heel pain shows a Haglund’s heel with corresponding Haglund’s syndrome (Fig. 1B) . Calcification of the distal Achilles tendon suggests advanced tendinosis with chronic recurrent tendinitis. In the image examples (2A, B) in case 2. of two men aged 48 respektvie 59 years, a small dorsal calcaneal spur is delineable in each case on CT (other question, fracture exclusion), also an initial haglund exostosis (Fig. 2B) and tendinosis of the Achilles tendon. Case report 3 (Fig. 3A,B) documents MR-tomographically a considerable degeneration and tendinitis of the Achilles tendon of a 54-year-old man (long-time endurance athlete, strain after overstretching of the tendon), the small heel spur is more difficult to delimit in the MRI than in the CT.
Take-Home Messages
- Radiographs laterally can demonstrate dorsal calcaneal spurs very well, but do not capture the often accompanying inflammatory soft tissue changes in the acute stage.
- Dorsal pain symptoms may be very similar in dorsal calcaneal spur and Haglund’s heel, but localization may differ.
- Computed tomography is superior to MRI in delineating bony contours.
- Inflammatory bony and soft tissue changes are very easy to identify on MRI, and intravenous application of Gd-DTPA may be diagnostically useful.
Literature:
- Riepert T, et al: The incidence, age dependence and sex distribution of the calcaneal spur. An analysis of x-ray morphology in 1027 patients of the central European population. Rofo 1995; 162(6): 502-505.
- Weiss E: Calcaneal spurs: examining etiology using prehistoric skeletal remains to understand present day heel pain. Foot (Edinb) 2012; 22(3): 125-129.
- Orthopaedic Joint Clinic: www.gelenk-klinik.de (last accessed 07.06.2021).
- Muecke R, et al: Low-dose radiotherapy for painful heel spur. Retrospective study of 117 patients. Strahlenther Onkol 2003; 179(11): 774-778.
- Debus F, et al: MRI in patients with Haglund’s deformity and its influence on therapy. Arch Ortop Trauma Surg 2019; 139(7): 903-906.
HAUSARZT PRAXIS 2021; 16(7): 38-39









