
Lesions of the Achilles tendons are among the most common tendon pathologies. In addition to excessive forefoot pronation and Haglund deformity, predisposing factors include certain sports and certain pre-existing conditions such as rheumatoid arthritis, systemic lupus erythematosus, diabetes mellitus, and arthritis urica. Acute Achilles tendon rupture is triggered by forced dorsiflexion of the foot against the contracting force of the gastrocnemius muscle. As a result of incomplete ruptures, fibromatous degenerative tendinosis often occurs.
The Achilles tendon is the strongest tendon of the human body. The transverse diameter is usually 6 mm. It has no tendon sheath and is the tendon with the most frequent lesions [1]. Inflammatory degenerative changes are classified in Overview 1 .
The inflammatory changes can occur in systemic diseases of the rheumatic type or be the result of incorrect or excessive strain. The mucoid hypoxic degeneration leads to thickening of the tendon, magnetic resonance imaging inhomogeneous structure and biconvex contour change. It is the most common cause of spontaneous rupture. Not all degenerative changes of the tendon are symptomatic [2]. However, the inflammatory reactions lead to local pain in the distal tendon area, swelling and limited weight-bearing capacity. Tendinosis and tendinitis can be treated conservatively, including small tears of the tendon. Consistent unloading, stabilization, and antiphlogistic therapy lead to proliferation and remodeling of tendon tissue after an initial inflammatory phase [3]. Ruptures of the Achilles tendon are associated with a loss of heel elevation function and are usually found about 3 to 5 cm cranial to the insertion at the calcaneus. Middle-aged men are more frequently affected depending on the level of athletic activity [4]. Minimally invasive surgical treatment produces functionally good results and significantly reduces postoperative complications.
Radiographs are very limited in detecting degenerative and inflammatory changes of the tendon, even ruptures are not detectable. Sonographically, inflammations of the Achilles tendon can be detected well, also ruptures with detectable loss of continuity [1]. Tendinosis can be quantified sonographically [5] (overview 2). Computed tomographic examinations can visualize tendinosis and inflammation associated with structural compression or widening of the tendon cross-section. Magnetic resonance imaging is the method of choice in the detection and differential diagnosis of Achilles tendon lesions. Inflammatory changes of the tendon itself, peritenonitis, and concomitant bursitis are safely visualized. MRI is also excellent for documenting healing progressions [1,6].
Case studies
Localized pain of the distal Achilles tendon was present in all demonstrated cases. Various causes led to the symptomatology; in the case of the tendon rupture, there was a complete restriction of the pulling effect of the tendon on the calcaneus.
Case report 1 shows a not-so-fresh contusion trauma of the Achilles tendon in a 56-year-old patient with extensive, partially organized hematoma dorsal to the tendon (Fig. 1) . Depending on the severity of the contusion and the condition, the tendon may remain intact, as in this case. In the case 2 , a short-stretch intratendinous tear (Fig. 2A and B) also occurred in an already significant tendinosis, and the 65-year-old patient had load-dependent pain. Case report 3 demonstrates a Haglund’s syndrome with Haglund’s exostosis, marked bursitis subachillea and minor tendinitis of the Achilles tendon (Fig. 3). The weight-bearing capacity and movement of the foot of the 48-year-old patient was painfully limited, and there was also considerable local pressure pain.
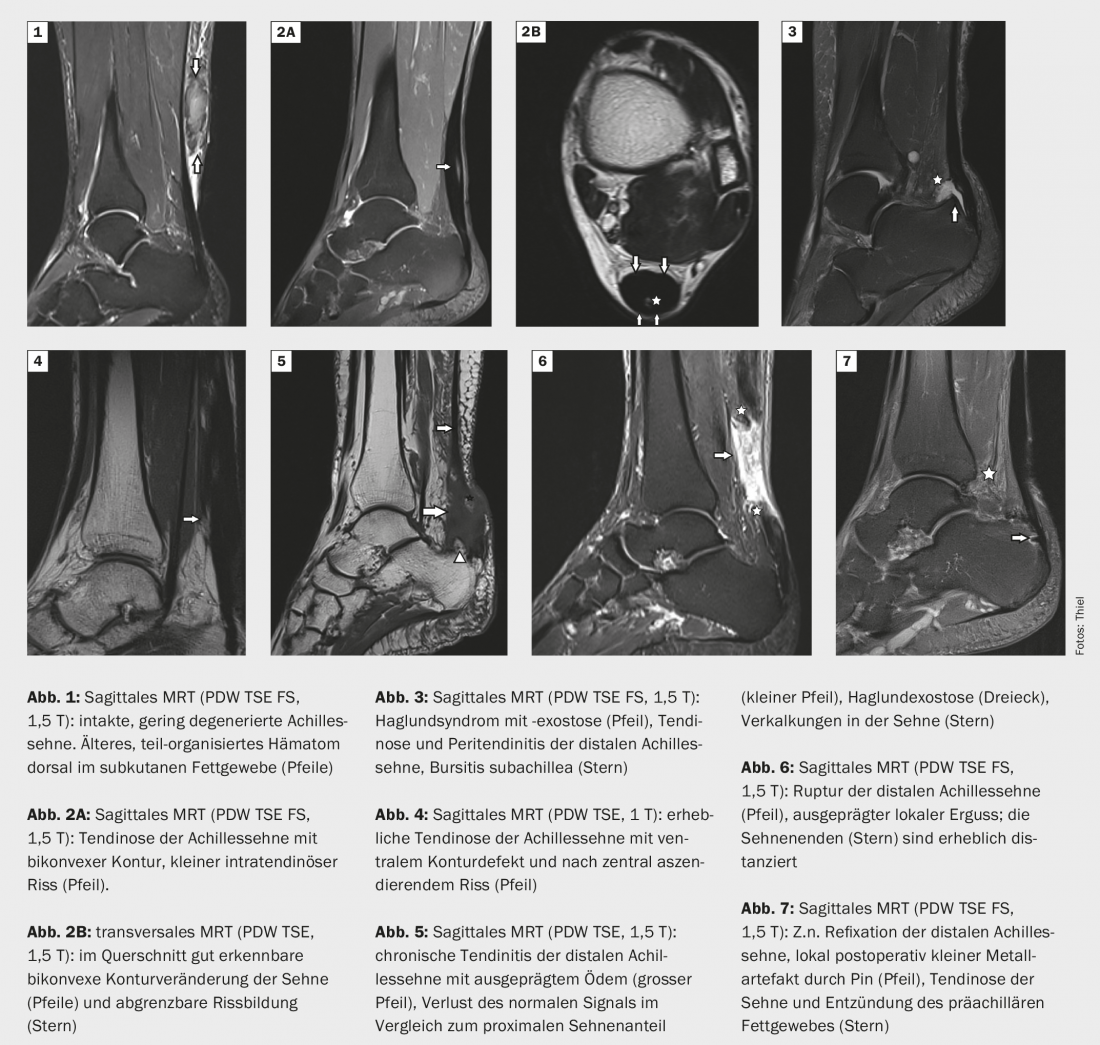
Significant tendinosis with ventral oblique partial tear (Fig. 4) is found in case 4, and tendinosis and chronic attachment tendinitis of the Achilles tendon with Haglund’s exostosis (Fig. 5) is present in case 5. Case 6 demonstrates a long-stretch rupture of the Achilles tendon loco typico (Fig. 6) in the case of significant degeneration and concomitant inflammation of the plain bearing, Case 7 a postoperative condition with refixation of the tendon at the calcaneus. (Fig. 7).
Take-Home Messages
- The Achilles tendon is the strongest tendon in humans and also the tendon with the most frequent pathological changes.
- Athletically active middle-aged men are particularly frequently affected by tendon ruptures.
- Diagnostically, sonography and MRI are leading in the detection of degenerative and inflammatory changes as well as ruptures.
- Tendinosis and tendinitis of the Achilles tendon can be treated conservatively; minimally invasive reconstructive surgical techniques are becoming established for ruptures.
Literature:
- Weishaupt D, Zanetti M: Radiological diagnostics of the foot. Radiology up2date 2002; 3: 237-257.
- Splittgerber L, Ihm JM: Significance of Asymptomatic Tendon Pathology in Athletes. Curr Sports Med Rep 2019; 18(6): 192-200.
- Thomopoulos S, et al: Mechanisms of tendon injury and repair. J Orthop Res 2015; 33(6): 832-839.
- Maffulli N, Via AG, Oliva F: Chronic Achilles Tendon Rupture. Open Orthop J 2017; 31(11): 660-669.
- Schueller-Weidekamm C: Sonography of the musculoskeletal system. Radiology up2date 2009; 1: 15-29.
- Breitenseher M: The MRI trainer. Lower extremity. Stuttgart, New York: Georg Thieme Verlag 2003; 66-71.
HAUSARZT PRAXIS 2021; 16(8): 32-33









