It was almost a sensation when the Pfizer company launched sildenafil, originally intended as an active ingredient for coronary heart disease, as a drug for erectile dysfunction in 1998. Sildenafil soon conquered the world market and became one of the most prescribed drugs.
The huge success of sildenafil and the other active ingredients against ED pushed the demand and promotion of natural preparations against erectile dysfunction somewhat into the background. However, such preparations have not completely disappeared, which has several reasons. The high price of phosphodiesterase-5 inhibitors certainly plays a role, and the possible side effects of sildenafil and co. may also contribute.
Unfortunately, the black market prices a large number of dubious preparations, which are unfortunately used again and again. A sad example of this is rhino horn powder, which is persistently used in China, although its ineffectiveness should have been known for a long time!
Phytotherapy
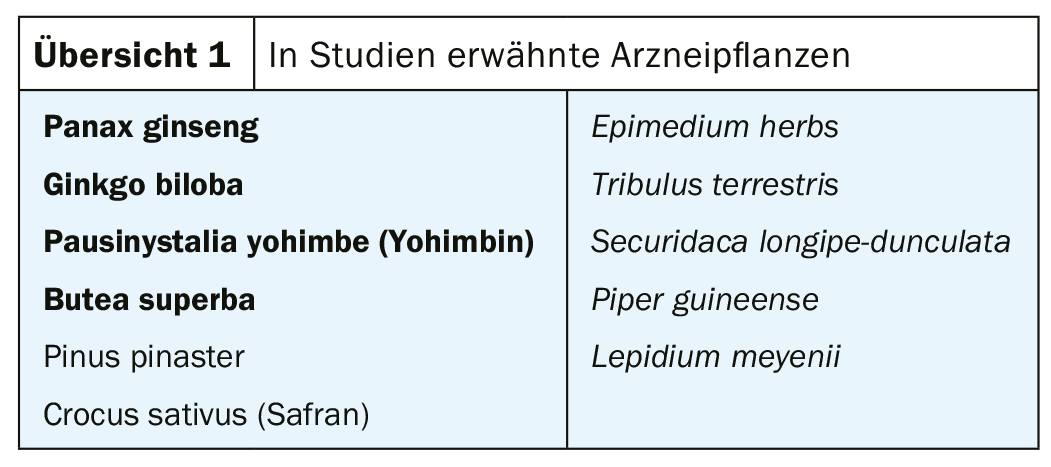
It must be stated in advance that there is no medicinal plant which has an effect against erectile dysfunction comparable to the PDE-5 inhibitors! However, a few studies have been published that report on medicinal plants repeatedly mentioned in folk medicine, to which a certain efficacy is attributed (overview 1).
Published, clinical or pharmacological studies report on the four medicinal plants in bold in the overview 1 and document some efficacy. Such studies are mentioned in the sequel. The other four medicinal plants are mentioned in publications without corresponding results suggesting that their use makes sense.
Panax ginseng: Known to have adaptogenic activity, Panax ginseng appears to be the only medicinal plant for which studies document fairly clear efficacy against ED. In recent years, a CRT and a meta-analysis have been published [1,2]. CRT determined significant efficacy of berry extract of Panax ginseng (4× 350 mg/day for 8 weeks) against mild to moderate ED. Note that this study used berries and not roots as usual. Meta-analysis also reports good efficacy of Panax ginseng against ED.
Ginkgo biloba: The Ginkgo biloba extract EGb761®, which is well known against cognitive disorders, is also said to have a possible efficacy against erectile dysfunction, which can be inferred from a pharmacological study [3]. High doses of EGb 761® produced significant improvement in rats with experimentally induced ED compared to the control group.
Butea superba: Butea superba, Plosso tree, a tree native to Asia and Southeast Asia, was reviewed in a randomized, placebo-controlled, double-blind study in subjects with an ED. The verum group received 250 mg of powdered tuber of Butea superba twice daily for three months. This treatment showed appreciable improvement in ED in 82% of subjects.
Pausinystalia yohimbe (yohimbine): A meta-analysis published in 1998 [4] examined 7 studies and concluded that yohimbine is superior to placebo for the treatment of ED. Yohimbine is an indole alkaloid derived from the tree Pausinystalia yohimbe, native to tropical West Africa. In Germany there is a prescription drug, tablets with 5 mg yohimbine.
Summary
There are some medicinal plants for which studies indicate some efficacy against erectile dysfunction. Panax ginseng is the most important of these. However, the effectiveness cannot be compared with modern, synthetic agents such as sildenafil or tadalafil.
Literature:
- Choi YD, et al: Effects of Korean ginseng berry extract on sexual function in men with erectile dysfunction: a multicenter, placebo-controlled, double-blind clinical study, Int J Impot Res 2013(2); 25: 45-50.
- Borelli F, et al: Herbal Dietary Supplements for Erectile Dysfunction: A Systematic review and Meta-Analyses, Drugs 2018(6); 78: 643-673.
- Wu YN, et al: Effect of Ginkgo biloba extract (EGb 761) on Recovery of Erectile Dysfunction in Bilateral Cavernous Nerve Injury Rat Model, Urology 2015(5); 85: 1214.47-15.
- Ernst E, Pittler MH: Yohimbine for erectile dysfunction: a systematic review and meta-analysis of randomized clinical trials, J. Urol. 1998(2); 159: 433-436.
HAUSARZT PRAXIS 2019; 14(9): 8